Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
100 Cards in this Set
- Front
- Back
|
What is the range of caries severity on radiographs?
|
R1-R4
|
|
|
Which is worse, R1 or R4?
|
R4
|
|
|
Enamel caries less than half through enamel
R1, 2, 3 or 4? |
R1
|
|
|
Enamel caries at least half through enamel but NOT involving DEJ
R1, 2, 3 or 4? |
R2
|
|
|
Caries through DEJ but less than half way through dentin?
R1, 2, 3 or 4? |
R3
|
|
|
Caries more than half way through dentin to pulp
R1, 2, 3 or 4? |
R4
|
|
|
What classification (R1, 2, 3 or 4) describes incipient caries?
|
R1
|
|
|
What area of the tooth are caries most common?
|
occlusal surface
|
|
|
What type of caries are more common in kids and adolescents in posterior teeth?
|
occlusal caries
|
|
|
True or False, irregularities of pits and fissures of teeth can make someone more inherently prone to occlusal caries
|
True
|
|
|
Occlusal caries have a triangle shape in the enamel. The "base" of the triangle is towards the dentin or the outer surface?
|
towards dentin
|
|
|
When are occlusal caries visible on a radiograph?
|
when it reaches DEJ
|
|
|
True or False, radiographs are a solid way to diagnose occlusal caries
|
False, you'll catch it too late
|
|
|
Why are occlusal caries often invisible on radiographs?
|
they are "hidden" by surrounding enamel that don't allow the carious lesion to be detected due to a lack of contrast
|
|
|
Occlusal caries spread along what line?
|
DEJ
|
|
|
Occlusal caries are (RO/RL) line between enamel and dentin
|
RL (duh...)
|
|
|
When occlusal caries break through the DEJ, what pattern to they create as they spread further towards the pulp
|
spherical (remember, they were triangular shaped in the enamel, but once they pass the DEJ, they spread like a sphere)
|
|
|
How can occlusal caries eventually lead to collapse of enamel that was not initially diseased?
|
Caries invades dentin and basically carves out under the enamel, giving it little support. Then, you bite down and collapse the enamel in the area.
|
|
|
Radiographs can detect occlusal caries as a fine grey shadow under the ___
|
DEJ
|
|
|
Radiographs are only effective for occlusal caries once the caries reach the ___
|
dentin (or DEJ)
|
|
|
True or False, R1 occlusal caries are not typically visible on a radiograph
|
True (must hit dentin before they can be seen)
|
|
|
True or False, for occlusal caries, the enamel may appear intact even though there is clearly decay in the dentin
|
True! You only need a very small hole for caries to spread and widen into the dentin. Enamel might look normal!
|
|
|
For occlusal caries, you'll first notice a (narrow/wide) based RL zone in the dentin
|
wide
|
|
|
A band of increased opacity between lesion and pulp chamber in dentin is likely what?
|
reparative dentin
|
|
|
True or False, severe occlusal caries can be seen on radiographs only
|
False, radiographs AND visually (duh, they're "severe")
|
|
|
Interproximal caries develop (fast/slow)
|
slow
|
|
|
It takes __ years for interproximal caries to become clinically apparent
|
3-4years
|
|
|
What two areas do interproximal caries typically develop?
|
1. just below contact point
2. on enamel between contact point and height of free gingival margin |
|
|
Interproximal caries will appear chalky-white and rough. Explain both of these findings.
|
chalky-white due to demineralization of enamel, and rough for the same reason. Enamel breaks down and becomes rough and chalky.
|
|
|
interproximal caries in the enamel create a triangle shape. The 'base' of this triangle is (towards the dentin/ towards the outer surface)
|
towards the outer surface (this is OPPOSITE of direction in occlusal caries)
|
|
|
What % of demineralization is needed before caries are seen on a radiograph?
|
30-40%
|
|
|
Why are incipient caries hard to detect on a radiograph?
|
Not much demineralization so there's hardly any (if any at all) contrast for the X-ray to pick up on
|
|
|
True or False, incipient caries are like all other caries and must be restored
|
False! They can be reversed and remineralized
|
|
|
True or False, once a lesion is more than halfway through the enamel, it is no longer considered incipient
|
True (it's now an R2)
|
|
|
R3 caries are when the lesion has invaded what area?
|
dentin or past the DEJ (same thing)
|
|
|
Why can caries that spread to dentin still affect the enamel?
|
They can undermine the integrity of the enamel above it and lead to it's collapse
|
|
|
Once caries have spread more than half way through the dentin, they are called:
R1, 2, 3 or 4? |
R4
|
|
|
True or False, you can remineralize any lesion as long as it has not reached the DEJ
|
False! Once it gets halfway through the enamel, it's no longer incipient!
|
|
|
What type of caries appear as a dark thin RL line running through interproximal enamel into dentin, where the caries then spreads along DEJ?
|
Lamellar caries
|
|
|
True or False, because of the antimicrobial properties of the pulp, caries can technically never get all the way through the dentin to the pulp
|
False, I completely made that up. You're welcome.
|
|
|
True or False, if caries are severe enough to get into the pulp, you will know it from the radiograph
|
False, caries are always worse clinically than radiographically and if it has just reached the pulp, you may not be able to tell on radiograph alone
|
|
|
Occlusal caries are identifiable on a radiograph when they are:
R1 R2 R3 R4 |
R3 and worse (So R3 and R4 only...)
|
|
|
Why is it hard to detect caries interproximally of you have overlapping contacts?
|
The contacts may cover up a carious lesion and it won't show up
|
|
|
What is commonly misdiagnosed as caries around the gum line?
|
cervical burn out
|
|
|
What causes cervical burnout?
|
the area between neck of tooth and root absorb less xrays... not related to disease
|
|
|
On (posterior/anterior) teeth, cervical burnout is a RL triangle on proximal cervical neck
|
posterior
|
|
|
On (posterior/anterior) teeth, cervical burnout is a RL band across cervical neck of teeth
|
anterior
|
|
|
What type of treatment is needed if cervical burnout is detected?
|
Nothing
|
|
|
Why will cervical burnout sometimes show up or not show up in the same patient?
|
often depends on horizontal angulation
|
|
|
Facial and lingual caries are often seen as "___ ___"
|
black holes (most worthless flashcard ever)
|
|
|
The periphery of facial or lingual caries is often (poorly/well) demarcated
|
well
|
|
|
Cervical caries on the facial or lingual are often ___ shaped
|
crescent
|
|
|
Cemental caries are known by what two other names?
|
1. root caries
2. radicular caries |
|
|
cemental caries start near the ___
|
CEJ
|
|
|
Cemental caries are (poorly/well) defined
|
poorly
|
|
|
Cementum is relatively (more/less) resistant to caries
|
less
|
|
|
What is a common medical cause of root caries in elderly?
|
Xerostomia
|
|
|
Cementum can slowly be exposed due to what in elderly people?
|
gingival recession
|
|
|
How do cemental caries look radiographically?
|
ill-defined
saucer-shaped "scooped-out" discolored |
|
|
(acute/chronic) caries are often seen in childhood and ages 15-25
|
acute
|
|
|
People that frequently snack or have poor hygiene often have (acute/chronic) caries
|
acute
|
|
|
What spreads faster, acute or chronic caries?
|
acute
|
|
|
(acute/chronic) caries are initially small with rapid penetration and spread at DEJ
|
acute
|
|
|
What type of caries are described by poor diet, and extensive caries
|
rampant caries
|
|
|
sudden and uncontrollable destruction is a sign of ___ caries
|
rampant
|
|
|
Who gets rampant caries the most?
|
young kids/teens
adults w/Xerostomia |
|
|
(acute/chronic) have a large surface entrance at initial stages
|
chronic
|
|
|
(acute/chronic) caries are more common in adults
|
chronic
|
|
|
The slow progress of (acute/chronic) caries allows time for sclerosis of tubules and 2ndary dentin
|
chronic
|
|
|
True or False, pain is very common in chronic caries
|
False
|
|
|
(primary/secondary) caries are defined as a new lesion with no prior cavity preparation
|
primary
|
|
|
What is another name for recurrent caries
|
secondary caries (hmmm go figure...)
|
|
|
What type of caries (primary/secondary) develop at margins of existing restorations?
|
secondary
|
|
|
If someone gets secondary caries, what might this indicate
|
1. susceptible to caries
2. bad hygiene 3. poor restoration |
|
|
Why are secondary caries often hard to see?
|
The existing restoration can "hide" them
|
|
|
Caries are usually (more/less) severe than they look on a radiograph
|
more
|
|
|
(over/under) exposure can mask proximal caries
|
over
|
|
|
What type of non-carious phenomenon is mistaken for cervical caries?
|
cervical burnout
|
|
|
Bad (vertical/horizontal) angulation results in foreshortening or elongation
|
vertical
|
|
|
Bad (vertical/horizontal) angulation results in overlap of contacts
|
horizontal
|
|
|
List a few types of restorations that appear RL and may mimic caries
|
1. older silicates
2. older Ca(OH)2 3. resins 4. some composites |
|
|
True or False, hypoplastic teeth (or enamel hypoplasia) can mimic caries
|
True
|
|
|
True or False, abrasion and attrition are the same thing
|
false, abrasion is mechanical wear, attrition is physiologic wear
|
|
|
If you brush too hard, you can get (abrasion/attrition) of the tooth structure
|
abrasion
|
|

What type of caries are indicated by the red arrow? purple arrow?
|
Red - R3 (mesial)
Purple - R2 (distal) |
|

What opaque region is indicated by the green arrow?
|
Reparative dentin
|
|

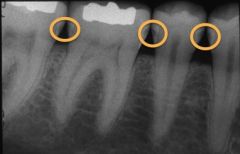
What level are all three carious lesions?
|
R1
|
|
These caries can all be classified as interproximal and what level?
|
R2
|
|

The orange and blue box are what level of caries? (not the same)
|
orange - R4
blue - R3 |
|

These caries are at what level?
|
R4
|
|

What is the likely cause of this little area of radiolucency?
|
cervical burnout
|
|

What is indicated by the white arrows?
|
Cervical burnout
|
|
|
What is wrong with the root of this tooth?
|
cemental caries
|
|

What is wrong with the root of this tooth?
|
Cemental caries
|
|

A patient comes in and you take this radiograph. It is an adult with xerostomia and the claim they didn't have cavities like this a year ago. What is your diagnosis?
|
rampant caries
|
|

A patient comes in and you take this radiograph. You notice that the caries indicated by the black arrow have looked nearly identical on radiographs for this patient for a few years now. What is your diagnosis? (bonus: what does the orange arrow indicate?)
|
Chronic caries, reparative dentin
|
|

What kind of caries are indicated by the green arrows?
|
Recurrent (aka secondary) caries. Notice that they are UNDER an existing restoration!
|
|

What is indicated by the red arrow? purple arrow?
|
red - recurrent caries
purple - R1 (incipient) interproximal carious lesion |
|

One of these is attrition and one is abrasion. Which is which?
|
green - attrition
blue - abrasion |
|

What is indicated by the blue arrow?
|
Gutta percha (root canal material)
|