Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
In periodontal disease, which direction does the junctional epithelium migrate?
|
apically
|
|
|
(long/short) scale gives you more detail
|
long
|
|
|
Does high or low kVp give you better visualization of bony detail and tooth roots?
|
high
|
|
|
You get straighter photons with a (short/long) BID
|
long
|
|
|
(Bitewings/PAs) more accurately record the distance between CEJ and crestal bone
|
bitewings
|
|
|
If the PDL and lamina dura cannot be seen, we are likely (over/under) angulated on the maxilla
|
over
|
|
|
The distance between the CEJ to the crest of the bone should be between __ and __ mm
|
1.5-2
|
|
|
What % of bone loss is usually needed before it is detectable?
|
30-50%
|
|
|
What type of radiograph analysis can detect bone loss after only about 5%?
|
digital subtraction (although, it is rarely used)
|
|
|
Conventional radiographs provide a (2/3) dimensional view
|
2
|
|
|
True or False, radiographs are very good at detecting the extent of mobility
|
False
|
|
|
What are some limitations to radiographs when it comes to perio disease?
|
Can't see soft tissue to hard tissue relationship
can't see facial or lingual aspect of teeth Can't see extent of mobility can't see early furcations doesn't reveal the difference between successful and unsuccessfully treated cases |
|
|
Radiographs show (more/less) bone destruction than there actually is
|
less
|
|
|
Increased width of PDL, resorption of lamina dura, and bone loss (& decrease in bone density) are all signs of what?
|
perio disease
|
|
|
Radiographs will reveal a (increased/decreased) width of PDL, (deposition/resorption) of the lamina dura, and bone (formation/loss) in periodontal disease
|
increased, resorption, loss
|
|
|
True or False, restoration overhangs do not trap plaque because plaque cannot adhere to metal effectively
|
False! They do trap plaque
|
|
|
(heavy/open) contacts can lead to food impaction
|
open
|
|
|
What are the 5 main functions of tooth contacts and embrasures?
|
allow food to escape occlusally
prevent food impaction protect the periodontium distribute force stabilize arch |
|
|
True or False, calculus is never mineralized enough to be visible on radiographs
|
false, with lots of mineralization, it will be visible!
|
|
|
Indistinctness and interruption of __ along the mesial and distal aspect of the interdental alveolar crest is a sign of problems
|
lamina dura
|
|
|
In the (anterior/posterior) region, damage to the alveolar crest will appear as blunting
|
anterior
|
|
|
In the (anterior/posterior) region, damage to the alveolar crest will appear as loss of sharp angle between LD and alveolar crest, loss of normal cortical surface, and irregular or diffused border
|
posterior
|
|
|
Widening of the PDL by bone resorption along mesial or distal aspect of interdental crestal bone is called
|
Triangulation (or funneling)
|
|
|
funneling is also called _____
|
triangulation
|
|
|
The sides of the 'triangle' in triangulation are formed by the __ & ___ and the base it towards the (crown/root)
|
alveolar bone, root surface, crown (apex towards root)
|
|
|
Finger-like radiolucencies extending from the crestal bone into the interdental bone are known as ___ bone changes
|
interseptal
|
|
|
nutrient canals become (more/less) prominent in interseptal bone changes
|
more
|
|
|
Reactive sclerosis is a defense mechanism where what occurs?
|
Deposition of more bone to fight against infection progress
|
|
|
Normal bone level is located approximately __-__mm apical to the CEJ of tooth
|
1-1.5
|
|
|
Which is more generalized, horizontal or vertical bone loss?
|
horizontal
|
|
|
(horizontal/vertical) bone loss occurs on plane parallel with a line connecting CEJ's of adjacent teeth
|
horizontal
|
|
|
(horizontal/vertical) bone loss occurs on plane not parallel to line connecting CEJ's of adjacent teeth
|
vertical
|
|
|
(vertical/horizontal) bone loss is typically due to local irritants and not many other factors
|
horizontal
|
|
|
(vertical/horizontal) bone loss is typically due to a variety of factors
|
vertical
|
|
|
Infrabony pockets may be classified as:
one-wall, two-wall, three-wall, or four-wall. What are the general descriptions of these names? |
One-wall: hemiseptal
Two-wall: crater-like Three-wall: three walls with root forming the 4th wall-more common on mandibular molar region Four walled: circumferential, surrounds the tooth |
|
|
A (1/2/3/4) wall defect is identical to vertical deformities
|
1
|
|
|
The normal CROWN to ROOT ratio is __:__
|
1:2
|
|
|
A (wider/narrower) PDL indicates potential tooth mobility
|
wider
|
|
|
Where are furcations MOST common?
LEAST common? |
Most common - man molars
least common - max premolars |
|
|
Furcations can only be seen radiographically at what point?
|
when the bone extends apically beyond the furca
|
|
|
Radiograph symptoms of chronic periodontitis may occur __-__ months after initial disease onset
|
6-8
|
|
|
True or False, if there is a very sharp angle between the LD and alveolar crest in the posterior region, this is a sign of chronic periodontitis
|
False, the LOSS of a sharp angle
|
|
|
(mild/moderate/severe) horizontal bone loss is 1-2 mm of loss
|
mild
|
|
|
(mild/moderate/severe) horizontal bone loss is up to the midpoint of root or furcation area
|
moderate
|
|
|
(mild/moderate/severe) horizontal bone loss is anything beyond the furcation area
|
severe
|
|
|
(horizontal/vertical) bone loss is typically localized
|
vertical
|
|
|
What is a good indirect method to detect infrabony defects?
|
use gutta percha
|
|
|
What is the etiology of aggressive periodontitis?
|
unknown!
|
|
|
The rate of bone loss in agressive periodontitis is __-__ times faster than expected
|
3-4
|
|
|
Diastima and distolabial migration of what teeth are indications of aggressive periodontitis?
|
max incisors
|
|
|
What is the best way to detect periodontitis radiographically?
|
Take images over time and compare them
|
|
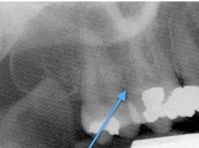
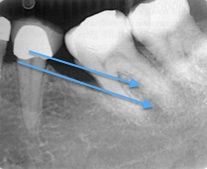
True or False, the bone indicated by the blue arrow is in error
|
True (bone is not actually taking up proximal area. Wrong angulation!)
|
|

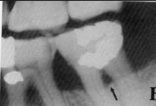
The radiograph indicated a problem with the teeth indicated in the orange circle. What is it?
|
open contacts
|
|

What small RO tabs are indicated by the black arrows?
|
calculus
|
|
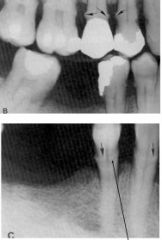
What is indicated by ALL the black arrows on both films?
|
calculus
|
|

What RO tabs are indicated by the two black arrows?
|
restoration overhang
|
|

What is the name for the process indicated by the black arrows?
|
funneling (or triangulation)
|
|
Whats the name for the process that makes this area slightly more RO than expected?
|
reactive sclerosis (new bone deposited to fight infection)
|
|
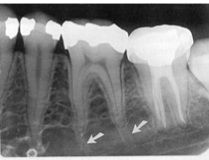
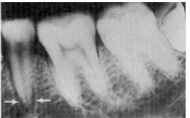
What are indicated by the white arrows?
|
nutrient canals
|
|
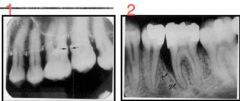
Which is horizontal bone loss? vertical?
|
horizontal - 1
vertical - 2 |
|
|
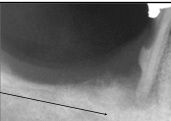
Is this horizontal or vertical bone loss?
|
horizontal
|
|

Is this horizontal or vertical bone loss?
|
horizontal
|
|

This is a (#) wall defect
|
1
|
|

This is a (#) wall defect
|
2
|
|
The tooth on the far left is (more/less) mobile than a normal tooth
|
More mobile (wider PDL)
|
|
What is the name for the RL area indicated by the black arrow?
|
furcation
|
|

Horizontal or vertical bone loss?
|
vertical bone loss
|