![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
56 Cards in this Set
- Front
- Back
|
Nutrients required for RBC production |
Fe, Co, Mn. B12, B6, C, E, folate, riboflavin, pantothenic acid, thiamine. Amino Acids |
|
|
Erythropoiesis regulated mainly by |
Erythropoietin Thryroid hormone Androgens |
|
|
Hemoglobin molecule |
Synthesized at the polychromatic normoblast stage of red cell development. Hemoglobin = Heme + Globin. Hemoglobin = 4 Heme structures with Fe in the center and 2 pairs of Globin chains. |
|
|
Reticulocyte |
Cell just one stage prior to the mature erythrocyte. |
|
|
Normal Reticulocyte count |
0.5 - 1.5% |
|
|
Stains for reticulocyte count |
Methylene Blue Brilliant Cresyl Blue |
|
|
Increased Retic Count |
Hemolytic Anemia Response to treatment of Iron / B12 / Folic acid. Recent Hemorrhage. Thalassemia. Pregnancy. Erythroblastosis fetalis. HbC disease. Leukemias. Hypoxia. |
|
|
Decreased Retic Count |
Decreased adrenocortical and anterior pituitary activity. Aplastic anemia. Cirrhosis. Megaloblastic anemia. Exposure to radiation. Anemia of chronic diseases. MDS |
|
|
Oversimplification of Retic count |
If cause of anemia is inside marrow - decreased Retic count. If cause of anemia is outside marrow - increased Retic count. |
|
|
Reticulocyte index |
= Reticulocyte count x Patient's HCT/Normal HCT |
|
|
Reticulocyte Proliferation Index |
= Corrected Reticulocyte Count/Shift Correction Factor PCV 45% = 1 PCV 35% = 1.5 PCV 25% = 2 PCV 15% = 2.5 |
|
|
Hematocrit (HCT) aka... |
Packed Cell Volume (PCV) Erythrocyte volume fraction (EVF) |
|
|
Formula for HCT |
Red cell number x Red cell volume |
|
|
High HCT/PCV |
Dehydration. Kidney disease with high EPo. Low O2 level in blood. Congenital heart disease. Cor Pumonale. Pulmonary fibrosis. High altitude. Polycythemia vera Smoking |
|
|
Low HCT/PCV |
Blood loss. Bone marrow failure. EPo deficiency. Hemolysis. Leukemia. Malnutrition. Multiple myeloma. Autoimmune/Collagen vascular disease like SLE or RA |
|
|
Note about PCV value: |
An elevated PCV may be due to spleen hyperfunction and a low PCV may indicate low thymus function. |
|
|
Rule of Three.... |
Hb x 3 = HCT +/- 3 RBC x 3 = Hb Exception to this rule is in patients with hypochromic red cells. These patients will have hematocrits that are more than 3 times the hemoglobin. |
|
|
MCV, MCH, MCHC were first introduced by.... |
Wintrobe |
|
|
MCV |
MCV = (HCT/Red Cell Count) x 100 |
|
|
MCV<72fl with normal RDW
|
Usually Thalassemia |
|
|
Anemia with normal MCV - Normocytic Anemia |
Acute Hemorrhage. Dimorphic Anemia. Hemoglobinopathies. Anemia due to inadequate blood cell production. Endocrinopathies (hypopituitarism, hypothyroidism, hypoadrenalism, hypogonadism) Anemia of chronic diseases. |
|
|
Anemia with increased MCV - Macrocytic anemia |
Megaloblastic Anemia. Pernicious Anemia. Sprue. Macrocytic anemia of pregnancy. Di Guglielmo disease. Myelodysplastic syndromes. Myelophthisic Anemia Post - splenectomy. Alcoholism. Liver disease. Anemia of hypothyroidism. Drugs. |
|
|
Anemia with decreased MCV - Microcytic Anemia |
Hypochromic Iron deficiency Thalassemia Lead poisoning Disorders of Porphyrin synthesis Normochromic Anemia of chronic disease (< 1/3rd of the patients) Heterozygous thalassemia and hemoglobinopathies |
|
|
Interferences with MCV |
Cold agglutinins (increased values) Warm autoantibodies. Marked hyperglycemia (increased MCV) Marked leukocytosis (increased values) In vitro hemolysis or fragmentation of RBCs (decreased values) Methanol poisoning (increased values) Marked reticulocytosis (>50% from any cause) (increases MCV) |
|
|
MCH |
MCH = (Hb/red cell count) x 100 |
|
|
Increased MCH |
Macrocytic Anemia Newborns and Infants |
|
|
Decreased MCH |
Microcytic and Normocytic Anemias |
|
|
Interferences in MCH |
Lipemia Marked Leucocytosis (>50,000/microL) Cold agglutinins In Vivo hemolysis Monoclonal proteins in blood High heparin concentration |
|
|
MCHC |
= Hb/HCT x 10 |
|
|
MCHC decreased in |
Microcytic hypochromic anemia (Normal value does not rule it out) |
|
|
MCHC increased in |
Hereditary spherocytosis Infants and Newborns Autoagglutination Artifactual |
|
|
Interferences to MCHC |
Decrease Marked Leucocytosis Increase Hemolysis Cold agglutinins Severe Lipemia of serums Rouleaux / RBC agglutinates High Heparin conc. |
|
|
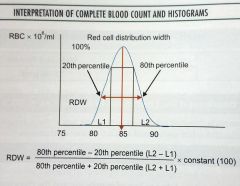
RDW |
|
|
|
RDW - what is it? |
Quantitative measurement or numerical expression of anisopoikilocytosis. |
|
|
RDW-CV |
= (SD of RBC Volume/mean MCV) x 100 Reference values: 11.5-14.5% |
|
|
RDW-SD |
Actual measurement of the width of erythrocyte distribution curve. This measurement is performed at the relative height of 20% above the baseline. The wider the curve is spread by RBCs of different sizes, the higher the RDW-SD value will be. Reference values: 35-45 fL. |
|
|
RDW - Exclusion of two extreme ends of RBC histogram |
Excluding extreme left side : Platelets, platelet clumps, and electrical interference. Excluding extreme right side : Clumped RBCs, overly large RBCs. |
|
|
Anemia - Normal MCV, Normal RDW |
Anemia of chronic disease Acute blood loss Acute hemolysis CLL CML Hemoglobinopathy |
|
|
Anemia - Normal MCV, Increased RDW |
Early IDA Early Vit.B12 Early Folate Sickle Cell Anemia |
|
|
Anemia - Low MCV, Normal RDW |
Anemia of chronic disease Thalassemia (heterozygous) |
|
|
Anemia - Low MCV, Increased RDW |
IDA RBC Fragmentation HbH Thalassemia intermedia G6PD deficiency |
|
|
Anemia - High MCV, Normal RDW |
Aplastic Anemia Preleukemia Myelodysplsatic Syndrome |
|
|
Anemia - High MCV, Increased RDW |
Vit B12 deficiency Folate deficiency Immune hemolytic anemia Liver disease Cold agglutinins Alcoholism |
|
|
Gross summary of above combinations |
Nutritional disorders - Independent of MCV have increased RDW Hemolytic disorders - Independent of MCV have increased RDW that is directly proportional to the degree of anemia caused by the disorder. Hypoproliferative disorders - Independent of MCV have normal RDW |
|
|
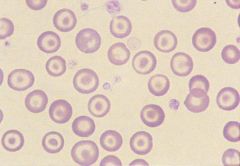
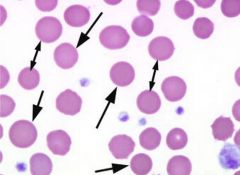
Microcytic, hypochromic RBCs |
RBCs are smaller than the nucleus of the small lymphocyte. Have markedly increased pallor, more than 1/3rd of diameter of RBC. Causes: IDA Thalassemia Minor Sideroblastic Anemia Lead Poisoning Pyridoxine defiency |
|
|
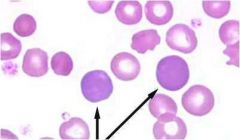
Macrocytic RBCs |
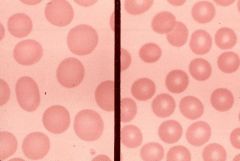
Most of the RBCs are larger than the nucleus of small lymphocyte. (Size >8.5 microns) Causes: Vit B12 or folate deficiency. Alcoholism Liver Disease MDS Hypothyroidism Drugs impairing DNA synthesis |
|
|
Oval Macrocyte |
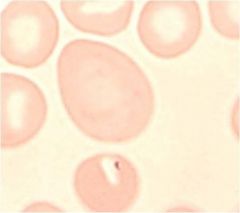
Causes: Folate deficiency Vit B12 deficiency Pernicious anemia MDS Post Chemotherapy |
|
|
Hypochromic macrocyte |
Causes: Alcholism Hypothyroidism Liver Disease Post Splenectomy |
|
|
Blue Tinged Macrocytes |
Causes: Neonates Response to Anemic Stress |
|
|
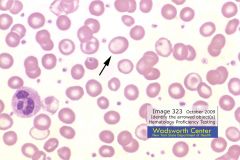
Target cells aka Bell cells aka Mexican hat cells aka Cododcytes |
Characteristic ringed appearance - due to increased surface area to volume ratio - excess membrane pools in the middle of the cells. Causes: Thalassemia Hemoglobinopathies (HbAC/CC/SS/SC) Liver disease Post splenectomy Severe IDA HbE Abetalipoproteinemia |
|
|
Note about Target cells |
In patients with obstructive liver disease, lecithin cholesterol acetyltransferase activity is depressed, which increases the cholesterol-to-phospholipid ratio and produces an absolute increase in the surface area of the red cell membrane. In contrast, membrane excess is only relative in patients with iron-deficiency anemia and thalassemia because of the reduced quantity of intracellular hemoglobin. |
|
|
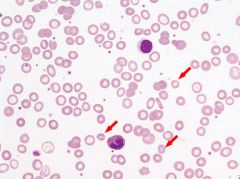
Schistocytes aka Schizocytes |

Physical damage to RBCs within bloodstream create these cells - include helmet cells, triangles, crescents and microspherocytes. |
|
|
Causes of Schistocytes |
Causes: DIC Severe hemolytic anemia Microangiopathic hemolytic anemia Hemolytic Uremic Syndrome Prosthetic/Abnormal Cardiac Valve Coarctation of Aorta Connective tissue disorders Burns (spheroschistocytes as a result of heat) TTP Uremia, ATN, Glomerulonephritis Malignant HTN Systemic amyloidosis Liver Cirrhosis Disseminated Carcinomatosis Chronic Relapsing Schistocytic hemolytic anemia |
|
|
Tear drop cells aka Dacrocytes |
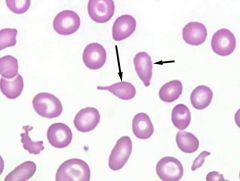
Pear shaped cells usually microcytic, hypochromic. Causes: Newborn Thalassemia major Leukoerythroblastic reaction Myeloproliferative syndrome |
|
|
Spherocytes |
Ball shaped RBCs, decreased surface/volume ratio, hyperdense (>MCHC). Causes: Hereditary spherocytosis ABO incompatibility Autoimmune hemolytic anemia, Microangiopathic hemolytic anemia, SS disease, Hypersplenism, Burns, Post Transfusion, Pyruvate Kinase deficiency, Water-dilution hemolysis |
|
|
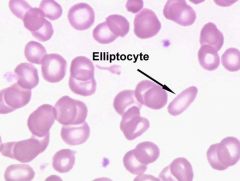
Elliptocyte |
Normally seen in less than 1% of RBC Causes: Hereditary Elliptocytosis IDA Thalassemia Major Leukoerythroblastic reaction Malaria Megaloblastic Anemia Any anemia may present with 5-10% elliptocytes |