Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
Significance of Na transport
|
•Na and water transport within the kidney are responsible for the maintenance of ECF and BP
|
|
|
Function of the Kidneys
|
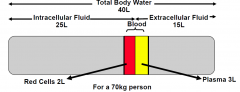
Regulate the volume and composition of body fluids within narrow limits
–Total body water ie 58% of body mass –Intracellular (5/8ths) and extracellular (3/8ths) body fluids |
|
|
Functions of the kidney in ion composition
|
–Maintains electrolyte composition, Na, K, HCO3, Cl, Ca, PO4, and hence acid base status
–Regulates volume through regulation of Na reabsorption and secretion. –Regulates ‘concentrations’ through regulation of water transport. –Volume regulation (ie maintenance of BP) overrides regulation of electrolyte concentrations and acid base status. |
|
|
Hypovolaemia causes
|
–GIT Na losses
–Sweating –Renal Na losses – eg diuretics, mineralocorticoid deficiency, renal tubular disease |
|
|
Hypervolaemia causes
|
–Iatrogenic – Na loading
–Renal Na retention in generalised oedema states (CCF, cirrhosis, nephrotic syndrome –Renal Na retention in renal failure –Primary mineralocorticoid excess |
|
|
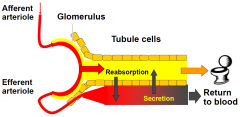
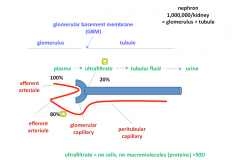
•Glomerular filtration
|
–is the process whereby a clear fluid is produced from the blood perfusing the glomerulus at each nephron. Blood, proteins and other macromolecules are excluded from the ultrafiltrate
–Produced largely because of hydrostatic pressure ie blood pressure (Hence if blood pressure falls below a critical perfusion pressure glomerular filtration stops! |
|
|
•Tubular Modification
|
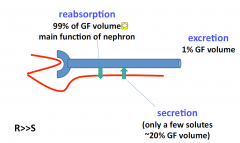
–Tubules alter the volume and composition of the glomerular ultrafiltrate
–Overall 99% of the filtrate is reabsorbed. However some organic molecules/drugs are secreted into the ultrafiltrate |
|
|
Filtration and Reabsorption in the Kidney
|
|
|
|
Blood flow and GFR
|
•Kidneys receive 20% of the cardiac output
•CO about 5L/minute. Hence renal blood flow about 1000ml/min •Assuming a Hct of 50%, then renal plasma flow is 500ml/min •If filtration fraction is 20% then GFR is 100ml/min or 144L/24 hrs. •Given 99% filtrate is reabsorbed 1L urine per 24 hrs |
|
|
Main task of the kidneys is to
|
Main task of the kidney is to regulate body fluid composition and volume
•Volume regulation (I.e. ECF volume) is dependent on regulation of Na transport •Osmolality (in effect serum Na) is dependent on regulation of water transport •These two factors are independent |
|
|
Regulation of renal Na transport
•Dependent on |
–Delivery of Na to the kidney
»thus affected by BP, cardiac output, renal blood flow –Renal function »Including glomerular filtration rate (GFR), and intact tubular mechanisms for Na reabsorption –Hormonal influences on tubular Na reabsorption »Dominant influence is via the renin-angiotensin system on Na transport in the distal tubule |
|
|
RAAS acts mainly at the
|
distal tubule
DOMINANT INFLUENCE IS HERE (idk if its the only input.. other slides saying it acts at the proximal tubules too) •Whilst the proximal tubule is responsible for the bulk of Na transport, the distal tubule/CCD is the target of most regulation. |
|
|
Dysregulation of renal Na transport
|
•Glomerular dysfunction
–Reduced delivery of Na to the tubule, thus if severe results in Na retention •Tubular dysfunction (due to primary renal disorders or secondary hormonal or haemodynamic influences on the tubule) –May -> excess Na losses and volume depletion –May -> excess Na reabsorption and increased ECFV, normally manifesting as hypertension Normally 180 litres (each containing 140 mmol/l Na) are filtered by the glomerulus each day. Hence a 1% change in reabsorption results in large changes in Na and fluid homeostasis |
|
|
Proportion of Na reabsorption throughout the kidney tubules
|
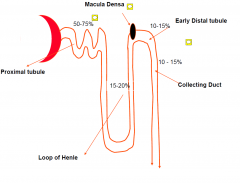
MAIN: proximal tubules
HOWEVER: (drugs) Na regulation is late distal tubule and collecting duct (seems counter intuitive but it is soo that the Na regulation is unaffected by tublues down track because thee is nothing down track) |
|
|
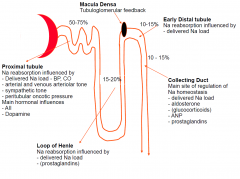
Macula Densa
|
lies in close proximity to the glomerulus and feeds back to by producing renin (juxtaglomerulua apparutus)
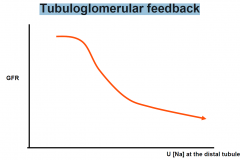
•Macula densa located at this site which regulates tubuloglomerular feedback –Ie - if increased Na delivery is sensed by the macula densa at the early distal tubule, a signal is transmitted to the glomerulus which reduces GFR. –Signal most likely involves adenosine |
|
|
Regulation of renal Na transport Proximal tubule
|
•Responsible for ‘bulk’ transport (50-75%)
•Glomerulotubular balance applies –I.e if increased filtration, then increased reabsorption –GT balance perturbed mainly by physical factors. Eg - high BP, increased ECF volume or low plasma oncotic pressure -> decreased proximal Na reabsorption •Hormonal influences on PT Na reabsorption –Angiotensin II -> increases PT Na reabsorption –Dopamine inhibits Na reabsorption •Increased sympathetic tone increases PT Na reabsorption –Low BP or low ECF volume -> activates renal sympathetic nerves and Na reabsorption stimulated |
|
|
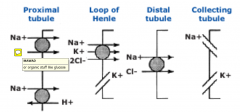
Proximal tubule Pumps
|
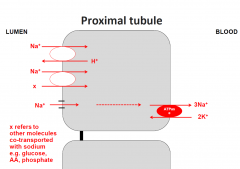
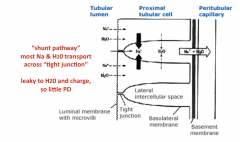
MOST Na and water via the shunt pathway; isotonic
|
|
|
Regulation of renal Na transport Loop of Henle
|
•Responds to delivered load of Na
•Prostaglandins -> inhibit Na reabsorption in the loop |
|
|
LOH Pumps
|

Shunt is WATER IMPERMEABLE
|
|
|
Regulation of renal Na transport Distal convoluted tubule
|
•Responds to delivered load of Na
•Macula densa located at this site which regulates tubuloglomerular feedback –Ie - if increased Na delivery is sensed by the macula densa at the early distal tubule, a signal is transmitted to the glomerulus which reduces GFR. –Signal most likely involves adenosine |
|
|
Tubuloglomerular feedback
|
|
|
|
Early Distal Tubule Pumps
|
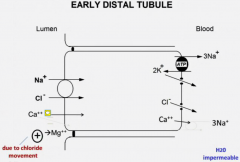
- also water impermeable
- hypercalcaimic - main reason due to proximal reabsorption (due to dec. Na levels.. ) - INC ca reabsorption - Ca |
|
|
Regulation of renal Na transport Collecting Duct
|
•Main site of regulation of Na transport
•Main regulators are: –Delivered Na load –Activation of the renin angiotensin system -> Increased action of aldosterone –Atrial natriuretic hormone. »Released from the atria under conditions of volume expansion and inhibits Na reabsorption in the distal tubule –Other glucocorticoids –Prostaglandins |
|
|
Main Regulators of Na
|
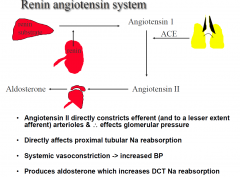
–Activation of the renin angiotensin system -> Increased action of aldosterone
–Atrial natriuretic hormone. »Released from the atria under conditions of volume expansion and inhibits Na reabsorption in the distal tubule –Other glucocorticoids –Prostaglandins |
|
|
RAAS
|
|
|
|
Aldosterone in distal tubule
|
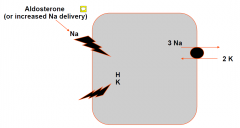
Net effect of Aldosterone is to increase Na entry into cell -> facilitates Na reabsorption -> K losses (hypokalaemia -> H losses (alkalosis) -> increase ECFV, BUT over the course of a few days Na excretion becomes normal, but at the expense of increased ECF and BP
|
|
|
Cortical Collecting Duct Pumps
|
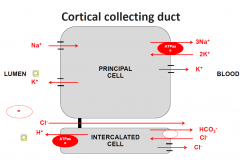
Order of events:
1. Na reabsorbed 2. -ve lumen drives K+ out PRINCIPAL CELL 1. Na/K/ATPase 2. Na channel (lumen to cell) 3. -ve INC. in lumen, drives K out of the cell AND drives Cl- away INTERCALATED CELL reabsorbs -ve ions and secretes H+ - H+ loss is increased with aldosterone usage too (countering the -ve lumen) |
|
|
Summary Slide of Renal Tubule
|
|
|
|
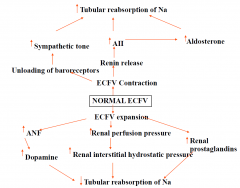
Mechanisms to deal with volume change
|
|
|
|
Endocrine Function of the Kidneys
|
EPO
activation of VitD (1OH to 25OH vit D) renin |
|
|
Priority of Functions within the Kidney
|
volume> osmolality > potassium & acid‐base
|
|
|
Kidney Overview
|
|
|
|
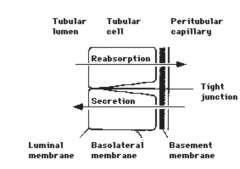
Tubular Cells
|
|
|
|
Reabsorption, Secretion and excretion
|
|
|
|
"Shunt" pathway
|
|
|
|
Renal Sodium Transporters
|
|
|
|
Reabsoption of Proteins
|

in proximal tubule
- specific receptors (eg megalin, cubilin, AMN) |
|
|
Proximal tubular disorders
|
low MW proteinuria
renal glycosuria aminoaciduria phosphaturia uricosuria hypokalaemia proximal RTA |
|
|
Loop of Henle (thick ascending limb)
transport lesions |
salt wasting and hypovolaemia
hypokalaemia high renin and aldosterone JGA hypertrophy metabolic alkalosis hypomagnesaemia (+/-) hypocalcaemia (Hypercalciuria) impaired urine concentration BP normal or low |
|
|
Juxtaglomerular Cells
|
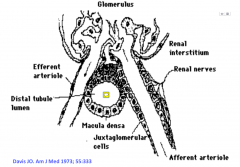
this apparatus produces renin
|
|
|
Early distal tubule transport lesions
|
mild salt wasting and hypovolaemia
hypokalaemia metabolic alkalosis hypomagnesaemia hypocalciuria (hypercalcaemia)* impaired urine dilution* BP normal or low * differences between it and the LOH |
|
|
Cortical collecHng duct transport
lesions |
A. IMPAIRED Na TRANSPORT ‐
salt wastng hypovolaemia hypotension hyperkalaemia metabolic acidosis (RTA type IV) B. ENHANCED Na TRANSPORT ‐ salt retenHon hypertension hypokalaemia (K wasHng) metabolic alkalosis low renin and aldosterone C. IMPAIRED H+ SECRETIONRenal tubular acidosis |
|
|
RTA Type 1
|
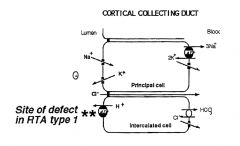
renal tubular acidosis
- abnormality in H+ excretion |
|
|
RTA 4
|
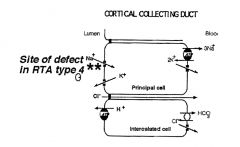
defect in principal cell
- thus the lumen is no longer -ve and thus harder to secrete H+ ions into the lumen and alos harder to secret K+ |