Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
88 Cards in this Set
- Front
- Back
|
Functions of the skin
|
Immunologic barrier
Temperature regulation Protection from radiation Nerve sensation Injury repair Appearance |
|
|
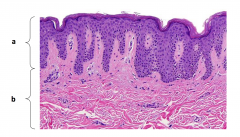
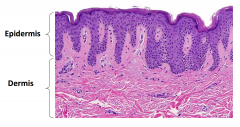
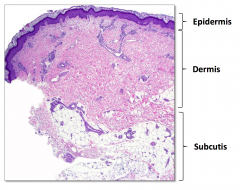
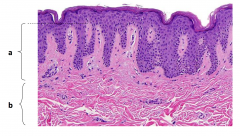
Layers of skin
|
Epidermis
Dermis Subcutis |
|
What are the layers of skin
|
Epidermis and Dermis
|
|
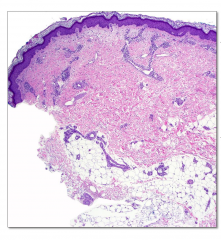
Layers of the skin
|
|
|

4 major layers of epidermis
|
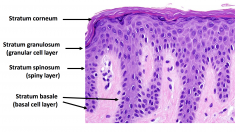
Stratum Corneum
Stratum granulosum (granualar cell layer) Stratum Spinosum (spiny layer) Stratum basale (basal cell layer) |
|
|
Three main types of cells that make up the epidermis
|
Keratinocytes
Melanocytes Langerhans Cells |
|
Two layer of dermis
|
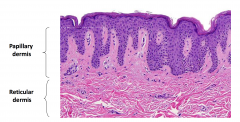
Papillary dermis
Reticular dermis |
|
|
Structures in the dermis
|
blood vessels
lymphatic vessels nerves pilosebaceous units apocrine glands eccrine glands |
|
|
Cells of the dermis
|
Fibroblasts
-- synthesize collagen Mast cells -- immune response; release histamine |
|
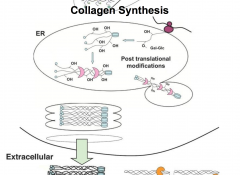
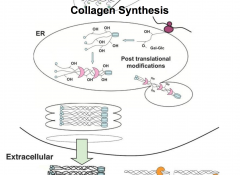
Collagen synthesis
|
|
|
|
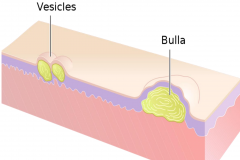
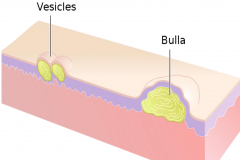
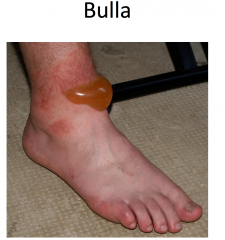
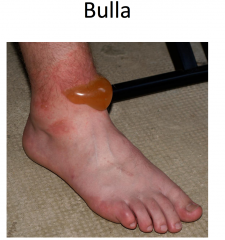
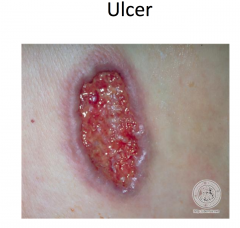
Vessicles and bulla both contain clear fluid.
Vessicle < 1cm Bulla > 1 cm |
|

|

|
|
|
|
|
|
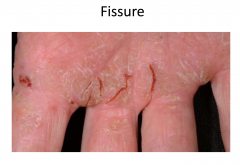
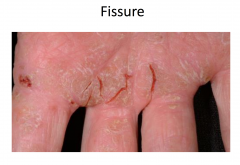
Secondary lacerations
|
|
|
|
|
|
|
|
|
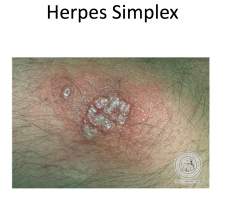
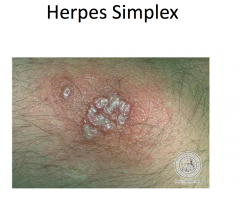
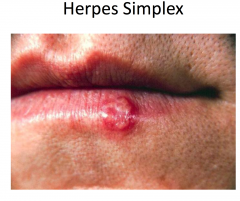
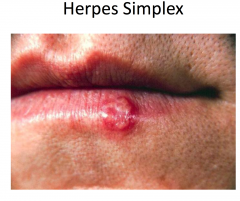
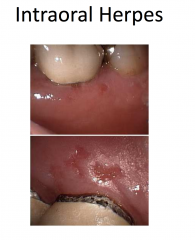
Herpes Simplex
|
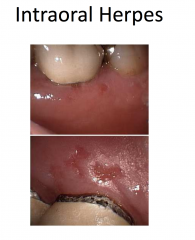
Herpes simplex viruses 1 and 2
Painful, grouped vesicles on an erythematous base -- may appear pustular (white to yellow) -- may see just erosions Pain and recurrence suggests HSV |
|
|
|
|
|
|
|
|
|
|
|
HSV Pathogenesis: Course of infection
|
Primary infections (once in a lifetime!)
Virus transmission to mucosa or abraded epithelium Robust lytic replication that is limited to inoculation site |
|
|
Which cell types support HSV replication
|
Many
|
|
|
Which cell types support HSV latency
|
Neurons
|
|
|
In what situations will HSV disseminate systemically
|
In cases such as severely immunocompromised host. May disseminate systematically and seed to several organs (adrenal glands, liver, CNS)
|
|
|
What does herpes simplex virus infect?
|
Sensory neurons innervating the site of inoculation - retrograde transport to the sensory ganglia where the virus establishes latency
|
|
|
Sites of herpes simplex latency : HSV-1
|
Trigeminal ganglia
|
|
|
Sites of herpes simplex latency : HSV-2
|
Sacral ganglia
|
|
|
Stimuli that trigger herpes simplex
|
Stress
Physical trauma these trigger viral reactivation leading to a switch from latent to lytic life cycle |
|
|
Reinfection of an individual with HSV
|
Reinfection of a seropositive indiv with a different strain of HSV is possible, but uncommon - exogenous reinfection
|
|
|
Diagnosis of Herpes SImplex
|
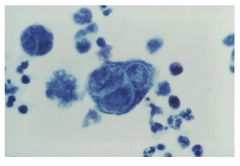
- Tzanck Smear (low sensitivity and specificity)
- Molecular test (direct fluorescent antigen, polymerase chain reaction ) - rapid <24 hours & high sensitivity and specificity |
|
|
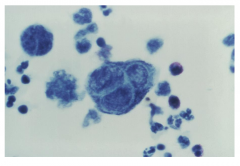
Positive Tzanck Smear
Merged with other cells. They are fusigenic. Becomes a large gigantic multinucleated cell. |
|
|
HSV Treatment
|
No treatment needed for most infections
-- treatment started within first 24 hours can shorten duration or decrease severity |
|
|
Treatment that is needed for certain infections:
|
Severe gingivostomatitis
Extensive cutaneous disease Ocular involvement Pregnant patient Immunocompromised patient |
|
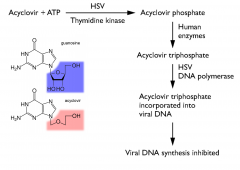
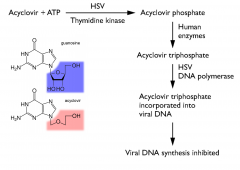
Acyclovir Mechanism
|
|
|
|
Acyclovir
|
Valacyclovir is the prodrug of acyclovir
Ganciclovir, valganciclovir, and famciclovir have similar MOA |
|
|
Adverse effects of acyclovir
|
Oral
-- nausea, vomiting, diarrhea -- headache IV -- phlebitis at injection site -- Nephrotoxicity (crystal formation) |
|
|
Herpes Zoster
|
- Caused by an eruption of latent varicella zoster virus (VZV)
- Clues to the diagnosis - Dermatomal (zosteriform) eruption on one side of the body - Grouped vesicles on an erythematous base - Most often on trunk but can be anywhere - Usually preceded by pain or burning - Generally shingles occurs only once in the immunocompetent , in contrast to herpes simplex virus which frequently recurs. |
|
|
Which herpes virus is resistant to acyclovir and requires high dose
|
CMV (lack thymidine kinase)
|
|
|
Varicella Zoster pathogenesis
|
VZV is an alpha herpes virus and belongs to the same subfamily as HSV
|
|
|
Primary Infection of Varicella Zoster
|
VZV replicated in the upper respiratory tract, is efficiently aerosolized during coughing and is readily acquired via respiratory route
VZV spreads systematically and replicates throughout the body Secondary viremia seeds VZV to the skin, where it causes widespread vesicular rash -- chicken pox |
|
|
Latency of HSV virus
|
Viral latency is supported by many ganglia as opposed to one of a few for HSV
Virus can reactivate from ANY infected ganglia later in life to cause shingles Unlike HSV several viral gene products are actively transcribed and translated within latently infected neurons -- how the virus deals with the immune system recognition in vivo is unclear |
|
|
VZ Vaccine
|
Live, attenuated virus-oka strain
given to young children Main mechanism is to decrease the symptoms of primary infection and therefore decrease the efficiency of virus spread 15-20% of vaccinated individuals do get eventually infected with wild type VZV that foes on to establish latency. Symptoms of primary infection are not present and a vaccinated individual does not know that they picked up wt VZV. |
|
|
Wild type VZV in a vaccinated individual
|
Wild type VZV can reactivate and cause zoster later in life, in spite of immunization
Oka vaccine strain establishes a lifelong latent infection, reactivation can occur, but is very inefficient in immocompetent indiv; reactivation of vaccine strain , at worst, results in mild symptoms |
|
|
Oka Vaccine strain can be transmitted to?
|
Immunocompromised individuals - use caution when vaccinating healthy children with immunocompromised siblings
|
|
|
Usefulness of Oka Vaccine
|
Elderly patients to prevent zoster. Recent studies show that immunization can limit zoster.
Immunity in aged not as long lasting, booster is recommended in pop > 60 |
|
|
Chicken Pox
|
VZV primary infection
Diffusely scattered vesicles on an erythematous base - vesicles arise in crops and are in different stages - "Dewdrops on a rose petal" Can be extensive and severe, especially in adult |
|
|
Impetigo
|
Bacterial infection caused by gram pos bacteria
-- S. aureus -- S. pyogenes --- aka group A beta-hemolytic strep Majority of lesions are crusted papules (impetigo contagiosa) |
|
|
S. aureus
|
Gram pos cocci
Encodes many toxins that are responsible for virulence |
|
|
Where does S. aureus colonize?
|
Anterior nares of healthy individuals
|
|
|
How does S. Aureus spread?
|
Via person to person or person-fomite contact
Can survive on artificial surfaces for a long time Methicillin-resistant strains are of particular concern |
|
|
Staphylococcal Scalded Skin Syndrome
|
Focus of infection secretes toxin into the blood
- Epidermolytic toxin A - Epidermolytic toxin B Widespread superficial blisters - skin peels away in sheets - Wound cultures from erosions are negative |
|
|
Who is at risk for Staphylococcal Scalded Skin Sydrome
|
Kids < 2 years and adults with renal disease
Consult dermatology immediately |
|
|
|
|
|
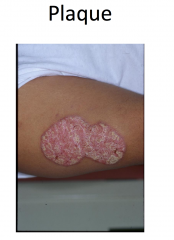
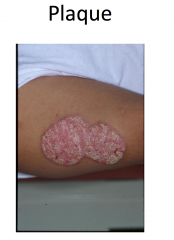
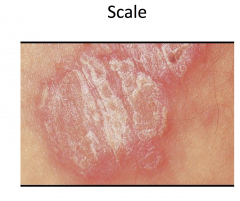
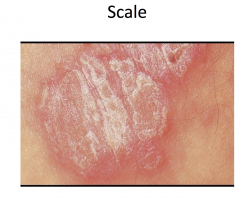
Psoriasis
|
Chronic plaque psoriasis most common variant
Sharply defined plaques with silvery-white scale, often symmetric -- most common on elbows, knees, scalp, presacrum, hands, and feet -- genitalia involved in up to 30% Arthritis in 20-30% of patients Increased risk of metabolic syndrome and CVD Several other variants; more than one may coexist simultanceously |
|
|
Immunology of psoriasis
|
Considered a prototypic type 1 helper T cell disease
-- increased IL-2, IL-12, IFN-gamma, TNF-alpha - decreased IL-1, IL-10 Th17 and Th22 cells more recently found to be crucial in pathogenesis |
|
|
Treatment of Psoraisis
|
Individualized balancing extent and severity of disease
Topical treatments: topical corticosteroids, topical vit D analogs, tar based therapies, topical retinoid Phototherapy (PUVA, NBUVB, excimer laser) Systemic Therapy - methotrexate - cyclosporine - retinoids - biologic agents |
|
|
Methotrexate
|
Synthetic analog of folic acid
Competitively inhibits DHFR -- necessary for pyrimidine and purine synthesis Adverse Effects -- nausea, anorexia, fatigue, alopecia, stomatitis -- leukopenia, thrombocytopenia -- hepatotoxicity Also effective in treating psoriatic arthritis |
|
|
Leucovorin
|
Active metabolite of folic acid
Displaces methotrexate from intracellular binding sites and restores the folate required for DNA/RNA synthesis Used for inadvertent methotrexate overdose or high dose methotrexate rescue |
|
|

|
|
|
|
|
|
|
|
|
|
|

|

|
|
|
Exanthematous Drug Eruption
|
Morbilliform drug eruptions
MC type of drug-induced eruption Mechanism likely immunologic; often thought to be delayed (type IV) hypersensitivity reaction Occurs 7-14 days after drug started Low grade fever may be present Spontaneously resolve in 1-2 weeks MC caused by aminopenicillins, sulfonamides, cephalosporins, anticonvulsants |
|
|
Signs of a possible severe cutaneous reaction
|
Mucous membrane involvement
Temperature above 38.5 C Blisters Facial edema and erythema Lymphadenopathy Painful skin lesions Marked peripheral blood eosinophilia |
|
|
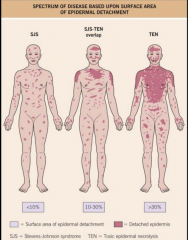
Stevens Johnson Syndrome/ Toxic Epidermal Necrolysis
|
Onset between 1-3 weeks of drug initiation
Typical lesions are tender dusky red or purpuric macules that progress to flacid bullae and erosions Often fever, LAD, hepatitis, cytopenias |
|
|
Where is Stevens Johnson Syndrome/ Toxic Epidermal Necrolysis found
|
Buccal, ocular, and genital mucosae in > 90%
Respiratory tract involved in 25% |
|
|
What typically causes Stevens Johnson Syndrome/ Toxic Epidermal Necrolysis?
|
Allopurinol, anticonvulsants, antibiotics, NSAIDs
|
|

|
|
|

|

Top layer of epidermis slides away from underlying skin
|
|
|
|
|
|
Hypersensitivity reaction and EBV
|
Occurs in up to 90% of patients with EBV induced infections mononucleosis treated with amoxicillin or ampicillin
-- less often PCN or cephalosporins Occurs 7-10 days after starting med |
|
|
|
|
|
|
|
|
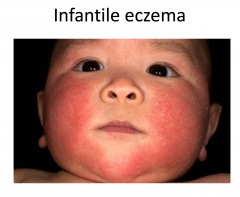
Atopic Dermatitis
|
Chronic disease with periods of worsening and remission
|
|
|
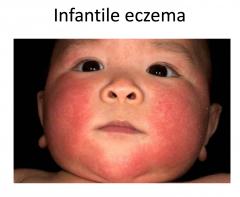
Atopic Dermatitis : Infantile Stage
|
More acute; involves face, scalp, extensor surfaces of the extremities, diaper area spared, secondary impetiginization common
|
|
|
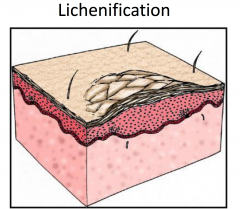
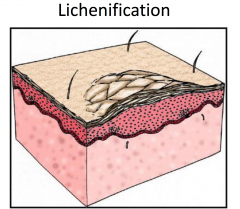
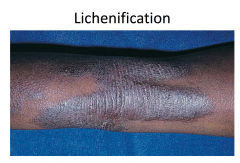
Atopic Dermatitis: Childhood Stage
|
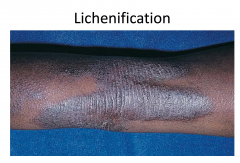
More chronic; involved flexural folds and extremities, more lichenification
|
|
|
Atopic Dermatitis: Adult Stage
|
Variable course; hand dermatitis common
|
|
|
|
|
|
|
|

|

|
|

|

|
|
|
Immunology of Eczema
|
Considered a prototypic type 2 helper T cell disease:
-- Increased IL-4, IL-5, IL-13 -- Decreased IL-2, IFN-gamma Defects in epidermal skin barrier -- decreased essential fatty acids -- fillagrin mutations -- increased susceptibility to allergens -- increased water loss Defects in cell mediated immunity -- increased susceptibility to viral, bacterial, and fungal infections of the skin |
|
|
Molluscum Contagiosum
|
Most common in children; increased risk with atopic dermatitis
Appears 7 weeks after exposure to the virus Firm, small, pink, or flesh colored dome-shaped papules Spread by contact with infected skin or clothing Most people have complete clearing in 2-4 months Lesions persist and are more numerous in those with weakened immune systems |
|
|
Structure of Molluscum Contagiosum
|
Very large DSDNA virus - poxvirus family
Virion is ovoid to brick shaped, complex structure Replictes exclusively in the cytoplasm of infected cell -- a unique feature for a DNA virus Single life cycle -- lytic replication |
|
|
Histology of Molluscum Contagiosum
|
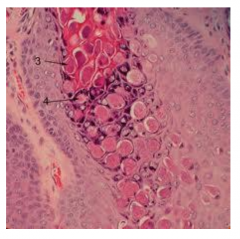
Includes molluscum bodies - large eosinophilic inclusions in the cytoplasm -- viral factories
|
|

|

central depression - umbilication
|
|
|
Eczema Herpeticum
|
AKA Kaposi varicelliform eruption
Refers to viral infection of a pre-existing dermatosis Sudden eruption of painful, edematous, crusted vesicles, pustules, and erosions May be associated with high temperature, malaise, LAD Most commonly caused by disseminated HSV infection in patients with atopic dermatitis and referred to as eczema herpeticum requires IV acyclovir |