Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
|
Sepsis epidemiology:
|
*600-750,000 pt/yr
*100-200,000 deaths/yr *17 Billion USD/yr |
|
|
Increase in sepsis rates in past few decades:
|
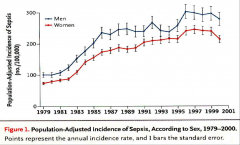
*21 yr study: 10 million severe sepsis pt-750 million hospital discharges-NHDS in USA.
*More likely to develop in males. |
|
|
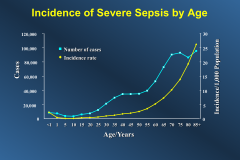
Incidence of Severe Sepsis by Age:
|
|
|
|
The changing microbiology of severe sepsis:
GPB, GNB, Fungi: |
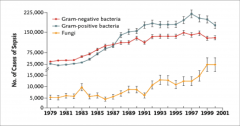
*fungi mainly candida
|
|
|
∆ in sepsis mortality rates in past 45 years:
|
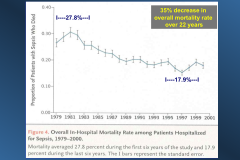
*due to better care in ICU.
|
|
|
Definition of sepsis/continuum:
|
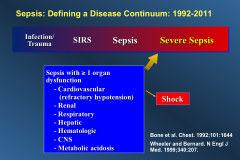
*SIRS=just sick
*severe sepsis= inflammatory response has become badly damaging to yourself *Septic shock = hypotension, severe |
|
|
Proposed Definitions of--
Infection: Sepsis: Septic Shock: |
*Infection: interaction with a microorganism that induces a local or systemic host response (old term-sepsis); if microbe induces no host response=colonization
*Sepsis: A deleterious host response to infection resulting in organ dysfunction remote from the site of infection (old term was "severe sepsis") *Septic Shock: sepsis complicated by diffuse microvascular dysfunction causing hypotension not responsive to simple fluid challenge (usually accompanied by tissue hyoperfusion and multi-organ dysfunction) |
|
|
The pathobiology of fever:
|
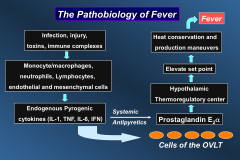
OVLT= organum vasculosum of the lamina terminalis
|
|
|
Effect of fever on sepsis prognosis:
|
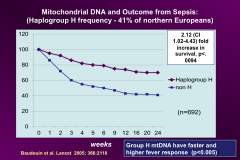
*higher fever response means better survival from sepsis
*Determined by mitoDNA *Northern Europeans are protected; somehow |
|
|
The Adaptive Value and the Perils of the Febrile Response:
|
*Favorable Attributes
-Bactericidal to some pathogens -Heat Shock Proteins, APR -Iron stress for pathogens -Increases cardiac output -Increases PMN chemotaxis, phagocytosis, and B cell antibody responses *Detrimental Effects -Increases caloric needs -Increased myocardial work -Somatic tissue catabolism, cell turnover -Febrile seizures, denatures proteins -Increased fluid losses |
|
|
Should you treat fever?
|
*In general-it's better not to treat fever in an infected patient; fever is a biomarker for successful intervention.
|
|
|
Is there value to fever if you're not infected?
What about hypothermia? |
*No
*No- you should be more concerned about a hypothermic patient. |
|
|
Pathophys of septic shock:
|
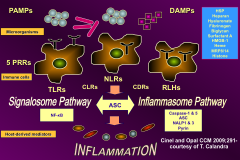
*Infection and Damage from inflammation look the same.
|
|
|
What's the initiating cause of sepsis?
What the outcome determinant? |
*The pathogen is the initiating cause of sepsis
*But the host response determines outcome |
|
|
Different kinds of TLRs and what they recognize:
|

*Lots of locations
*Lots of things they bind *TLR2 --> gram negs *TLR1 --> gram pos *NOD1 and NOD2 |
|
|
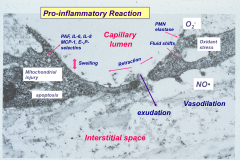
Describe damage in the microcirculation due to inflammation:
|
|
|
|
Why is it bad to stay in prolonged septic shock?
|
*“The longer you’re in shock the less likely you will get out of shock”
*Adrenergic receptor down regulation following prolonged and repeated stimulation *Massive release of nitric oxide via iNOS and eNOS synthesis -vascular smooth muscle relaxation -Oxidant stress, peroxynitrite production-apoptosis -Insensitivity to C’AMP-mediated vasoconstriction *Myocardial depression -“MDF” (TNF, IL-1, IL-6, NO): ß3 receptor availability *Vasopressin deficiency-V1 receptors up regulated *Microvascular dysfunction, microthrombi |
|
|
Diagnosis of Sepsis:
|
*No single lab test, clinical finding or hemodynamic event is diagnostic for sepsis
*Clinical Diagnosis of an invasive infection (with or without bloodstream invasion) + a deleterious host response - fever (or hypothermia), leukocytosis (or neutropenia), tissue hypoperfusion with or without systemic hypotension *multiorgan involvement- DIC, AKI, ARDS, CNS dysfunction, Lactic acidosis, hepatic dysfunction *Shock- fluid non-responsive hypotension (BP<90/60) with early hyperdynamic cardiovascular response (high CO, normal Lt Atrial filling pressure, Low systemic vascular resistance) |
|
|
Treatment of Severe Sepsis:
|
*Standard therapy
-Early recognition and intervention -Early fluid resuscitation, followed by restricted fluids -Bactericidal antibiotics -Treat the focal infection -Supportive care *Newer treatments of sepsis -Intensive insulin therapy -Stress dose steroids for relative adrenal insufficiency -Hemofiltration and plasmaphoresis -Low tidal volume ventilation -Immunomodulators, maybe |
|
|
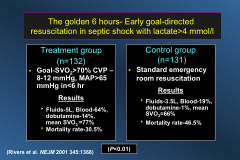
Describe the Golden 6 hours in sepsis treatment:
|
|
|
|
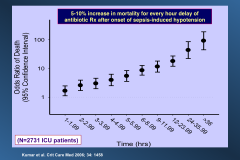
Importance of early antibiotics in sepsis:
|
|
|
|
What should fluid treatment be like in the second 24 hrs of sepsis treatment?
|
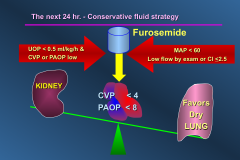
*keep them on the dry side after first 24 hrs
|
|
|
Effects of glucose control in sepsis treatment:
|
-Studies have gone both ways.
-High blood sugar probably okay unless it's extremely high. |
|
|
VENTILATION WITH LOWER TIDAL VOLUMES COMPARED WITH TRADITIONAL TIDAL VOLUMES FOR ACUTE LUNG INJURY AND ARDS:
|
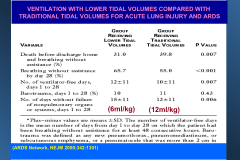
*Use low stretch ventilation*
|
|
|
Effects of activated PRO C?
|
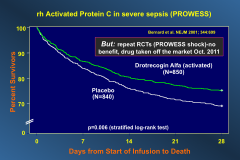
*None. Don't use it.
|
|
|
Effect of Treatment With Low Doses of Hydrocortisone and Fludrocortisone on Mortality in Patients With Septic Shock:
|
-unclear.
-effects of steroids are inconclusive. |
|
|
Prognostic factors in septic patients:
|
*Before onset of sepsis
-Severity of underlying disease -Age -Gender (males do worse) -Genetic polymorphisms -Status of Immune defenses *After onset of sepsis -APACHE II -Need for ventilator -Multiorgan failure -Polymicrobial bacteremia -Pseudomonas, candida, enterococcal bacteremia -Early antibiotics, ? euglycemia, optimal fluids, low TV ventilation, ? Stress-dose steroids? albumin? |
|
|
Current overall mortality from sepsis:
|
Current overall mortality 25-35% severe sepsis-40-45% for septic shock managed in the ICU.
|