![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
308 Cards in this Set
- Front
- Back
|
How do you classify foot type? |
Navicular tubercle position to the Feiss Line |
|
|
What is the feiss line? |
Line from the plantar surface of the head of the 1st MT to apex of medial malleolus |
|
|
When should foot type be measured? |
During weight bearing (Standing)
[Because arch changes when weight bearing] |
|
|
Where is the navicular tubercle during a pes planus foot? |
The navicular tubercle located below feiss line |
|
|
The pes planus foot is a _________ medial longitudinal arch, _______ forefoot and ______ rearfoot |
*Low or bulging *Abducted *Everted |
|
|
The pes planus foot is similar to pronation or supination? |
Pronation |
|
|
What does congenital pes planus foot mean? |
Hereditary |
|
|
What is acquired pes planus foot? |
Suffered an injury |
|
|
How does one have acquired pes planus foot? |
*Rupture or weakness of planatr fascia, plantar ligaments, spring ligaments, tibialis posterior or anterior
Fatigue or damage to static stabilizers of arch leads to PPF |
|
|
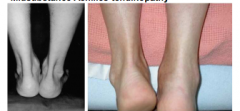
What is the too many toes sign? |
Since forefoot is abducted in the pes planus foot, so when stand behind someone who is not wearing shoes in their neutral stance you can see 3-5 toes because the forefoot is abducted |
|
|
What does an everted rearfoot look like? |
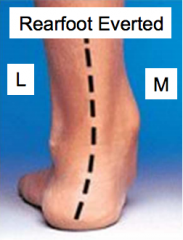
(See too much for the forefoot) |
|
|
For people with acquired pes planus they might need support and assistance with what? |
Straight leg heel raise |
|
|
What is an indicator of pronation? |
Navicular drop |
|
|
What is navicular drop |

The distance the navicular tuberosity moves in standing as the subtalar joint is allowed to move from its neutral to relaxed position
Get the person to stand. Then palpate the talus and adjust foot till feel equal medial and lateral heads and say that is the neutral position. Then have the subject relax and see if the foot collapses then meausre where the navicular was and see how much of a difference that drop was |
|
|
What does rigid pes planus foot mean? |
That the pes planus there for both weight bearing and non-weight bearing |
|
|
What does flexible pes planus mean? |
That pes planus only there during weight bearing |
|
|
Can you correct a rigid pes planus foot? |
No, but can cushion |
|
|
Do you have increased or decrease shock absorbing capacity with a rigid pes planus foot |
Decreased
(When we make contact with the ground we want to go from supination into pronation but if it is arleady in pes planus we don't have the ability to absorb forces through the pronation of gait so forces will be increased up the kinetic chain) |
|
|
How do you correct for flexible pes planus foot? |
Orthotics correction |
|
|
What are the possible assoications of pes planus foot? |
*MT Stress fracture *Navicular stress fracture *Knee pain *Low back pain *Plantar fasciitis |
|
|
How do you define PPF with an X-ray? |
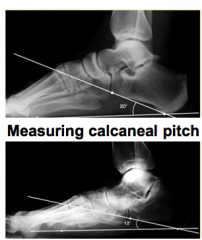
Looking at calcaneal pitch
"Pitch" = inclination off the calcaneous |
|
|
Where is the navicular tuberosity located on a pes cavus foot? |
Navicular tuberosity is located above the Feiss Line |
|
|
Are there more or less people with pes cavus foot? |
Less |
|
|
Pes cavus foot has a _____ medial longitudinal arch, _____ forefoot and _____ rearfoot |
*High *Adducted *Inverted |
|
|
The pes cavus is more like pronation or supination |
Supination |
|
|
Since the pes cavus foot has a higher arch what does that do the stiffness of the foot? |
Stiff |
|
|
If there is a stiffer foot what does that do to the shock absorbing capacity? |
Decreased |
|
|
What are the possible association for the pes cavus foot? |
*Claw or hammer toe *Metatarsalgia *Plantar fasciitis *Hypomobile first ray *Stress fracture of the MTs, tibia and femur |
|
|
Why can pes cavus foot lead to plantar fasciitis |
The foot is rigid and so won't go through pronation as much, plantar fascia gets loaded a lot more |
|
|
Does the pes cavus foot have a higher or lower calcaneal pitch? |
Higher |
|
|
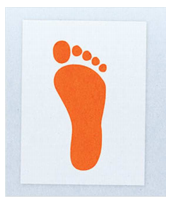
What does the wet foot test look like for the pes planus foot? |
|
|
|
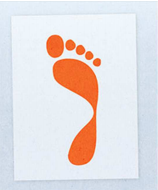
What does the wet foot test look like for a normal foot? |

|
|
|
What does the wet foot test look like for the pes cavus foot? |
|
|
|
What is hammer toe and claw toe |
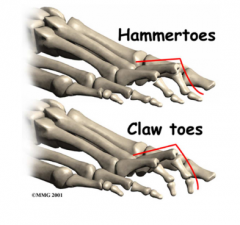
Hammer toe is differnet than claw toe because the distal interphalangeal joint is extended as opposed to flexed |
|
|
What is the Morton's Foot (Mortion's Toe)? |
Shorted 1st MT so it looks like the 2nd toe is really short |
|
|
What is the consequence of Morton's Foot? |
Increased weight bearing through the 2nd toe and MT which is not designed to do that so it is more suseptible to stress fractures |
|
|
How much of the population has Morton's Foot/Toe? |
10% |
|
|
What does the plantar fascia do? |
Plantar fascia reinforces longitudinal arches of the foot |
|
|
what is the plantar fascia important for? |
Force absorption Propulsion |
|
|
Aggravation of the PF can result in _______ |
Irritatin and inflamation |
|
|
However many chronic cases of plantar fasciitis does not involve _____, but rather ______ |
*Active inflammation *Degeneration of the PF |
|
|
What is the mechanism of injury for plantar fasciitis? |
Repeat stress (overuse) or single traumatic episode |
|
|
What is baxter's nerve |
Possible entrapment of branch of lateral plantar nerve in the porta pedis |
|
|
How do you differnetiate between plantar fasciitis |
If load foot and don't do anything to the knee of hip and it is painful then it is probably plantar fascia
If load foot and nervous system by extending the knee and flexing the hip and feel pain then there is a nerve problem |
|
|
What is the signs and symptoms of plantar fasciitis? |
*Pain localaized at origin of PF (palpation on medial calcaneal tubercle is painful)
*Pain/stiffness upon waking in the morning (because when sleep in supine, feet is plantar flexion for around 8 hrs)
*Heel pain during/after activity
*pain with passive ankle doriflexion
*Pain in DF with passive toe extension (Windlass Effect) |
|
|
What is the prognosis for plantar fasciitis? |
*Conservative treatment is effective for 80% of cases but takes a long time to heal and sometimes greater than a year to feel satisfactory outcome
*Sgns and symptoms can persist for months to years
|
|
|
Do bilateral or unilateral cases of plantar fasciitis respond less favorably |
Bilateral
Because probably has to do with the anatomy of the foot |
|
|
Does rupture (chronic plantar fasciitis) risk increase after corticiosteroid injection? |
es
Chronic plantar fasciitis doesn ot always result in rupture and there are people who can rupture the plantar fascia and never exterience ain beforehand |
|
|
Can plantar fascia rupture occure without prior history |
Yes
(For example males greater than 20-25 yrs old who pariticpate in running and jumping type sports) |
|
|
What are the early conservative treatments for people with plantar fasciitis? |
*Stretching of foot/gastroc-soleus complex
*Soft tissue release
*Longitudinal arch taping
*Ice cup massage with foot on stretch (post exercise) |
|
|
What is the prolonged conservative treatment of plantar fasciitis? |
*Prefabricated insoles, heel cups, orthotics (chornic cases)
*Night splint (Locked in 90 degres)
*Corticosteroid injection |
|
|
What is the agressive, chronic treatment for plantar fasciitis? |
*Electoporeal shockwave therapy (after 6 months of conservative treatment) [Powerful ultrasound, uncomfortable hammering on tissue)
*Surgical release (Come in and remve any scar tissue that is impinging on the nerve itself or creating extra pressure in the area) |
|
|
What is a heel spur? |
Exotosis, bony outgrowth of the medial calcaneal tubercle |
|
|
What is an exostosis |
Excessive bone growht that is typically seen on sites with insertion of structures at the origin of short toe flexor |
|
|
What shape is the heel spur? |
Hook shaped |
|
|
Can the heel spur occur simultaneously with plantar fasciitis? |
Yes, but not necessarily causal of each other
Sympotms are similar |
|
|
What is the signs and symptoms of heel spur? |
Gradual onset of symptoms
Pain during heel strike phase of gait |
|
|
What is the treatment of heel spur? |
*Still treat conservatively if at all possible
*Stretching
*Comfortable and supportive footwear
*Heel cups
*Surgery (spur removal or endoscopic plantar fasciotomy |
|
|
What is the mechanism of injury for the metatarsal fracture? |
Can occur with direct or overuse trama |
|
|
What are the types of fractures for the fifth metatarsal? |
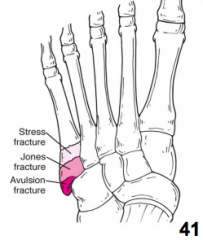
*Jones Fracture (Base of the 5th MT)
*Stress Fracture (Distal to jones)
*Avulsion Fracture (Peroneal brevis avulses off styloid process) |
|
|
What is the metarsal fracture for the 2nd, 3rd or 4th MT? |
march fracture |
|
|
Is it rare to see a stress fracturei n the 1st MT? why |
Yes, because it is such a thick and strong bone |
|
|
What is the MT shaft fracture's mechanism of injury? |
Something dropped on the foot or the foot has twisting on it |
|
|
What is the 5th MT suseptible to fractures? |
Because the blood supply varies throughout the bone itself
When fractures are through the base of the 5th MT, the blood supply also affected so healing is much mroe complicated |
|
|
What is the signs and symptoms of MT stress fractures? |
Localized bone pain (dull pain that can be present at rest but increases with activity
Can progress to a gross fracture if not treated
Need to get patient to rest right away |
|
|
What is the signs and symptoms of acute MT fractures |
*Intense pain (may be unable to Weight bear)
*Crepitus (Assess for this during palpation --> Crunching sensation)
*Acute onset of swelling over fx site |
|
|
What is the treatment of avuslsion fractures |
Immobilization and non-weight bearing for four weeks |
|
|
What is the treatment for jones fracture? |
Immobilization and non weightbearing
Surgery (internal fixation with a screw)
Recovery for 8+ weeks |
|
|
What is the treatment of a stress fracture? |
*Rest
*PWB with fixed cam walker boot
*Bone growth stimulator
*Avoid aggressive return and resulting gross fracture |
|
|
Where is the lsfranc joint |
Tarso-metatarsal joint |
|
|
What are the type of injuries from a lisfranc injury? |
*Sprain *Dislocation *fracture-dislocation |
|
|
What is the MOI for a lisfranc injury> |
High energy axial loading of foot while distal segment is fixed and that causes a buckling of the join
(IE being stepped on back of the heel with ball of foot planted) |
|
|
Signs and symptoms for lisfranc injuries? |
*Range to from subtle to obvious (pain, swelling, deformity, ecchymosis on plantar surface) of midfoot
*Acute mid-foot injury with pain should have flip to r/o Lisfranc injury
-Lisfranc fracture: 2% of all fracture, but often misdiagnosed |
|
|
What is the conservative treatment of lisfranc injuries? |
Non-weight bearing |
|
|
What is the surgical treatment of lisfranc injuries? |
*Open reduction and internal fixation
*8 weeks NWB (cast/splint)
*Arthrodesis for ligamentous injury (surgical joint fusion) --> Worst case scenario |
|
|
What is an intermetatarsal neuroma? |
Enlargement of that erve |
|
|
What is morton's neuroma |
Typically entrapment of the 3rd common digital (plantar) nerve, located between 3rd and 4th MTs |
|
|
What is the MOI of Morton's Neuroma |
*Prolonged pressure of nerve resulting in formation of fibrotic nodules and edma around the nerve
|
|
|
What the contributors to the prolonged pressure MOI for Morton's Neuroma? |
*Excessive pronation
*Improperly fitted shoes |
|
|
Are women or men more likely to get morton's neuroma? |
Women |
|
|
Is there a high re occurence rate of morton's neuroma? |
Yes |
|
|
What is the signs and symptoms of morton's neuroma? |
*Pain in transver (metatarsal) arch of foot, radiating to toes
*Numbeness/paresthesia into the toes
*Increased pain/numbness when pressure is increased in forefoot (standing on toes) or with tight shoes
*Positive: increase in symptoms with metatrsal compression (Squeezing foot) |
|
|
What positive test is for Morton's Neuroma |
Mulder sign |
|
|
What can you occassionally palpate on the plantar surface of the metatarsal arch for Morton's Neuroma |
Nodule |
|
|
What is the treatment for Morton's Neuroma |
*Metatarsal arch pad
*Low dye taping (Widens MT arch)
*Lidocaine/Corticosteroid injection
*footwear modification
*Surgical excision (remove scar tissue around nerve) |
|
|
What is hallux rigidus? |
Stiff great toe |
|
|
What does hallux rigidus involve |
Progressive degeneration of first MTP joint's articular surfaces |
|
|
Is hallux rigidus often a bilateral or unilateral ocndition? |
Bilateral, genetic disposition |
|
|
What may hallux rigidus progress to |
Ankylosed joint (Fused) |
|
|
What are the signs and symptoms of hallux rigidus |
*Stiff 1st ray
*Impacts toe off
*Pain and swelling after/during activity
*Exotosis devlopment possible on dorsal aspect of MTP joint |
|
|
What are the associations with hallux rigidus |
Morton's toe
(People with morton's toe are more suseptible to getting this condition) |
|
|
What is the treatment of hallux rigidus |
*Passive ROM and joint mobilization
*Orthodics to unload the first MTP joint (decrease hyperextension)
*Turf Toe taping (Limiting DF)
*Corticosteroid injection (Quiet down inflammation)
*Surgical intervention (Cheilectomy: Removal of distal portion of MT and exotosis) |
|
|
What is hallux valgus? |
Progressive degeneration and subluxation of the first MTP joint
charactized by the MTP because in over 20 degrees of abduction
"valgus deformity"
Associated with a bunion (exotosis) on medial aspect of the joint |
|
|
What is the treatment for the hallux valgus? |
Taping to increase adduction and limit abduction
Appropriate shoes
Pad between 1st, 2nd, 3rd phalanges
NSAIDS
Surgical intervention: Changing the shape of the foot (reshape of the 1st of MT)
Exosectomy (bunionectomy)
and
Osteotomy (chevron osteotomy at the distal end of MT) |
|
|
What is turf toe? |
Sprain at the 1st MTP joint |
|
|
what is the mechanism of injury for turf toe |
Foot planted, is made to go to dorsiflexion and first toe is hyperextended
Can also involved force walgus or varus of the 1st MTP joint |
|
|
What is the signs and symptoms of turf toe? |
*Pain with toe off during gait or quick stops
*Pain with palpation
*Limited ROM of MTP joint |
|
|
What is the treatment for Turf toe |
*Rest and NWB-PWB in acute stages (cam walker)
*RICE
*Turf toe tapingstrap (stabilize toe)
*Firm shoe inserts or fabricated orthoplast insertW |
|
|
What are the sesamoids? |
Two bones in the tendons of the flexor hallucis brevis tendons that act with the same mechanical advantage as the patellar tendon
They are less stable in the MT groove in extension therefore they have the most forces placed on them during extension |
|
|
What is the MOI for sesamoiditis? |
Overuse injury (in conjunction to poor shoe type) more stress during extension when it's not as stable in the MT groove
May result in stress fracture of seasmoids |
|
|
What is the signs and symptoms for sesamoidits? |
*Pain when "being on toes (IE toe off, high heeled shoes)
*Walk on outside of foot to avoid pressure
*TTP over ball of foot (Under 1st MT head)
*Painful passive extension ROM of 1st MTP joint |
|
|
What is the treatment of sesamoiditis? |
*Padding or orthotics designed to unload the ball of the foot and dissipate forces on sesamoid bone
*Corticosteroid injection
*Surgical excision of sesamoid bones (if chronic pain) |
|
|
What type of joint is the talocrural joint? |
Hinge joint |
|
|
What is the the angle joint movememnt of the talocrural joint? |
Dorsiflexion Plantarflexion |
|
|
Is the talus dome wider anteriorly or posteriorly? |
Anteriorly |
|
|
Is the axis of rotation of the talocrural joint oblique or completely horizontal? |
Oblique (tilteD) |
|
|
What is the close packed position of the talocrural joint? |
Full dorsiflexion
Talus locked against the fibula and tibula
(Ie mid stance of gait and squatting) |
|
|
What is the subtalar joint? |
Talocalcaneal joint |
|
|
What movement does the talocalcaneal joint have? |
Inversion and eversion (1 degree of freedom) |
|
|
What are static stabilizers? |
Components of the lateral and medial ligment complexes of the talocrural joint |
|
|
Is inversion and eversion detrimental to the talocrural joint? |
Yes, because of its geometry |
|
|
Are the distal projections of the lateral and medial malleoli different? |
Yes |
|
|
Is inversion or eversion of the subtalar joint greater? |
Inversion
They increase potential stress on the talocrural joint static stabilizers |
|
|
Are lateral or medial ankle sprain more common? |
Lateral (80%) |
|
|
What are the MOIs for lateral ankle sprains? |
*Excessive supination (injure talocrural and subtalar joint)
*Pure inversion (Rolling over the lateral surface of the foot, stepping on an uneven surface (IE first base) with the ankle dorsiflexed)
*Contact with another player |
|
|
What are the three lateral ankle ligaments |
*Anterior talofibular ligament
*Calaneofibular ligament
*Posterior talofibular ligament |
|
|
Which is most often injured during the lateral ankle sprain? |
Anterior talofibular ligament
(Taut in supination) |
|
|
When is the clacaneofibular ligament injured during the lateral ankle sprain? |
Injured with more significant inversion |
|
|
Which is the most rarely injured ligament in lateral nakle sprains? |
Posterior talofibular ligament |
|
|
How do you injure the posterior talofibular ligament in a lateral ankle sprain? |
Inversion and dorsiflexed ankle |
|
|
What is the signs and symptoms of the lateral ankle sprain? |
*Popping
*TTP sinus tarsi and lateral ligament complex
*Diffuse ecchymosis and edmea/swelling (increases with the severity of injury)
*Pain or laxity with anterior drawer test or talar tilt test |
|
|
What do you have to rule out first for a lateral ankle sprian? |
Fracture (fibula, tibia, talus)
Avulsion fracture (styloid process of the 5th MT) |
|
|
What is the predispositon for the lateral ankle sprain? |
Previous history of ankle instability or sprain |
|
|
What are the two types of chronic ankle instability? |
Mechanical instability
Functional instability |
|
|
What is mechanical instability? |
Gross laxity of the talocrural or subtalar joints with clinical examination |
|
|
What is functional instability? |
History of repeated ankle sprains but normal findings during ligamentous stress tests
Reports instablity but none of that shown in tests, could be from neuromuscular control |
|
|
What are osteophytes? |
Bone spurs |
|
|
What are osteochondral defects? |
When ankle subluxes and goes back in, articular cartilage is damaged |
|
|
What is osteoarthritis? |
People who develop have an increased chance for a significant ankle trauma |
|
|
What are the secondary complications of ankle sprians? |
Osteophytes
Osteochondral defects
Osteoarthritis |
|
|
Baed on the ottawa ankle rules when do you get ankle films |
If there is malleolar pain and any of
1) Tender on posterior edge, tip or distal 6 cm of lateral or medial malleolus
2) Unable to complete 4 steps |
|
|
Based on the Ottawa Ankle Rules when do you get foot films |
Midfoot pain and any of:
1) Navicular tenderness (Navicular bone has poor outcome for healing so you don't want to miss it)
2) Base of 5th of MT tenderness
3) Cannot complete 4 steps |
|
|
What is a syndesmosis sprain? |
High ankle sprain |
|
|
What does the syndesmosis sprain come form |
Injury to the tibofibular syndesmosis (syndesmosis that is holding two bones together) and inferior anterior tibiofibular ligament |
|
|
What will syndesmosis sprain reuslt in? |
Lateral displaement of the distal fibula, shifting off the ankle |
|
|
Waht is the occurance rate of the syndesmosis sprain? |
10%
18% in NFL |
|
|
Is the prognosis for the syndesmosis sprain slower to return or quicker to return? |
Slower to return because it is the injury of a structure that holding two bones together that has been injured and when step down, thebones seperate and is very painful. Longer timing to heal mechanical outcome of injury is the problem |
|
|
What is the MOI of a syndesmosis sprain |
External rotation of talus when ankle is dorsflexed |
|
|
What is the signs and symptoms of the syndesmosis sprain? |
*Pain (TTP) localized anterior aspect of the ankle (inferior tibio fibular joint)
*Pain wiht ankle dorsiflexion
*Positive Keliger's test
*Pain with walking corresponds to painful location with palpation (morise widens during WB) |
|
|
Why do fewer medial ankle sprains occur/ |
Configuration of static stabilizers and joint configuration which prevent excessive ankle eversion |
|
|
What ligament is often sprained in medial ankle sprain? |
Medial ankle sprain |
|
|
What can the medial ankle sprain also be associated with |
Syndesmosis injuries Malleolar fractures |
|
|
What is the signs and symptoms of the medial ankle sprain? |
*TTP medial joint line
*Diffuse ecchymosis and edema/swelling on medial aspect of ankle
*Pain or laxity with the eversion talar tilt test |
|
|
What should you rule out for the medial ankle sprain |
*Medial malleolus fracture (knock off fracture)
Bimalleolar fracture (Pott's fracture) |
|
|
What is a knock off fracture |
If talus everts and rocks into the lateral malleolus can knock off the medial malleolulus |
|
|
What is a pott's fracture |
Bimalleolar fracture
If have knack off fracture through the medial malloelus and a fracture through the lateral malleolar |
|
|
What are complicated injuries of the ankle? |
Fracture and dislocation |
|
|
Will tibia shaft fracutres typically present with gross deformities? |
Yes |
|
|
Does a tibia shaft fracture equire signficant force? |
Yes |
|
|
Can peopel with tibia shaft fractures weight bear? |
No |
|
|
Is there is possiblity for radiating pain on the tibia shaft fractures? |
Yes |
|
|
What sort of leg fractures can rotational stresses cause? |
Fibula spiral fracture |
|
|
Can a person weight bear with a fibula spiral fracture? |
May be able to (limited) |
|
|
Is there swelling in a fibula sprial fracture? |
Yes, localized pain as well as swelling over location of fracture |
|
|
What should you rule out with ankle sprains? |
*Rule out fracture of superior portion of fibula with ankle sprains (Maisonneuve fracture) |
|
|
Does the achilles tendon have good or bad vasularity? |
Poor
Achilles tendon has a portion that is less vascularized than other (~2-6 cm above insertion on calcaneous) |
|
|
Where does the achilles tendon insert |
The tendon twists and inserts slightly medially on the axis of the subtalar joint on the calcaneous |
|
|
Where is the comon site of achilles pathology: tnedinosis or rupture |
Distal avascular zone |
|
|
What is a midsubstance achilles tendinopathy? |
*chronic tendinopathy of the achilles tendon so presents as thicker and can palpate and feel crepitis as person moves
It is acutely swollen around achilles so hard to see the contour of the achilles |
|
|
What is a pump bump |
Exotosis on the achilles tendon |
|
|
What is insertional tendinopathy |
Pain right wehre the achilles tendon inserts on the calcaenous |
|
|
Does a person with midsubstance or insertional achilles tendinopathy have a better prognosis |
Mid substance
Harder to heal insertional |
|
|
What is a partenon of the ahcilles tendon |
Highly vascularized layer surround the achilles tendon that is susceptible to inflammation and forms adhesions to underlying tendon |
|
|
What is the path of tendon rupture |
Paritenonitus Tendinosis (often silent) Tendon rupture |
|
|
What is achilles tendinosis |
Degeneration of tendon midsubstance
Leads to microscopic tears and necrotic areas |
|
|
Is achilles tendinosis often silent |
Yes |
|
|
Is achilles tendinosis visible with a disagnositic ultrasound or MRI? |
Yes |
|
|
What are the precipitating factors for achilles tendinopathy |
*Previou ankle sprain
*Hyperpronation (Continue to overload the achilels more because more tension on medial and achilles mainly work in sagittal plane)
*Tibial varum (Deliver more forces inot the achilles)
*Calcaneovalgus(Part of hyperpronation --> Calcaneous turned laterally)
*Achilles tightness
*Hamstring tightness
*Training errors |
|
|
What is the signs and symptoms of achilles tendinopathy? |
*Burning pain during activity
*TTP
*Palpable nodule
*Visible thickening (If chronic)
*Crepitis with active movement (Scarring between peritenon and achilles tendon) |
|
|
What is the treatment for achilles tendinopathy |
*Eccentric training
*Improve limited DF RoM through stretching and tissue and joint mobilizing
*Taping
*Surgery (Last course of action ot clean out debris) |
|
|
what may cause achilles rupture |
Achilles tendinosis or paratenonitis may lead to rupture but not necessary as precipitating factor |
|
|
Which is achilles rupture more common in? |
Males > 30 yrs old |
|
|
What is the MOI of Achilles rupture |
Forceful contraction (landing from jump, sudden changes in direction) |
|
|
What is the signs and symptoms of achilles rupture? |
*Loud pop (gunshot) at time of injury and person reports feeling that "was kicked in calf"
*Visible defect in tendon
*Absence of palpable in tact tendon
*Excessive edema/ecchymosis
*Positive thompson test
*Can actively plantar flex
*Can walk but can't do a single leg hell raise (can't get enough torque) |
|
|
How long does achilles rupture take to recover? |
7-9 months |
|
|
What is the conservative treatment of achilles rupture |
Immobilization (cast or night splint) 8 weeks |
|
|
Are outcomes better with surgery or conservative management for achilles rupture |
Surgery
*Lower instance of re rupture
*Faster return to pre-injury activity |
|
|
What are medial tibial stress syndromes also called? |
Shin splints |
|
|
What does medial tibial stress syndromes also involve |
Reaction of tissues along the medial border of the distal tibia (periostitis, posterior tibialis tendonopathy, tibial stress fracture)I |
|
|
ARe shin splints an overuse yes |
Yes
Or can be acute response to changes in surface, shoe type, volume of training |
|
|
Why can overpronation also contribute to medial tibial stress syndrome |
Because overloads the posterior tibialis makes change of tension and cause inflammation of the periosteum |
|
|
Do the medial tibial stress syndrome develop gradually? |
Typically |
|
|
Medial tibial stress syndromes have diffuse pain along where? |
Along posterio-medial tibial border during activity |
|
|
What is the treatment during medial tibial stress syndrome? |
Usually responds well to conservative treatement
*Ice *Modified training *Correcting alignement issues *Improved shoe type *Strenghtening of posterior tibialis
(Tape very tight because of gate theory --> But just masking problem)
|
|
|
If the pain of a medial tibial stress syndrom goes from diffuse to focal what should be ruled out? |
Stress fracture of the tibia |
|
|
Where can stress fractures occur? |
Several locations:
Distal tibia Midshaft of tibia Distal fibula |
|
|
What kind of injury is a stress fracture |
Overuse injury |
|
|
How do you diagnosis a stress fracture |
X ray Bone scan |
|
|
What is the signs and symptoms of a stress fracture |
*focal pain on bone *Pan during activity and at rest -"Night pain" *Positive bump test or squeeze test (not always sensitive in early stages) |
|
|
What is the treatemnt for stress fractures |
*Rest *Walking boot *PWB to NWB depending on severity) *Modified conditioning to maintain fitness (Swim Ex) *Bone stimulator *Pulse ultrasound |
|
|
What are the four compartments of the leg? |
*Superficial *Postieror *Deep posterior *Anterior |
|
|
The four compartments of the leg are bordered by what |
Dense fascia and bone |
|
|
The dense fascia are poor elastic properties to accomodate expansion? |
Yes |
|
|
What happens to pressure in compartments as exercise |
Increases because more blood flow |
|
|
Abnormally high pressure in compartments has potential to do what? |
Damage nerves and vessels |
|
|
What happens when comparments have abnoramlly high pressure that exceeds capillary perfusion pressure (Pressure within capillaries that forces blood out to surrounding tissues)? |
Resultsi n ischemia and hypoxia, eventually leads to cell death because can't deliver oxygenated blood to the tissues that need it |
|
|
What are the two types of compartment syndromes? |
*External compartment syndrome (chronic vs acute onset)
*Traumatic compartment syndrome |
|
|
When do the signs and symptoms for the exertional compartment syndrome occur (chornic onset) |
During or after exercise) |
|
|
How long does it take to get to the chronic onset of the exertional compartment syndrome? |
Takes weeks or years |
|
|
What are the signs and symptoms of the exertional compartment sndrome |
Increased fascia thickness inibits venous outflow but not arterial inflow (can take blood into compartment but can't get out) |
|
|
What compartments are most susceptible for the exertional compartment syndrome? |
*Anterior *Lateral *Deep posterior |
|
|
What compartments don't have exertional compartment syndrome? |
*Superficial *Posterior Wh |
|
|
What is different about the acute onset of exertional compartment syndrome? |
Same as s/s for chronic without the prior symptoms or history of tramatic injury |
|
|
What is the sign and symptoms of the exertional compartment syndrome? |
*Pain localized in compartment
*Possible numbness into the toes and / or dorsla and lateral aspect ofoot (anterior or lateral CS)
*Decreased strength of muscles associated iwth compartment
*Pain with passive ROM (stretching does not help)
*Possible visible swelling in compartment
*rEduced or absent pulse (dorsalis pedis) in advanced/extreme cases |
|
|
When is fasciotomy required? |
When the resting pressure is > 15 mmHg
>30 mmHg 1 min post ex
>20 mmHg 5 minutes post exercise |
|
|
Is traumatic compartment syndrome a medial emergency |
Yes could lead to significant muscular necrosis and lose muscle mass that doens't come back |
|
|
What is the MOI for traumatic compartment syndrome |
*Direct blow to the anterior or lateral compartment (most exposed)
*More common in the anterior compartment *May also be present with tibia or fibula fracture |
|
|
What are the signs and symptoms of the traumatic compartment syndrome |
Related to the 5 P's
Pain Pallor Pulselessness Paresthesia Paralysis |
|
|
What are the signs and symptoms of a traumatic compartment syndrome |
Visibally swollen compartment
*Shiny skin (because stretch) *Hard to touch compartment and TTP *Inability to DF ankle or extend toe *Pain with passive ankle ROM (stretch) --> Plantar flexion if anterior compartment *Walking extreme pain *Drop foot (if nerve peralis) *Dorsalis pedis pulse integrity |
|
|
Do you apply compression wraps with traumatic compartment syndromes? |
No
Because will further resist ability of fluid to leave compartment |
|
|
What type of joint is the knee? |
Hinge |
|
|
Why do we need patella? |
Because increases the leverage of the quads and makes it more efficient |
|
|
Is the knee joint more or less stable than the ankle? |
More
Less likely to sprain the ankle because of the ligamentous support (cruciate and collateral ligament) |
|
|
What are the three articulations of the knee? |
Patellofemoral Tibiofemoral Fibulotibula |
|
|
What is the largest diarthrodial joint? |
Tibiofemoral joint |
|
|
How many degrees of freedom does the tibiofemoral joint have? |
3
Flexion/extension Internal/external rotation Abduction/adduction |
|
|
How many voluntary movements does the tibiofemoral joint have? |
2 DOF
Sagittal and transverse plane |
|
|
What is the ranking of ROM (osteokinematics) |
(Greatest to least)
Sagittal plane (140 degrees)
Transverse plane (IR 30 degrees, ER 45 degrees)
Frontal plane (Slight and passive) |
|
|
Will range of motion be greater or less wen measured dynamically during activity? |
Greater |
|
|
Is abduction valgus or varus? |
Valgus |
|
|
Is adduction valgus or varus? |
Varus |
|
|
During knee flexion the tibia _____ rotates on the femur |
Internally |
|
|
During knee extension, the tibia _____ rotates on the femur |
Externally |
|
|
What is the screw home mechanism? |
As the knee approaches terminal extension (last 20 degrees), tibia externally rotates
And when the knee flexes, the tibia internally rotates (important during the swing phase of the gait (unlock knee)) |
|
|
Why does the screw home mechanism occur? |
Because of the femoral condyle curvature (allowing the tibia to glide and slide longer on the medial femoral articulating surface)
Increases the tibia stability on the femur (lockign the knee, tightening the cruciate ligaments) |
|
|
What is the knee flexing and the tibia interally rotating initiated by? |
Popliteus muscle |
|
|
Are medial and lateral femoral condyles convex or concave |
Convex |
|
|
Does the medial or the lateral condyle have a longer articulating surface |
Medial |
|
|
What is more prominent the lateral or medial condyle? |
Lateral |
|
|
Is the tibial plateaul concave or convex |
Concave |
|
|
What is the tibial plateau assisted by? |
Menisci |
|
|
Which tibial plateau is larger the medial or the lateral |
Medial
(The lateral TP is less concave than the medial TP) |
|
|
The convex and concave articulation translations (arthokinematics) provides an additional ___ DOF |
2
-Anterior-posterior -Medial-lateral -Superior-inferior (distraction/compression) |
|
|
When a concave surface moves on a convex surface the concave surface glides and slides in the ____ direction as the osteokinematic motion |
Same |
|
|
When the convex surfaces moves on a concave surface the convex surface glides and slides in the ____ direction as the osteokinematic motion |
Opposite |
|
|
If you flex the knee, the tibia rolls _____ and slides _____ |
Back In same direction |
|
|
In the ankle is the talus convex or concave |
Convex |
|
|
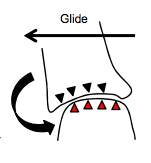
As the ankle goes into dorsiflexion, is the talus gliding posteriorly or anteriorly |
Posteriorly |
|
|
What is the glide of the tibia on the femur during knee flexion |
Glides posteriorly |
|
|
During squatting when the femur is moving the the tibia, what is the direction of the glide |
Femur gliding forward |
|
|
In an open kinetic chain when the talocrural joint is in dorsiflexion, the talus moving on the tibia/fibula is gliding in what direction |
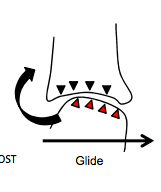
Posteriorly |
|
|
When the talorcural joint goes into squatting and the tibia/fibula is moving on the talus what direction is the glide? |
Anterior |
|
|
What is the consequence of motion without gliding (translatory motion) |
During knee motion, menisci would more likely be pinched between the condyles and tibial plateau which leads to injury |
|
|
Patella displays ____ motion |
Translatory motion |
|
|
What is the patellofemoral arthrokinematic movements: when the knee flexes the patella glides _____ |
Distally (inferiorly) |
|
|
When the knee extends the patella glides ____ |
Posteriorly (superiorly) |
|
|
Is the knee more mobile in flexion or extension |
Patella is very mobile in extension when quads not working on it |
|
|
What is the mechanical advantage of the patella |
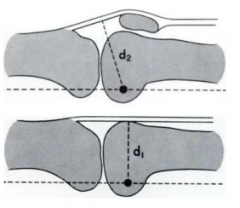
Moment arms for the quads is greater in presence of patella so less quad force required |
|
|
Does the patella offer less or more mechanical advantage when the knee is extended compared to when flexed |
Less |
|
|
What is the patellar tracking movement influenced by? |
Quad contraction and geometry of femoral condyles |
|
|
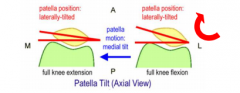
What is the medial and lateral shift of the patella |
C-curve pattern from the knee extension to flexion influencing medial and lateral tilt |
|
|
The patella tilts ____ from extension to flexion |
Laterally |
|
|
Does the contact area of the patella with the femur change as knee flexion changes |
es |
|
|
Why is the patella more mobile in extension |
Because in less contact with femur near extension |
|
|
Patellofemoral joint reaction forces ___ predictably in response to quad muscle force and ____ in knee flexion until about ___ degrees flexion |
*Increase *Increase *70 |
|
|
Do you take the q angle standing or supine |
Standing |
|
|
Is the q angle larger in males and females why? |
Females
Pelvis width/femur length (Men have longer femurs) |
|
|
What lines create the q able |
1) Line from the tibial tuberosity and midpoint of patella
2) Line form midpoint of patella to ASIS W |
|
|
What sort of loading does the MCL resist? |
Valgus loading |
|
|
How many portions does the MCL have? |
2
(Superficial and deep) |
|
|
Where does the deep portion of the meidal collateral ligament go? |
Deep into the joint and inserts on the medial meniscus |
|
|
What kind of size doe sthe medial collateral ligament have |
Broad flat |
|
|
Is the MCL tigher or not when knee is extended |
Tighter |
|
|
What is the MOI for the MCL sprain |
Medially directed force on the lateral aspect of the knee resulting in valgus loading |
|
|
What are the signs and symptoms of the medial collateral ligament sprain |
TTP over the medial apsect of the knee (adductor tubercle to the tibial plateau or mid-substance of MCL)
*Positive valgus stress test (gapping medial joint line, pain)
*Decreased tolerance to AROM knee flexion/extension due to pain and/or swelling (Would especially not like it in extension because extension makes the medial collateral ligament more tense)
*Edema visible on medial aspect of knee (may take time to develop) |
|
|
How are most medial collateral ligaments treated, conservatively or surgically |
Conservatively |
|
|
What is treatment of medial collateral ligament sprains like? |
*Conservatively (Rest, ice, PWB-FWB, progressive rehabilitation)
*Imobilization brace for 2-3 degree injries
*3 degrees sprains can be surgically repaired when in conjunction with an ACL injury |
|
|
Adolescents displaying valgus laxity should be screed for waht |
Epiphyseal plate injuries |
|
|
What kind of shape does the lateral collateral igament have? |
Cord-like |
|
|
Does the lateral collateral ligament connect to the lateral malleolus |
No |
|
|
What kind of loading does the lateral collateral ligament resist |
Varus loading and deformity |
|
|
What is the signs and symptoms of the lateral collateral ligament sprain |
*TTP over lateral aspect of knee on lateral collateral ligament and joint line
*Localized swelling visible on lateral aspect of knee (LCL is extracapsular)
*Positive varus stress test (gapping lateral joint line, pain)
*Decreased tolerance to AROM knee flexion/extension due to pain and/or swelling |
|
|
What do you have to rule out with a lateral collateral ligament |
Fibular head fracture
Common peroneal nerve injury |
|
|
How are most 3rd degree LCL injureis treated |
Surgically (early repair: suture anchors on avulsed site or seqing ends together late reconstruction: Replacing LCL with tendon graft) |
|
|
What is the length of recovery for a mild-moderate lcl sprain |
4-6 wks W |
|
|
hat is the length of recovery for surgical managment of LCL sprain |
WB restriction up to 12 weeks then progress |
|
|
Adolescents displaying varus laxity should be screened for _______ |
Epiphyseal plate injuries |
|
|
ACL is _____articular and ____synovial |
Intraarticular Extrasynovial |
|
|
Will the synovial fluids benefit the anterior cruciate ligament at all? |
No, because it is outside of the synovial capsule |
|
|
What does the anteriro crucial ligament inhibit |
Anterior translation of tibia, intrarotation of tibia and restiricts valgus and varus of the knee |
|
|
What kind of bundle structure does the ACL have? |
Double bundle |
|
|
What are the two bundles of the ACL like in extension |
Parallel |
|
|
What are the two bundles of the acl like in 110 degrees of flexion |
Crossed |
|
|
What is the benefit of having a double bundle structure? |
"Regional Recruitment"
Allows knee to be afforded stability across a larger degree of motion
Because as go into flexion the AMB (anterior medial bundle) tightens while the PLB (Posterior lateral bundle tighens in extension)
Affords support thorugh the full range of knee motion |
|
|
What are the typical mechanism of injury for anterior cruciate ligament injuries? |
Non-contact
(Jump landing, rapid stopping, changes of direction) |
|
|
What is the difference between non contact, indirect and direct contact injuries? |
Non contact: No contact on the knee or from any opponent
Indirect: Actually cotact somewhere just not the knee
Direct: Contact the knee |
|
|
What is the mechanism of injury for the anterior cruciate ligament injuries |
*Valgus *Rotatory loading (tibial rotation-can be both external and internal rotatio) *Agressive quad force (Because will anteriorly translate tibia) |
|
|
In matched sports are females or males more likely to suffer ACL tears |
Femlaes |
|
|
Do males or females suffer more ACL injuries per year comapred to females? Why |
Males, just because there are more sports that males generally play |
|
|
What are the factors to consider when understanding injury risk? |
*Anatomical *Hormonal *Neuromechanical (Neuromuscular and biomechanical)
Neuromuscular = recuritment and activation of muscle and strength differences
Biomechanical = distribution of forces (kinetic and kinematics) |
|
|
What does the factors to consider for understanding injury risk help us determine? |
What do we know? What we need to know? How will we determine.measure what we need to know? How we can intervene and prevent inuries |
|
|
What are the possible anatomical predisposing factors for anterior cruciate ligament injuries? |
*ACL size (Better ot have an increased corsssectional area, to increase strength and ultimate load to failure, females typically have a smaller ACL)
*Femoral intercondylar notch size (Only have so much space availabe because the ACL is nestled in the femoral intercondyler notch. If have smaller notch, tighter, more and less space for the ACL to move around the condyle)
*Pelvic tilt (How much the pelvis rotates back and forth)
*Pelvis width to femoral length ratio
*Joint laxity
*Q angle (line of force of quads)
*Tibial slope (If look at tibia from medial to lateral, tibia has line slope that is slightly posterior, people with an increased posterior slope more likely to tear their ACL) |
|
|
What are the hormonal predisposing factors of ACL injuries |
Menstruation: Estrogen and progesterone |
|
|
What are the neuromuscle predisposing factors for ACL injuries |
*Quad dominance (People who rupture ACL are typically quad dominatn)
*Poor ham strength
*Poor hip strenght (reduciton of femur adduction) |
|
|
What are the biomechanical predisposing factors for ACL injuries |
*Greater knee valgus during task
*Trunk position during task
*Over pronation (Tibial rotation affects the pronation of the foot) |
|
|
What is genu recuvatum? |
Hypermobility
Excessive laxity |
|
|
What is the unhappy tirad |
ACL rupture MCL rupture Medial meniscus tear |
|
|
What are the signs and symptoms of ACL injuries |
*Felt/heard a distinct pop at time of injury *Felt like knee shift *Effusion onset is rapid (hours) *Palpation tenderness can be diffuse: Note pain on posterio-lateral corner of knee or lateral joint line due to concomitatnt bone bruise *Can WB but prefers slight knee bend and shortened stance time *Positive Lachman's and ADT |
|
|
Which is more sensitive the Lachman's Test or the Anterior Drawer Test |
Lachman'sW |
|
|
What does "sensitive" mean |
Less likely to have a false positive |
|
|
When is the anterior drawer test more likely to be useful and positive |
Post acute patient |
|
|
Both lacman's and anterior drawre test will be less likely to be positive after what? |
Several hours of injury due to muscle gaurding |
|
|
Is partial ACL tear (2nd degee) a misnomer? |
Yes, there is still a dysfunction in the ACL such that the knee stability is greatly affected. Surgery is not usually performaed in such a situation; however, it's usually inevitable the partial tear becomes a complete tear over time (return to activity) |
|
|
Is lack of clincial laxity a good predictor of functional ability and stability? |
No
(There are copers and non-copers, 10% are copers |
|
|
What is the early management of anterior cruciatel igament sprain? |
Knee mobilizer PWB progressing ot FWB Reduce swelling Improve ROM and quad function
(Outcomes from the surgery are improved if full ROM and quad tone and function are improved prior to surgery) |
|
|
What is the surgical reconstruction of ACL sprain like? |
7-8 months recovery
*Patella bone-tendon-bone graft (autograft or allograft)
*Hamstring quadrupled bundle graft (autograft)
*Achilles tendon graft (allograft) |
|
|
What are the basic steps of the arthroscopic surgery of the knee for ACL reconstruction |
Tunnels drilled and then debris the knee and then have a little endobutton fixation and then screw fixation between the new and old bone (pulled graft through) |
|
|
Is the ACL surgery an open surgery? |
No |