Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
81 Cards in this Set
- Front
- Back
|
What is the LD50?
|
median lethal dose
calculated dose projected as being likely to cause death in half of exposed animals of species/strain/age/sex exposed |
|
|
How would you extrapolate toxicity data:
a. within the same species? b. to another species? |
a. 10x factor for intraspecies variability
b. 10x factor for interspecies variability = 100x margin b’twn species |
|
|
What are some factors that influence toxicity?
|
dose, duration & frequency of exposure, route of exposure, time of exposure relative to periods of stress, food intake, etc.
animal factors: breed, age, gender, stage of development, physiologic state, health at time of exposure, individual variation environmental factors: air circulation, season, temperature, light, water, diet, housing |
|
|
What are some factors affecting the absorption of an ingested toxicant?
|
absorption site
time substance remains at site pH of stomach or intestinal contents at site |
|
|
What are some factors affecting the absorption of an inhaled toxicant?
|
solubility in blood (high: well absorbed, low: poorly absorbed),
rate & depth of breathing rate of blood flow to lung |
|
|
What is a phase I biotransformation rxn?
Where do they commonly occur? |
body digesting xenobiotic (oxidation, reduction, hydrolysis)
microsome (RER) |
|
|
What is a phase II biotransformation rxn?
Where do they commonly occur? |
addition of functional groups to metabolized xenobiotic
-ex. glucuronide, sulfate conjugation -also acetylation, AA conjugation, glutathione conjugation, methylation cytosol |
|
|
What is the primary route of excretion for toxicants & what types of substances are most easily excreted by this method?
|
urinary
weak organic acids & bases secreted by renal tubules |
|
|
What are 4 main routes by which
toxicants are excreted? |
urinary
fecal (incl. biliary) exhalation milk |
|
|
What are some age related differences that effect absorption of toxicants?
|
intestinal enzyme activity, intestinal motility, & gastric acid secretion are less in neonates than in adults
pre-ruminant vs. ruminant: microbes in rumen metabolize many xenobiotics infant BBB much more permeable than adult infant has lower GFR milk is major source of nutrition for infants: persistent, fat soluble toxicants diseases of old age (↓ GFR, ↓ metabolic capacity) common in dogs, cats, horses |
|
|
What is the result of biotransformation of toxicants?
|
-enhances excretion of substance
-a substance may be biotransformed into a more (bioactivated) or less (detoxified) toxic metabolite -agents that must be bioactivated have delayed onset of signs by a few hours -w/ GI tract absorption & IP injection, blood goes directly to liver: much of substance is biotransformed quickly (1st pass effect) |
|
|
What are some general factors affecting absorption of a toxicant?
|
route of exposure
conc. of substance at site of contact chemical & physical properties of substance |
|
|
What are some important species differences in hepatic metabolism of toxicants?
|
dogs: relatively poor at N-acetylation
swine: little ability to conjugate xenobiotics to sulfate cats: relatively poor at glucuronidation |
|
|
What species has a relatively poor ability to excrete organic acids in urine?
|
dog
|
|
|
What are the goals of management of acutely poisoned animals?
|
stabilize vitals
ongoing clinical evaluation prevent continued exposure to toxicant administer appropriate antidote facilitate removal of absorbed toxicant supportive therapy |
|
|
What drugs would be used to tx toxicant induced:
a. bradycardia? b. metabolic acidosis? c. status epilepticus? |
a. parenteral atropine
b. fluids w/ added sodium bicarb c. IV valium, then IV phenobarb, finally inhaled anesthetic |
|
|
What are some measures used to reduce absorption of toxicants?
|
dilution
emesis gastric/rumen lavage adsorbents cathartics gastrotomy or gastric endoscopy |
|
|
For what type of toxicant might dilution be effective?
|
corrosives
need rapid dilution: use water or milk ASAP |
|
|
What are some contraindications for induction of emesis?
|
dyspnea, hypoxia, seizures, coma, or abnormal pharyngeal reflexes
don’t give emetics if airway is compromised or if animal has ingested agent that can rapidly cause seizures corrosives: ↑ risk of esophageal injury when agent comes back up volatile hydrocarbons: risk of aspiration pneumonia species that cannot vomit: horses, rabbits, rodents --> possible gastric rupture: usually need to do gastric lavage |
|
|
What emetics are preferred for:
a. at home use? b. in clinic use in dogs? c. in clinic use in cats? |
a. syrup of ipecac
b. apomorphine c. xylazine |
|
|
Under what circumstances might you use gastric lavage instead of emesis?
|
animals that can't vomit
cases in which massive ingestions (> LD50) occur if emesis is unproductive, or delayed GI emptying is anticipated |
|
|
How does activated charcoal work to decrease toxicant absorption?
|
used for recent (<6 hr) ingestions
medical grade AC contains large pore sizes & SA which allows for the non-specific binding of many toxicants nonpolar, large molecules are most rapidly adsorbed ionized solutes are less firmly adsorbed than neutral solutes doesn’t work for small organic molecules (ex. some metals, ethanol) |
|
|
How do cathartics work to decrease toxicant absorption?
|
↓ GI transit time --> ↓ absorption
|
|
|
What are 2 main classes of cathartics?
|
saline cathartics: sorbitol
-good media for bacterial growth, harder to obtain than osmotic cathartics osmotic cathartics: preferred -magnesium sulfate (Epsom Salt): can get at drug store; don’t use if injury to BBB: low risk of CNS depression -sodium sulfate |
|
|
Under what circumstances might you use gastrotomy or gastric endoscopy?
|
rarely indicated
may be required to remove FBs from stomach: endoscopy preferred metal ingestions: lead weights, pennies, zinc bolts, etc. large quantities of drugs which form coalesced masses: ex. meprobamate |
|
|
What are 2 measures to enhance elimination of a toxicant?
|
diuresis
ion trapping |
|
|
How would you treat ingestion of a corrosive agent?
|
-dilution: must be rapid (H2O or milk)
-GI protectorants & demulcents to prevent esophageal/gastric ulcers -steroids: controversial -bougienage: balloon procedure to physically destroy esophageal stricture (strictures occur commonly: hard to manage & can’t resect) -NO gastric lavage: could perforate weakened esophagus w/ stomach tube -NO emetics -neutralization CONTRAINDICATED |
|
|
What clinical signs would be expected w/ ingestion of an:
a. acid corrosive? b. alkali corrosive? |
a. oral & esophageal irritation, pain on swallowing, mm burns, epiglottal edema --> dyspnea, esophageal necrosis & stricture
b. -more severe than acids -mm burns, esophageal necrosis/stricture: can occur w/o evidence of injury to oral cavity -button batteries often just sit in esophagus & start to release acid, or may get stuck in stomach: usually require surgical or endoscopic removal |
|
|
How do cardiac glycosides effect the CV system?
|
interfere w/ K, Na, Ca movements --> effect cardiac conduction (muscle contraction)
|
|
|
What clinical signs are associated w/ toxicosis by cardiac glycoside containing plants?
|
o poisoning occurs w/in hours of ingestion
early signs: anorexia, salivation, vomiting (PROJECTILE vomiting should ↑ suspicion), colic CNS depression, weakness, ataxia, paralysis of limbs, coma cardiac arrhythmias terminal seizures, death animals may remain sick for more than 2 days & gradually recover |
|
|
What are some gross lesions assoc. w/ cardiac glycoside poisoning?
|
GI irritation, renal tubular damage (toxic nephrosis), hepatocellular damage very common lesions w/ poisoning in general
|
|
|
What is the tx protocol for cardiac glycoside poisoning?
|
-always monitor EKG: auscultation alone not very helpful
-emetics -activated charcoal & saline cathartic -monitor serum potassium conc. -support respiration -tx arrhythmias: bradycardia (atropine), heart block (phenytoin), tachyarrhythmia (propranolol) -digitalis antibodies (Digibind): work very well, but are expensive -calcium containing solutions CONTRAINDICATED |
|
|
How would one dx cardiac glycoside poisoning?
|
evidence of consumption
clinical signs lesions |
|
|
What plants are known to contain cardiac glycosides or cardiac glycoside like agents?
|
foxglove
monkshood oleander milkweed lily of the valley rhododendron mountain laurel |
|
|
Monkshood
a. species most commonly affected b. common presenting complaint |
a. cattle; emerges in early spring
b. GI signs: often present for bloat |
|
|
Milkweed
a. species most commonly affected |
a. birds that eat catepillars
|
|
|
Rhododendron
a. when during the year do most toxicoses occur & why? |
a. most toxicoses occur in winter & early spring when other forage is unavailable (evergreen)
|
|
|
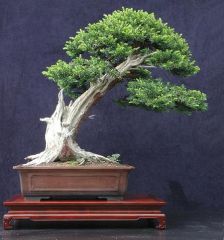
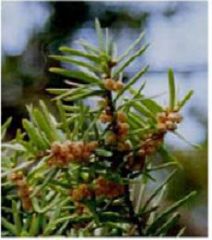
Japanese Yew
a. species most affected b. what toxicant does c. clinical signs d. dx e. tx |
a. monogastric more sensitive (livestock can eat large doses w/ no toxicoses)
b. does NOT act as a cardiac glycoside, but depresses conduction of depolarization thru heart c. indistinguishable from cardiac glycosides d. ID of plant in stomach or rumen contents (needles often survive mastication) & appropriate clinical signs, often incl. death e. -induce emesis -activated charcoal & saline cathartic -atropine to counter CVS depressant effects -maintain body fluid & electrolyte balance |
|
|
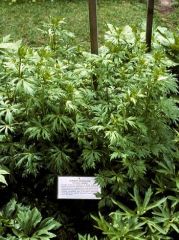
Black Snakeroot
a. species most affected b. clinical signs c. tx d. what part of plant is esp. toxic? |
a. sheep, also cattle, horses, & pigs
b. salivation, nausea, vomiting, muscle weakness, staggering, convulsions, coma, death c. -emetics -activated charcoal & saline cathartic -atropine to tx bradycardia d. bulbs |
|
|
Gossypol
a. species most affected b. what species is relatively unaffected? c. toxicity d. clinical signs e. dx |
a. primarily domestic livestock, esp. immature ruminants & pigs
b. horses c. -toxic effects usually only occur after long term exposure (weeks to months) - conc. in cotton plant affected by plant species, climate, soil type, fertilization d. -acute heart failure resulting from cardiac necrosis -sudden death -dyspnea (d/t CHF) -hepatotoxicity: 1º or 2º to CHF --> icterus -↓ spermatogenesis & sperm motility -green discoloration of egg yolks, ↓ egg hatchability e. -hx of dietary exposure to cottonseed products over a relatively long period -analysis of diet: shipment of feed that causes toxicosis may be gone by time of analysis (sample from bottom of bin & get multiple samples) -compatible clinical sings: sudden death, chronic dyspnea -multiple animals affected |
|
|
Bufo Toad
a. species most affected b. toxicity c. clinical signs d. tx |
a. dogs
b. toxicosis occurs in animals that bite or mouth various species of toads that contain bufotoxin (cardiac glycoside) c. -develop w/in minutes of mouthing toad -profuse salivation, head shaking, ataxia, vomiting, polypnea, hemorrhagic diarrhea, seizures -monitor ECG: can see sinus arrhythmia, tachycardia, occ. V fib d. -wash buccal mucosa w/ swab or hose to dilute toxin -IV diazepam -IV atropine -propranolol -digitalis specific Fab fragment (Digibind) effective |
|
|
ionophores
a. species that is highly susceptible b. other species affected c. species that is relatively resistant d. mode of action |
a. horses
b. cattle, sheep, pigs, dogs c. poultry d. -ionophores create functional membrane pores, allowing cations to bind to ionophores & shuttle back & forth across cell mems -high intracellular Na --> ↑ myocardial cell & diaphragm cell contractility -early: positive inotropy -later: negative inotropy & contracture -skeletal & cardiac m. dysfunction |
|
|
nitrate/nitrite
a. species most affected b. sources c. mode of action |
a. cattle
b. cereal grasses (oats, millet, rye), corn, sunflower, sorghums, fertilizers, soils naturally high in nitrogen, contaminated water, weeds w/ high nitrogen concentrations c. -rumen reduces nitrate (NO3) --> nitrite (NO2) -rapid absorption of NO2 from gut --> oxidation of of Fe2+ in hemoglobin to Fe3+ --> methemoglobinemia (dark brown blood) -methemoglobin can’t bind O2 --> hypoxia, anoxia, death |
|
|
nitrate/nitrite
a. clinical signs b. dx c. tx d. prevention |
a.
-varies from acute death to signs exhibited over days to weeks -rapid onset d/t O2 deficit & ↓ BP -tachycardia, weak heart beat, hypothermia, muscle tremors, weakness, ataxia -tachypnea, severe cyanosis, anxiety, excess salivation, diarrhea, frequent urination -abortions, stillbirths: fetus doesn’t tolerate methemoglobin well b. -dark brown blood -feed or water samples: diphenylamine test or Aquacheck water quality test strip -postmortem: enucleated eye &/or aspirated aqueous humor, CSF c. -1% or 2% methylene blue IV: can cause methemoglobinemia in animals that do not already have methemoglobinemia -mineral oil drench OR 3-5 gallons of cold water (preferred) w/ ABs ↓ rate of nitrate --> nitrite -give gallon of vinegar to ↓ rumen pH --> ↓ conversion of nitrate --> nitrite -vasoconstrictors (epi, norepi) may be helpful d. -maintain animals on good plane of nutrition -avoid excess application of manure or nitrogen fertilizers: wait 24-48 hours to put animals out -don’t overstock pasture -delay harvesting any stressed forages |
|
|
ionophores
a. clinical signs b. dx c. causes of poisoning d. uses of ionophores in livestock |
a.
-latent period: varies w/ species, host factors, dose ingested -signs appear w/in 12-72 hours -usually not many noticeable CV signs -horses: sweating, muscle tremors, pacing -anorexia, cardiac failure (tachycardia), dyspnea, stiffness, muscle weakness, ataxia, diarrhea, recumbency, myoglobinuria, sudden death seen in most species -deaths may occur long after acute exposure & apparent recovery d/t cardiac fibrosis b. hx of exposure (ex. change in feed) --> get feed analysis, characteristic clinical & pathologic signs (myocardial necrosis, pulmonary congestion, skeletal muscle lesions similar to nutritional myopathy) c. -generally results from exposure to undiluted premixes -misformulation of feed: too much of ionophores added -animal eats feed meant for a different species: ex. horses much more sensitive than cattle d. -used to control bloat & acidosis -control of coccidiosis in cattle -↑ feed efficiency -inhibits certain rumen bacteria -influences energy & nitrogen metabolism thru changes in rumen fermentation -used to ↓ likelihood of acute bovine pulmonary emphysema & edema |
|
|
copper toxicosis: acute
a. species affected b. causes c. clinical signs |
a. calves, young sheep
b. accidental administration of excessive amounts of soluble copper salts: anthelmintic drenches, mineral mixes, improperly formulated rations, young calves or sheep injected w/ soluble forms of copper c. -may result in death: may be able to detect icterus in animals that die suddenly -severe gastroenteritis: abdominal pain, diarrhea, anorexia, dehydration, shock --> erosions & ulcerations in abomasum of ruminants -if animal survives, hemolysis & hemoglobinuria develop after 3 days -centrilobular hepatic necrosis --> icetrus -animals that survive acute episode may die of subsequent renal failure: iron in hemoglobin damages kidneys |
|
|
copper toxicosis: chronic
a. species affected b. mode of action c. causes |
a. sheep
b. -toxicosis remains subclinical until animal is stressed --> copped stored in liver is released in massive amounts --> systemic circulation --> hemolytic crisis -possible stressors: transport, lactation, strenuous exercise, deteriorating plane of nutrition, ingestion of hepatotoxic plants -blood copper conc. ↑ suddenly --> lipid peroxidation & intravascular hemolysis c. -may occur in sheep that ingest cattle rations, which contain higher levels of copper, or when their water is supplied via copper plumbing -chronic toxicosis more likely to occur w/ low dietary intake of molybdenum & sulfur |
|
|
copper toxicosis: chronic
a. clinical signs b. characteristic gross lesion c. dx c. tx |
a.
-CNS depression, weakness, recumbency, rumen stasis, anorexia, thirst, hemoglobinuria, icterus -methemoglobinemia, hemoglobinuria, anemia -several days to weeks before hemolytic crisis, liver enzymes are usually ↑ -herd morbidity often < 5%, but >75% of affected animals usually die -losses may continue for up to 2 mo. after dietary problem corrected b. gunmetal blue kidneys c. -↑ copper concentrations measured in liver, kidney, blood -signs of hemolysis, liver failure, & nephrosis -test multiple animals from herd d. -copper chelation: d-Penicillamine: binds to many metals & enhances excretion - dietary supplementation w/ zinc acetate may ↓ copper absorption -fluid therapy -may have poor px in animals undergoing active hemolytic episode |
|
|
copper hepatopathy (dogs)
a. breeds affected b. mode of action c. clinical signs |
a. Bedlington terriers, Westies, Skye terriers, Dobermans
b. Bedlington terriers have autosomal recessive trait: up to 65% affected -have abnormal copper binding proteins c. -may have mild anemia & hemolysis, abnormal coag profile -liver enzymes may be ↑: varies w/ stage of dz -blood copper levels: normal to elevated -dogs w/ hemolytic crisis: hyperbilirubinemia, bilirubinuria |
|
|
copper hepatopathy (dogs)
a. dx b. tx |
a.
-↑ copper conc. in liver measured on bx sample -↑ blood copper conc.: use green top tube -histopath changes: hepatic necrosis, cirrhosis, copper stain b. -low copper diet -copper chelation: d-penicillamine: often needed for life of animal -zinc supplementation: zinc acetate -ascorbic acid supplementation: MAY ↓ cooper absorption (not proven) |
|
|
molybdenum
a. species most effected b. clinical signs c. tx |
a. cattle, sheep
b. Teart: effusive diarrhea, anemia, poor growth, joint deformities c. copper or sulfate in diet |
|
|
acetaminophen
a. species most affected b. mechanism of toxicosis |
a.
-cats: have low levels of glucuronyl transferase needed for glucuronide conjugation -dogs: those w/ < 30% of normal hepatic glutathione b. -conjugated w/ glucuronide, sulfate, or glutathione -when conjugation capacity reached --> production of toxic metabolites (hepatotoxic) |
|
|
acetaminophen
a. clinical signs: cats b. clinical signs: dogs |
a. CNS depression, vomiting, dyspnea, methemoglobinemia (brown blood), swelling of face & paws (w/in hours of exposure), icteric or “muddy” mm, Heinz body anemia, hepatic necrosis (w/in days of exposure)
b. -initial phase (2-24 hours): anorexia, vomiting, nausea -asymptomatic phase: abnormal liver enzymes -3-5 days post ingestion: hepatic necrosis --> liver failure (icterus) -7-8 days post ingestion: recovery |
|
|
ddx for methemoglobinemia in small animals
|
-acetaminophen: facial swelling unique (cats)
-onion -naphthalene: moth balls, "snake away" -local anesthetics: ex. overuse of lidocaine during intubation in cats -resorcinol |
|
|
acetaminophen
a. tx |
a.
-recent ingestion (< 2 hours): emetic, activated charcoal +/- saline or osmotic cathartic -oxygen supplementation: O2 cage -n-acetylcysteine (mucomyst): most effective if given w/in 16 hrs of ingestion -supplement for glutathione --> ↑ conjugation of drug -ascorbic acid (oral or parenteral): given up to QID (injection painful: acidic) |
|
|
Black Snakeroot (Death Camus)
|

Name the plant.
|
|
|
Black Snakeroot (Death Camus)
|

Name the plant.
|
|
|
Black Snakeroot (Death Camus)
|

Name the plant.
|
|
|
Black Snakeroot (Death Camus)
|

Name the plant.
|
|
|
Black Snakeroot (Death Camus)
|

Name the plant.
|
|
|
Foxglove
|

Name the plant.
|
|
|
Foxglove
|

Name the plant.
|
|
|
Foxglove
|

Name the plant.
|
|
|
Japanese Yew
|

Name the plant.
|
|
|
Japanese Yew
|
Name the plant.
|
|
|
Japanese Yew
|

Name the plant.
|
|
|
Japanese Yew
|
Name the plant.
|
|
|
Japanese Yew
|

Name the plant.
|
|
|
Japanese Yew
|

Name the plant.
|
|
|
Lily of the Valley
|

Name the plant.
|
|
|
Lily of the Valley
|

Name the plant.
|
|
|
Lily of the Valley
|

Name the plant.
|
|
|
Lily of the Valley
|

Name the plant.
|
|
|
Monkshood
|
Name the plant.
|
|
|
Monkshood
|

Name the plant.
|
|
|
Monkshood
|

Name the plant.
|
|
|
Oleander
|

Name the plant.
|
|
|
Oleander
|

Name the plant.
|
|
|
Rhododendron
|

Name the plant.
|
|
|
Rhododendron
|

Name the plant.
|
|
|
Rhododendron
|

Name the plant.
|