Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
90 Cards in this Set
- Front
- Back
|
What are the findings of a thoracic aortic aneurysm or rupture on plain film
|
displacement of NGT or trachea
depression of the left main stem bronchus apical cap indirect signs such as fx |
|
|
Is an intimal flaps seen sometimes in pseudoaneurysms
|
no
|
|
|
Where is the catheter from when performing an aortic angiogram
|
right subclavian artery
|
|
|
What are the angiographic findings of a traumatic pseudoaneursym
|
indistinct borders
delayed wash out of contrast intimal tear |
|
|
What is the differential diagnosis of a traumatic pseudoaneuryms
|
ductus diverticulum
|
|
|
What does a ductus diverticulum look like
|
a smooth anteromedial outpouching
|
|
|
Where do pseudoaneurysms most commonly occur
|
at the aortic isthmus (distal to the left subclavian)
|
|
|
Why do pseudoaneurysms occur at the aortic isthmus
|
the ascending aorta is fixed and decelerates more rapidly that the descending aorta
|
|
|
What are the 2 options for treatment of surgical and endovascular repair of traumatic aortic injury
|
surgical repair
endovascular repair |
|
|
What is the ddx of a aortic aneurysm
|
post-traumatic
atherosclerotic mycotic congenital syphylittic idiopathic |
|
|
Do thoracic aortic aneurysms have a higher rate of rupture than an abdominal aortic aneurysm
|
yes
|
|
|
What tends to happen to the true lumen in a dissection
|
they tend to become compressed by the false lumen
|
|
|
Is there usually delayed filling of the false lumen
|
yes
|
|
|
What is the debakey classification of thoracic aortic aneurysms
|
-1=ascend and descend
-2=ascending only -3=descending only |
|
|
What is the Stanford classificaion
|
A=Ascending involved
B=Ascending not involved |
|
|
What is the main option if a dissection involves the ascending aorta
|
surgery
|
|
|
What is the treatment of a descending aortic dissection
|
medical treatment
|
|
|
If there is involvement of branch vessels what is the treatment
|
surgery
|
|
|
When is the best time to look for a graft leak
|
delayed images
|
|
|
What type of endoleak is the result of retrograde filling
|
type 2
|
|
|
What is the treatment of a type 2 endoleak
|
to coil the branch vessel
|
|
|
What is the treatment of an acute SMA embolus
|
operative embolectomy
|
|
|
What are 2 causes of acute visceral ischemia
|
embolic
thrombotic (hypercoaguable) |
|
|
What are the causes of chronic visceral ischemia
4 |
stenosis at orgin of celiac or SMA
atherosclerosis median arcuate ligament syndrome FMD |
|
|
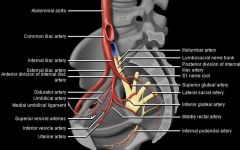
vessels of the internal iliac artery
|
|
|

|

|
|
|
Where are the middle colic , right colic arteries and ileocolic artery
|
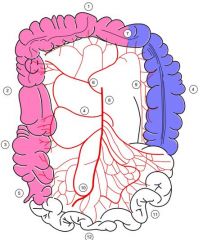
middle colic -6
right colic- 4 ileocolic- 10 |
|
|
Where is the marginal artery
|
#9
|
|
|
What is the marginal artery
|
also known as the marginal artery of Drummond and artery of Drummond (named after Sir David Drummond (1852-1932) an English physician),[1] is a blood vessel that anastomoses (connects) the inferior mesenteric artery (IMA) with the superior mesenteric artery (SMA). It is sometimes absent, as an anatomical variant.
|
|
|
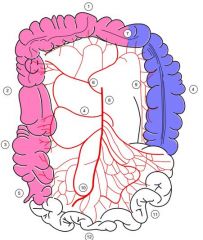
Where are the left colic, and hemorrhoidal arteries
|
|
|
|
Is it important to obtain a lateral when viewing the abdominal aorta
|
yes, it makes it easier to see the celiac, sma and ima
|
|
|
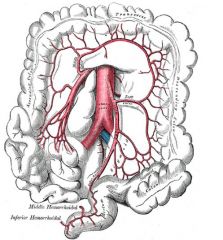
What vessel is involved in collateralization of the abdomen in chronic mesenteric ischemia
|
the marginal arteries run between the ima and sma
|
|
|
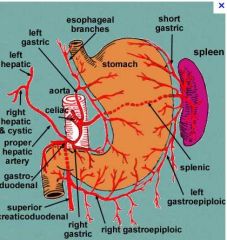
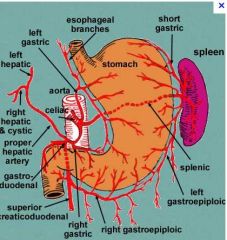
What is the collateral vessels of the celiac and sma
|
pancreatico doudenal arteries
|
|
|
What are the arteries of the celiac axis
|
|
|
|
Where are the pancreaticodoudenal arteries located
|
|
|
|
Can vessels from the internal iliac vessel sometimes feed the IMA via retrograde flow
|
yes
|
|
|
Can FMD go into the branch vessels of the renal arteries
|
yes
|
|
|
What percent of renovascular htn are caused by FMD
|
only 1/3rd
|
|
|
What percent of FMD are bilateral
|
2/3rds
|
|
|
What is the more common side if FMD is unilateral
|
the right side
|
|
|
What are the 3 types of fibrodysplasia
|
medial fibrodysplasia (85%)
perimedial fibroplasia (10%) intimal fibroplasia (5%) |
|
|
What is the tx of fmd
|
balloon angioplasty
|
|
|
What type fibrodysplasia causses web like stenosis
|
intimal fibroplasia
|
|
|
what is the ddx of web-like stenosis of the renal artery in a young person
|
intimal fibroplasia
connective tissue disease vasculitis dissection mimmicking an aneurysm |
|
|
What is typically seen distal to the web-like stenosis in a pt with intimal fibrodysplasia
|
post stenotic dilation
|
|
|
What is the treatment for a GI bleed
|
microcatherization
coil embolization |
|
|
What is the treatment of bilateral renal artery stenosis
|
bilateral renal stents
|
|
|
What percent of pts improve there htn with stents in renal artery stenosis
|
>60%
|
|
|
What are the arteries of the leg
|
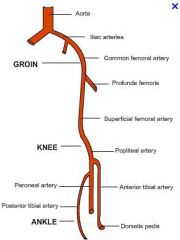
NOTE COMMON FEMORAL IS FROM THE EXTERNAL ILIAC
|
|
|
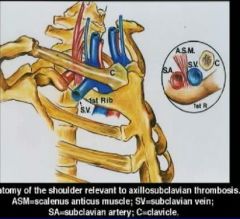
What is thoracic outlet syndrome
|
compression of brachial plexus, subclavian artery, or subclavian veins by bones or muscles of the thoracic outlet (scalene, pectoralis, clavicle, first rib)
|
|
|
What are the SS of thoracic outlet syndrome
|
unilateral upper extremity pain, swelling or ischema
|
|
|
What are 2 complications of thoracic outlet syndrome
|
post-stenotic aneurysm or distal emboli
|
|
|
What is the anatomy of TOS
|
|
|
|
What is the treatment of arterial TOS
|
surgical decompression by first rib resection
|
|
|
What is another name for venous thoracic outlet obstruction
|
paget schroetter syndrome
|
|
|
What is seen in paget schroetter syndrome
|
extensive venous collateralization
|
|
|
What is the treament of venous TOS
|
angioplasty, thombolysis, 1st rib resection
|
|
|
What is subclavian steal syndrome
|
Retrograde vetebral artery flow with transient neurologic symptoms related to cerebral ischemia
|
|
|
What are the findings in late angiographic images
|
reconsititution of flow in the left subclavian secondary to flow from the vetebral artery
|
|
|
What is the treatment for subclavian steal
|
angioplasty Vs stent (controversial)
complete occlusion is treated with bypass |
|
|
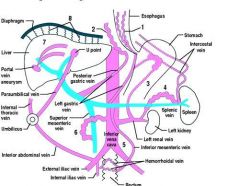
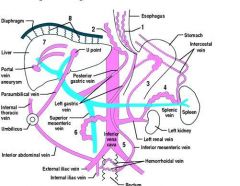
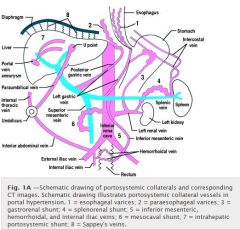
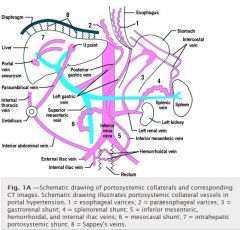
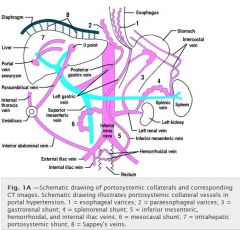
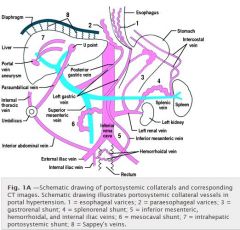
What is the anatomy of portosystemic shunts
|
|
|
|
Where do paraesophageal varices come frome
|
|
|
|
Where are sappeys veins
|
|
|
|
Does the umbilical vein get canulated via the left portal vein
|
yes
|
|
|
What feeds the esophageal varices
|
|
|
|
What are the 2 shunts off the left renal vein
|
|
|
|
What is the coronary vein also known as
|
the left gastric vein
|
|
|
What is the clinical triad of budd-chiari syndrome
|
RUQ pain
ascites hepatomegaly |
|
|
What are the findings of budd chiari syndrome
|
hepatic outflow obstruction (spider web appearance of collateral vessels)
|
|
|
What is a secondary finding of cudd chiari
|
spider web appearance of intrahepatic collaterals
|
|
|
How is budd chiari tx
|
pta or stent
|
|
|
Is budd chiari an indication for TIPS
|
yes
|
|
|
What is may thurner syndrome
|
left iliac vein stenosis (due to crossing of right iliac artery)
|
|
|
What is the treatment for May Thurner Syndrome
|
thrombolysis and then stenting
|
|
|
What is the criteria for eligibility of liver transplant
|
. To be eligible for a transplant, a patient must have fewer than four tumors, with no single tumor greater than three centimeters in diameter, and must have had no cancer outside the liver in the last six years.
|
|
|
What are the factors associated with poor prognosis of survival with liver cancer
|
Factors associated with poor prognosis for overall patient survival include Child-Pugh class B or C, tumor size ≥4 cm, 5 or more tumors, portal vein invasion, and an alpha fetoprotein (AFP) level >83 ng/mL
|
|
|
Is portal vein thrombosis a relative contraindication to chemoembolization
|
yes
|
|
|
Does chemoembolization and radiofrequency ablation increase the life expectancy in pts with liver cancer
|
yes, up to 3 times longer
|
|
|
When should radiofrequency ablation be used
|
should be used in patients with early-stage HCC with up to 3 lesions with a tumor diameter of ≤ 3 cm and for patients with nonresectable liver metastasi
|
|
|
When is a follow up scan of chemoembolization obtained
|
10-14 days after the procedure
|
|
|
When is polyvinyl alcohol embolization commonly used
|
carcinoid syndrome
|
|
|
How and why is a preprocedure angiogram performed prior to chemoembolization
|
Angiography is usually performed by placing a 5F to 6F catheter through a sheath via the right or left femoral artery. The catheter should be able to accept the insertion of a 3F coaxial microcatheter. A celiac-axis and superior mesenteric angiogram is first obtained to identify common variations in the blood supply to the liver and to check for patency of the portal vein.
|
|
|
Why is the chemotherapy used in chemoembolization so effective
|
there are very high levels of chemo
|
|
|
What are the 2 parts of chemoembolization
|
chemo
embolization |
|
|
How are the candidates for chemoembolization
|
pt with primary or metastatic liver tumors that are not resectable (to prolong life)
Pt on transplant list who need to have a tumor reduced in size |
|
|
What is the most common type of metastatic liver tumor treated with chemoembolization
|
carcinoid
|
|
|
What are the side effects of chemoembolization
|
pain
fatigue decreased appetite fever bleeding infection hairloss bonemarrow suppression |
|
|
What are the 2 common agents used for chemoembolization
|
cisplatin
doxorubicin |
|
|
What is the embolic agent
|
iodiodal
|
|
|
Are patients typically admitted overnight following chemoembolization
|
yes
|