Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
385 Cards in this Set
- Front
- Back
|
Motor Behaviors Involve the Entirety of the CNS
|
Spinal Cord - protective reflexes, locomotion generator
Cerebellum - breathing, chewing, swallowing, eye movements Cerebral Cortex - fine motor skills (speech, hand-finger control) Brainstem Basal ganglia - eating and drinking |
|
|
Direct Motor Pathways
|
Nerve impulses for precise, voluntary movement
Three tracts: lateral corticospinal, corticobulbar, anterior corticospinal Somatic = Voluntary = Skeletal Muscle Motor Cortex: contains upper motor neurons The primary motor area of the cerebral cortex is responsible for initiation of voluntary movements (area 4, precentral gyrus) Spinal cord contains lower motor neurons A.K.A - alpha motor neurons. These neurons actually connect to skeletal muscle |
|
|
Spinal Cord
|
Dorsal (posterior) = sensory
Ventral (anterior) = motor Outer Layer: white matter, fiber tract = axons and their myelin Inner Layer: gray matter, neuronal cell bodies and dendrites Ascending and Descending Motor Tracts |
|
|
Ascending Sensory Tracts
|
Sensory
Afferent pathway - axons that conduct nerve impulses from the spinal cord toward the brain |
|
|
Descending Motor Tracts
|
Motor
Efferent pathway - axons that carry nerve impulses away from the brain down the spinal cord |
|
|
Direct Motor Pathway --> Path Taken
|
Motor Cortex --> Corona Radiata --> Internal Capsule --> Crus Cerebri (midbrain) --> Basal Pons (pons) --> Pyramids (Medulla Oblongata) --> Corticospinal Tracts (Lateral and Ventral - anterior) [spinal cord] --> Ventral Horn --> Ventral Roots --> Peripheral Nerves --> Skeletal Muscle
|
|
|
Premotor Cortex
|
think about moving
|
|
|
Primary Motor Cortex
|
actual movement
Upper Motor Neurons - essential for planning, initiating, and directing sequences of voluntary movement |
|
|
Corona Radiata
|
Axon fibers exit the motor cortex using the this (use it for travel)
Condenses into internal capsule (V-shaped condensation of motor fibers) |
|
|
Internal Capsule
|
3 Limbs
Anterior Limb (A) - sensory Posterior Limb (P) - motor, trunk, and extremities (stroke = trunk) Genu (g, bend) = motor, brain stem (if stroke occurs, trouble moving head and neck if this part is damaged) 5 total limbs of internal capsule, the other two are sensory |
|
|
Corticonuclear Tracts (AKA - corticobulbar)
|
motor cortex to skeletal muscles of head and neck to coordinate precise, voluntary movements, travel in genu of internal capsule
Bulb = brain stem Lower Motor Neurons = motor nuclei of cranial nerves III, IV, V, VI, VII, IX, XI, and XII Discrete voluntary (somatic) movement of muscles of neck, larynx, tongue, head and face Axons travel through corona radiata, genu of the internal capsule and crus cerebri Axons cross midline at the level of the motor nucleus they innervate (lower motor neurons, no discrete decussations) Innervate head and neck muscles via the cranial nerves Unlike spinal cord, innervation is often bilateral |
|
|
Crus Cerebri
|
continuation of the posterior limb of the internal capsule
Located in the midbrain Goes to the basal pons (located in the pons) to the medulla oblongata where it enters the pyramids |
|
|
Pyramids
|
Defines the border between the spinal cord and the medulla oblongata
Pyramidal Decussation defines the transition between the brainstem and the spinal cord 3/4 of the axons cross the midline |
|
|
Lateral Corticospinal Tracts
|
Motor cortex to skeletal muscles of the OPPOSITE side of the body
Precise, voluntary movements of the arms and legs (distal part of free limbs) Right side of the brain controls the left side of the body Fibers cross at PYRAMIDAL DECUSSATION |
|
|
Anterior (Ventral) Corticospinal Tracts
|
Motor cortex to skeletal muscles of both sides of the body
Responsible for trunk movements Half side of the cords cross Approximately half of the fibers cross at the PYRAMIDAL DECUSSATION and half do not Synapse in the ventral horn (alpha motor neurons) Alpha motor neurons project their axons via the ventral roots |
|
|
Indirect Motor Pathways
|
Provide input to lower motor neurons from motor cortex to motor centers in the brainstem
4 Descending Pathways Vestibulospinal Tracts: ORIGINATE: vestibular nuclei, pons, and medulla and INSERT in the Reticulospinal Tracts: reticular formation found throughout brain stem Tectospinal Tract: superior colliculi, midbrain Rubrospinal Tract: red nucleus, midbrain |
|
|
Medial and Lateral Vestibulospinal Tracts
|
Vestibular nuclei, pons, and medulla
Inner ear information Tells the person where they are in space Reflexive regulation of balance and posture Originate in vestibular nuclei |
|
|
Medial Vestibulospinal Tracts
|
descend bilaterally through cervical segments of spinal cord and influences neck musculature
|
|
|
Lateral Vestibulospinal Tract
|
descends to lumbar-sacral segments of spinal cord
|
|
|
Reticulospinal Tracts
|
Origin: reticular formation found throughout brain stem (specifically pons and medulla)
Functions to set muscle tone (adjust posture) in anticipation of a movement Found at all levels of the spinal cord - would be a lot slower without it |
|
|
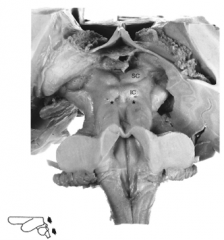
Tectospinal Tract
|
mediates reflexive movement of head and neck in response to sensory stimuli (predominantly vision and hearing)
Originates in the superior colliculus (SC, midbrain) and descends through cervical levels of the spinal cord |
|
|
Rubrospinal Tract
|
Midbrain of brain stem
Regulates muscle tone in upper limbs Ex. putting hands out when falling Originates in red nucleus (R) of the midbrain then crosses at the level of the nucleus Descends through cervical spinal cord, following a pattern similar to the corticospinal tract |
|
|
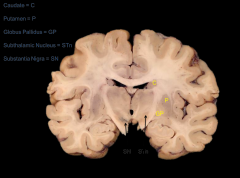
Nuclei Include:
|
Caudate Nucleus and Putamen --> Striatum
Globus Pallidus --> Pallidum Substantia Nigra --> Brain Stem Subthalamic Nucleus --> Diencephalon |
|
|
Basal Nuclei
|
collection of interconnected subcortical nuclei that function as a central link in the part of the motor system that translates the desire to move (mentation, i.e. thinking) into action
"Organ of Habit" "Selects" desired behaviors and "inhibits" unwanted behaviors (unwanted = trimmers) They remember/involved in habits |
|
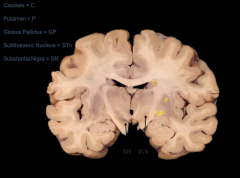
Basal Nuclei - Frontal Plane
|
|
|
|
Basal Nuclei - Loop
|
Works in a loop:
The cortex projects to the striatum (caudate and putamen) which projects to the golubus pallidus and the substantia nigra. The substantia nigra projects back to the striatum |
|
|
Cerebellum
|
maintains proper posture and balance and is activate in learning and performing rapid, coordinated highly skilled movements
Each cerebellar hemisphere influences movements on the ipsilateral (same) half of the body |
|
|
How does the Cerebellum Work?
|
Monitors intentions for movement by receiving impulses from the motor cortex and basal nuclei via the pontine nuclei
Monitors actual movement by receiving input from proprioceptors in joints and muscles that reveal what is actually happening Compares the command signals with sensory information If there is a discrepancy between intended and actual movement, sends out corrective feedback to upper motor neurons |
|
|
Cerebellum Anatomy
|
10% of the brain's mass, but contains 50% of the neurons
Consists of a cortex, underlying white matter and deep nuclei Contains 5 different neuronal types Is attached to the brain stem by 3 paired peduncles sits in the posterior cranial fossa, beneath the tentorium cerebelli |
|
|
The Cerebellar Peduncles
|
the cerebellum forms the roof of the 4th ventricle
The cerebellum is removed from the brain stem by cutting through the peduncles Superior, middle, inferior cerebellar peduncle |
|
|
Superior Cerebellar Peduncle
|
main outflow, fibers project to motor cortex
|
|
|
Middle Cerebellar Peduncle
|
fibers enter from the pons
|
|
|
Inferior Cerebellar Peduncle
|
fibers enter from the medulla and spinal cord
|
|
|
Superior Surface of the Cerebellum
|
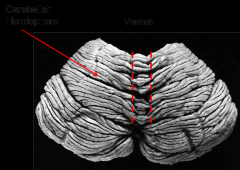
Vermis (wormlike) - the midline region of the cerebellum
The hemispheres, left and right, are on either side of the vermis |
|
|
Inferior Surface of the Cerebellum
|
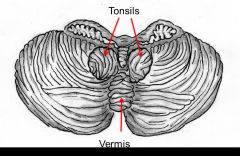
Tonsils - lobules of the hemisphere that lie above the foramen magnum
They may be herniated through the foramen magnum by increased intracranial pressure This is bad, why? - increase pressure - herniate and die |
|
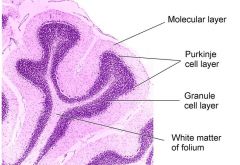
Cerebellar Cortex
|
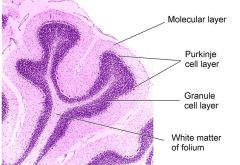
Folds = folia
Molecular layer - lots of connections, few neurons Purkinje cell layer - projects to deep nuclei - cells are huge and dendrites are in 1 plane (flat) Granula cell layer - lots of connection |
|
|
Deep Cerebellar Nuclei
|
out via the superior cerebellar peduncle
Purkinje cells communicate with this |
|
|
Loss of Cerebellar Function
|
does not result in paralysis or inability to initiate movement. Rather cerebellar diseases produces disturbances in the coordination and fine control of movements and posture
|
|
|
Diseases of the Motor System (Cerebellum)
|
Parkinson's Disease
Huntington's Disease ALS (upper and lower) - Lou Gehrig's Disease Stroke |
|
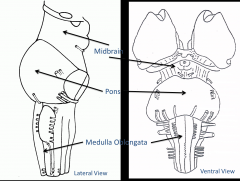
Brainstem
|
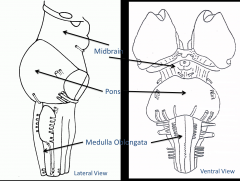
Midbrain
Pons Medulla Oblongata |
|
|
Medulla Oblongata
|
Transition from spinal cord to brainstem
Ventral Surface: Pyramid and Olivary eminence Dorsal Surface: covered by cerebellum Cranial Nerves: IX, X, XI, and XII |
|
|
Pons
|
floor of fourth ventricle
Cranial Nerves V, VI, VII, and VIII |
|
|
Ventral Surface of Midbrain
|

Crus cerebri, cranial nerves III and IV
Other landmarks: Optic chiasm, mammilary bodies, infundibular Stalk |
|
Dorsal Surface of Midbrain
|
Dorsal Surface:
Tectum - superior and inferior colliculi (2 each), cerebral aqueduct, pineal gland |
|
|
Olfactory (I) Nerve
|
Entirely sensory
Extends from olfactory mucosa of nasal cavity to olfactory bulb Projects directly to limbic cortex Sense of smell |
|
|
Optic (II) Nerve
|
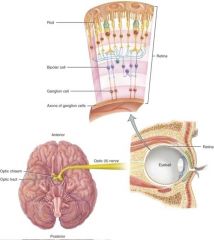
Entirely sensory
Carries signals from neural retina to thalamus Half of the information crosses to the contralateral thalamus and cortex Half project to ipsilateral thalamus and cortex Crossing occurs at the optic chiasm Conduct nerve impulses for vision In sequence, visual signals are relayed from rods and cones to bipolar cells to ganglion cells |
|
|
Oculomotor (III) Nerve
|
Innervates extrinsic muscles of the eye
Levator palpebrae - raises eyelid (loss = ptosis) - could be somatic Somatic - 4 extrinsic eye muscles Parasympathetic (visceral) - 2 intrinsic eye muscles Ciliary muscle and sphincter pupillae - these muscles allow for accommodation for near vision (changes shape of lens during reading) - constriction of pupil |
|
|
Trochlear (IV) Nerve
|
Somatic = 1 extrinsic eye muscle
Superior oblique eye muscle - loops around a bony hook = trochlea, hence it's name Nerve wraps around the pons - comes up dorsally and wraps around (only one that does that) |
|
|
Trigeminal (V) Nerve
|
Motor and sensory
Motor: muscles of mastication Sensory: face and oral cavity 3 Branches: Ophthalmic - sensory Maxillary - sensory Mandibular - sensory and motor |
|
|
Abducens (VI) Nerve
|
Motor
Somatic - 1 extrinsic eye muscle - lateral rectus: abducts the eye (lateral rotation) |
|
|
Facial (VII) Nerve
|
Motor (somatic) - muscles of facial expression
Parasympathetic (visceral) - salivary glands, nasal and oral mucosa, lacrimal glands Sensory: taste, anterior 2/3's of the tongue |
|
|
Vestibulocochlear (VIII) Nerve
|
Cochlear branch: carries auditory information from cochlea
Vestibular branch: carries information concerning blance from the vestibular apparatus and semicircular canals |
|
|
Gloosopharyngeal (IX) Nerve
|
Motor (somatic) Stylopharyngeus muscle (lifts throat during swallowing)
Parasympathetic - parotid gland (secretes saliva) Sensory - sensation and taste posterior 1/3 of tongue |
|
|
Vagus (X) Nerve
|
Sensory and motor
Motor: parasympathetic to thoracic and abdominal viscera, innervates gut to the splenic flexure Sensory: same distribution as motor - convey sensations such as hunger, fullness, and discomfort from thoracic and abdominal organs |
|
|
Accessory (XI) Nerve
|
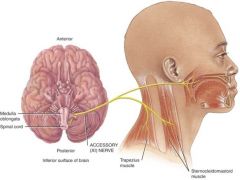
Motor: somatic (voluntary)
Cranial portion arises in the medulla and innervates skeletal muscle of the larynx and soft palate Spinal portion arises in the cervical spinal cord and innervates the sternoclediomastoid and trapezius muscles |
|
|
Hypoglossal (XII) Nerve
|
Motor: somatic
Intrinsic muscles of the tongue |
|
|
Lower Motor Neurons
|
alpha motor neurons that extend out of the brain stem and spinal cord to innervate skeletal muscles in the head and body - provide output from the CNS to skeletal muscle fibers
|
|
|
Upper Motor Neurons
|
essential for planning, initiating, and directing sequences of voluntary movements
|
|
|
Cardiovascular System
|
Blood, heart, and blood vessels
Interstitial Fluid Single-cell systems - do not have cardiovascular system |
|
|
Blood
|
matrix with connective tissue - blood's matrix is plasma (fully fluid)
Cellular component - maintains the matrix |
|
|
Interstitial Fluid
|
surrounds a body of cells
nutrients and waste move between the blood and the interstitial fluid and from there the interstitial fluid and the internal cell Want to move nutrients through interstitial fluid |
|
|
Hematology
|
study of blood, blood-forming tissues, and their disorders
|
|
|
Functions of Blood
|
Transportation
- Gases, nutrients, wastes, hormones Regulation - pH, temperature, water balance Protection - Clotting, immune |
|
|
Physical Properties of Blood
|
"thicker" than water - high viscosity
38 degrees C (100.4 F) pH: 7.35 - 7.45 ******** Color: red (oxygenated) <--> purple (deoxygenated) Typically 8% total body weight Volume: Men - 5-6 liters (1.5 gal) Women - 4-5 liters (1.2 gal) |
|
|
Blood Components
|
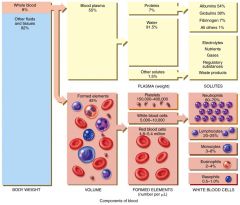
Blood plasma (55%) - top layer
- Water (and solutes) - Proteins - Albumins, globulins, fibrinogens, immunoglobulins Formed Elements (45%) - bottom layer - Leukocytes (WBC's) - Thrombocytes (platelets) - Erythrocytes (RBC's) - very bottom layer Middle layer during centrifusion has DNA |
|
|
Albumins
|
smallest and most numerous of proteins
Responsible for colloid osmotic pressure; major contributors to help blood viscosity; transport hormones (steroid), fatty acids, and calcium; help regulate blood pH Different from other proteins because they are not glyclocylated - carbohydrates don't readily attach to them - all other blood proteins are glyclocylated |
|
|
Globulins
|
large protein - plasma cells produce immunoglobulins (gamma globulins)
Immunoglobulins help attack viruses and bacteria; alpha and beta globulins transport iron, lipids, and fat-soluble vitamins |
|
|
Fibrinogen
|
Large protein
Plays essential role in blood clotting |
|
|
Formed Elements of Blood
|
White Blood Cells
Red Blood Cells Platelet |
|
|
Blood Smear
|
Cheap and fast way to see what might be going on in respect to the blood
Looking for how dense the blood cells are (not very dense - anemia) Lots of white blood cells when we are sick Also can see thrombocytes (platelets) |
|
|
Hematocrit
|
Percentage of red blood cells of total blood volume
Males: 40-54% - have higher hermatocrit Females 38-46% |
|
|
Anemia
|
Low hermatocrit - cannot supply tissues with oxygen that they need
Reduced oxygen carrying capacity of blood Iron-Deficiency Anemia - inadequate iron in diet Megaloblastic Anemia - inadequate vitamin B12 intake Pernicious Anemia (stomach no intrinsic factor) - parietal cells in your stomach are attacked by your immune system - will not secrete intrinsic factor which is necessary for the uptake of B12 Hemolytic Anemia - plasmalemma rupture Thalassemia - large contributing factor to anemia Aplastic Anemia (red bone marrow destruction - destruction of hermatopoeitic connective tissue |
|
|
Polycythemia
|
high increase in the percentage of RBC's - high hematocrit (above 54%)
Can be caused by dehydration or blood doping in athletes |
|
|
Erythropoietin (EPO)
|
Direct stimulus for the production of red blood cells is hypoxia (cellular oxygen deficiency) in kidney cells
Stimulates the synthesis of EPO in the kidneys EPO stimulates the production of RBC's Growth factor for erythrocytes Kidneys (peritubular interstitial cells - fibroblasts) Liver (perisinusoidal cells) during fetal development 10 mU/ml --> 10,000 mU/ml |
|
|
Blood Cell Formation
|
Hemopoiesis - process by which the formed elements of blood develop
First occurs before birth in the yolk sac of an embryo and later in the liver, spleen, thymus, and lymph nodes of a fetus. In the last three months before birth, red bone marrow becomes the primary site of hemopoiesis and continues to be the source of blood cells after birth and throughout life |
|
|
Red Bone Marrow
|
highly vascularized connective tissue located in the microscopic spaces between trabeculae of spongy bone tissue
about .05-.1% of red bone marrow cells are pluripotent stem cells - capable of developing into many different types of cells |
|
|
Pluripotent Stem Cells
|
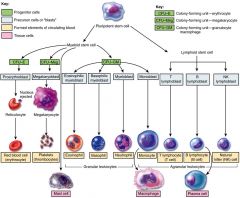
differentiate into myeloid stem cells and lymphoid stem cells
|
|
|
Myeloid Stem Cells
|
give rise to erythrocytes, thrombocytes, granular leukocytes (neutrophils, eosinophils, basophils), mast cells, and monocytes
Complete their development in red bone marrow |
|
|
Lymphoid Stem Cells
|
gives rise to agranular leukocytes (minus monocytes)
(T lymphocytes, B lymphocytes, natural killer cells) Begin to develop in red bone marrow but complete development in lymphatic tissues |
|
|
Myeloid and Lymphoid Cells and Hemopoiesis
|
Myeloid stem cells differentiate into progenitor cells - no longer able to reproduce themselves
CFU-E - produce erythrocytes (red blood cells) CFU-Meg - produce megakaryocytes (the source of platelets) CFU-GM - produce granulocytes (specifically neutrophils) and monocytes In the next generation, develop into precursor cells - over several cell divisions they develop into the actual formed elements of blood Lymphoid stem cells differentiate into T lymphoblast and B lymphoblasts which ultimately form T lymphocytes and B lymphocytes respectively |
|
|
Hemopoietic Growth Factors
|
Cytokines
Erythropoeitin (EPO) Thrombopoietin (TPO) Other Cytokines |
|
|
Cytokines
|
protein signaling molecules
Broad category of small peptide molecules - glyclocylated - means of communication among leukocytes and other cells of the body |
|
|
Thrombopoietin (TPO)
|
Secreted by the liver to produce more thrombocytes
|
|
|
Other Cytokines
|
Colony stimulating factors
Interleukins |
|
|
Bone Marrow Exam
|
in sampling for pathologies that might related to bone marrow (i.e. leukemia) - taken from the posterior iliac crest or the sternum
Relatively simple procedure but somewhat painful Low risk of side effects |
|
|
Red Blood Cells (Erythrocytes)
|
4.8 (females) - 5.4 (males) million RBC's/uL
Biconcave discs - more surface area Hemoglobin (33% of weight) - 280 million molecules per RBC - transports it Anucleate, lack mitochondria Life cycle average = 120 days Production = 2 million RBCs/second |
|
|
Hemoglobin
|
Reversibly binds to oxygen
At the center of each sub-unit is a heme groupwhich has an iron as its center where oxygen can reversibly bind to it |
|
|
Sickle Cell Disease (SCD)
|
Hb-S
Autosomal recessive - need to receive sickle cell allele from both parents Overdominance Malarial resistance May be compounded with a thalassemia (fewer RBC's produced and less hemoglobin) Predisposes hemoglobin molecules into forming polymers - quaternary structure changes and will form non-covalent polymer with hemoglobin molecules - RBC's take on a sickle-shape When they sickle they become adherent to one another and this causes them to lose their elasticity and get stuck in capillaries causing a lack of blood flow (eskemia) and can be deadly |
|
|
Hemoglobin
|
Globin protein - 4 polypeptides (2 alpha, 2 beta)
Heme - iron-containing pigment Reversibly binds to O2 - oxygen picked up in the lungs - as blood flows through tissue capillaries, the iron-oxygen reaction reverses and hemoglobin releases oxygen which diffuses into the cells Carrier 23% of CO2 - reversibly binds to carbon monoxide - competes and lowers the ability of hemoglobin to carry oxygen May release NO (nitric oxide) - vasodialation - helps to control blood flow |
|
|
Erythropoiesis
|
proerythroblast (red bone marrow) will divide and some of them will move from red bone marrow to blood system and will eject nuclei --> reticulocyte (ejected nucleus; in CVS) eventually matures --> mature erythrocyte
|
|
|
Blood Doping
|
Exogenous EPO
Transfusion (homologous or autologous) - inject exogenous EPO Natural blood doping - training at higher altitudes - body increases the production of red blood cells Polycythemia - abnormally high level of RBC's |
|
|
Blood Group Systems
|
RBC surface antigens - can be used to distinguish types of blood cells
100 genetically identified, 14 recognized systems Four basic blood types: Type A, B, AB, and O - named for surface feature antigens Type A - has A antigen and anti-B antibody in the plasma Type B - has B antigen and anti-A antibody in the plasma Type AB has both A and B antigens and neither antibody Type O has neither A or B antigens but has both anti-A and anti-B antigens in the plasma |
|
|
Hemolytic Disease of the Newborn (HDN) - Rh+
|
Arises during pregnancy
If a small amount of Rh+ blood leaks from the fetus through the placenta into the bloodstream of an Rh- mother, the mother will start to make anti-Rh antibodies - usually affects second pregnancy If the mother becomes pregnant again, her anti-Rh antibodies can cross the placenta and enter the bloodstream of the fetus If the fetus is Rh- no problem (Rh- blood does not have the Rh antigen) - If the fetus is Rh+ agglutination (clumping) and hemolysis (rupture) of REBC's brought on by fetal-maternal incompatibility may occur in the fetal blood Injection of anti-Rh antibodies (RhoGAM) can prevent HDN |
|
|
White Blood Cells (Leukocytes)
|
Granular vs. Agranular
Granules are clusters of proteins Agranular are usually lymphocytes themselves or phagocytic Monocytes fall under agranular but come from lymphoid stem cell***** Phagocytosis - ingest bacteria and dispose of dead matter Emigration (formly diapedesis) - able to cross capillary walls Chemotaxis Major histocompatibility complex (MHC) antigens |
|
|
Granular Leukocytes
|
Neutrophils
Eosinophils Basophils |
|
|
Neutrophils
|
no strong dye attraction - stain dull blue/pink
2-5+ lobed nuclei - older the cell, more nuclei Polymorphonuclear leukocytes - "polys" - lots of nuclei Most abundant, first on scene Phagocytic, chemotaxic, release cytokines Degranulation - release a lot of different substances like defensins and cytokines which disrupt cell membranes of various pathogens |
|
|
Eosinophils
|
Absorb eosin stain (acidic) - red-orange
2-3 lobed nuclei Granules do not obscure nuclei Phagocytic, chemotaxic Degranulation (enzymes) Numbers are greatest during parasitic infestation (allergies and endoparasites) |
|
|
Basophils
|
Absorb basic stain - blue-purple
2-lobed nuclei Granules obscure nuclei Least common Chemotaxic Allergies and ectoparasites Degranulation - generally releasing substances that are going to compliment the immune system (histamine, heparin, serotonin, etc.) |
|
|
Agranular Leukocytes
|
Lymphocytes
Monocytes |
|
|
Lymphocytes
|
Nuclei round or indented and stain dark
Cytoplasm stains blue T cells B cells --> plasma cells Natural killer cells (innate) Small vs. Large Lymphocytes LL: acute viral infections and immunodeficiency diseases |
|
|
Monocytes
|
U-shaped nuclei
Differentiate into macrophages (fixed of wandering) and dendritic cells Both are phagocytic and antigen-presenters (they will engulf a pathogen, break it down, and move pieces of that pathogen to their surface and head to the lymphatic system where they'll meet up with cytotoxic t-cells or b-cells and present pathogen to them and body will become resistant to that particular pathogen) |
|
|
Differential White Blood Count
|
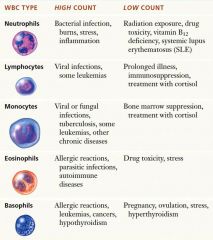
Leukocytosis - higher than typical level WBC present
Leukopenia - lower than expected level of WBC's |
|
|
Leukemia
|
bone marrow cancers with run-away abnormal leukocyte division
Acute lymphoblastic leukemia (ALL) - Most common leukemia in children Acute Myelogenous Leukemia (AML) -Both adults and children Chronic lymphoblastic Leukemia (CLL) - Most common in adults (esp. 55+) Chronic myelogenous leukemia (CML) - Mostly in adults Acute - generally runaway division of leukoblasts Chronic - generally runaway division of leukocytes Lymphoblastic - cells that are derived from lymphoid stem cells Myelogenous - cells that are derived from the myeloid stem cells |
|
|
Platelets (Thrombocytes)
|
Derived from myeloid stem cells
Megakaryocyte colony forming units --> megakaryoblasts --> megakaryocytes --> 2-3k thrombocytes Important for blood clotting Intrinsic and extrinsic cascades (clotting cascades) - prothrombin is converted into thrombin (which is an enzyme) which catalyzes two reactions: the first takes fibrinogen and converts it into fibrin (insoluble fibrinogen): it also catalyzes the formation of Factor 13A to Factor 13 - gets fibrin to clot - fibrin forms a dense web and thrombocytes get caught up in that web to form a blood clot |
|
|
Stem Cell Tranplants
|
Bone Marrow
Destruction and replacement with donor tissue Vulnerable to infection Graft-vs.-host disease Cord Blood Easily obtained Less infection and g-v-h issues Stored indefinitely |
|
|
Heart
|
pump driven by cardiac muscle tissue
Connective tissue about the size of closed fist Sits in the mediastinum - space between the sternum and the vertebral column and two lungs (also between 1st rib and diaphragm) Medial to pleurae Always working |
|
|
Heart Surfaces and Borders
|
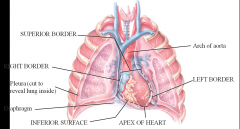
Heart is medial and posterior to the lungs- great vessels come superiorly off of the heart
inferior surface rests on the diaphragm Left border more extensive than right border Apex of the heart points anteroinferiorly (and slightly to the left) Anterior surfaces and posterior surfaces (against the vertebral column) |
|
|
Pericarium
|
Fibrous pericardium
Serous pericardium |
|
|
Fibrous Pericardium
|
Dense irregular connective tissue (inelastic)
protective, anchor most external layer |
|
|
Serous Pericardium
|
Parietal layer- fused to the fibrous pericardium
Pericardial cavity (percardial fluid - lubricant) Visceral layer (epicardium) - adherant to the heart |
|
|
Pericarditis
|
Acute
Typically suddenly and idiopathic (don't know what causes it) May mimic "heart attack" symptoms Treated with NSAIDs Chronic Gradual and long-lasting May lead to cardiac tamponade (when there is too much fluid in the serous layers) Treated with pericardiocentesis - use need and angle it upward and aspirate until we draw fluid |
|
|
Layers of the Heart
|
Visceral Pericardium (Epicardium) - lays over a little bit of adipose tissue and vasculature
Myocardium - comprised of cardiac muscle tissue Endocardium - deepest layer of the heart and is made up of mesothelium All of the cardiovascular system has simple squamous with basement membrane |
|
|
Epicardium
|
Two layers:
Visceral serous pericardium (mesothelial) Fibroelastic and adipose Neurovasculature for myocardium |
|
|
Myocardium
|
Cardiac muscle tissue - responsible for the pumping action of the heart
Myocarditis - inflammation of the myocardium that usually occurs as a complication of a bacterial or viral infection |
|
|
Endocardium
|
Endothelial
provides a smooth lining for the chambers of the heart and covers the valves of the heart Endocarditis - inflammation of the endocardium from bacteria - can affect valves of the heart and how it functions |
|
|
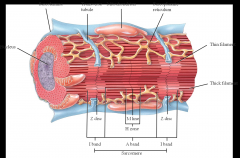
Cardiac Muscle Tissue
|

Striated - relies upon the overlap of motor proteins (actin and myosin) to work
Only has one nucleus per cell Intercalated Discs - this is where muscle cells connect to each other - embedded within the membrane are desmesomes (anchor adjacent cells together) and gap junctions (tubes that can continuously connect adjacent cells that share a cytoplasm) Adjacent cardiac muscle cells are able to work in concert because they share cytoplasm - as one cell is depolarized the cytoplasm allow all the other cells to contract as well |
|
|
Cardiac Muscle Cell
|
Can be autorhythmic - important to how the heart functions
|
|
|
Circulations of the Heart
|
Systemic Pump - comes from the left side of the heart - works through aorta - circulates oxygenated blood to all the systems of the body
Pulmonary Pump - comes from right side of the heart - fed by pulmonary artery - moves deoxygenated blood through the blood vessels of the lungs Coronary - provides myocardium with energy and nutrients it needs to make that energy - comes from right side of the heart |
|
|
Surface Features of the Heart
|
Auricles
Anterior Interventricular Sulcus Posterior Interventricular Sulcus Coronary Sulcus |
|
|
Auricles
|
expansions of the atria that allow blood to flow into it (hold a greater volume of blood)
|
|
|
Anterior Interventricular Sulcus
|
shallow groove on the anterior surface that marks the external boundary between the right and left ventricles
|
|
|
Posterior Interventricular Sulcus
|
marks the external boundary between the ventricles and the posterior aspect of the heart
|
|
|
Coronary Sulcus
|
goes around the heart - separates superior atria and inferior ventricles - coronary arteries are named for occupying the coronary sulcus
|
|
|
Structure of Heart
|
Atria
Atrioventricular Valves Ventricles Semilunar Valves |
|
|
Atria
|
gets deoxygenated blood from the vena cava (superior and inferior) and coronary sinus
walls of the atria are muscular but thin Pectinate Muscles - parallel ridges that line the remainder of the atrial wall |
|
|
Atrioventricular Valves
|
Tricuspid Valve
Bicuspid (mitral) Valve Chordae Tendineae - tendonlike cords - cusps of the tricuspid valve are connected by these |
|
|
Ventricles
|
Left ventricle is thicker than the right ventricle
Trabeculae Carneae - series of ridges formed by raised bundles of cardiac muscle fibers Papillary Muscles - chordae tendineae are connected to this - cone-shaped trabeculae carneae |
|
|
Right Atrium
|
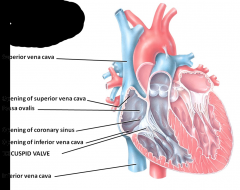
Superior and inferior vena cava and coronary sinus all dump here
Blood leaves the right atrium through the tricuspid valve and into the right ventricle |
|
|
Right Ventricle
|
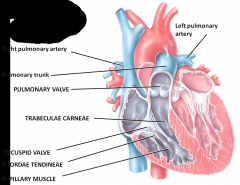
Right ventricle is separated from the left ventricle by a partition called the interventricular septum
Blood passes from the right ventricle through the pulmonary valve into the pulmonary trunk - divides into right and left pulmonary arteries |
|
|
Left Atrium
|
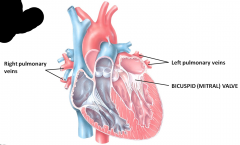
Pulmonary vein brings deoxygenated blood to left atrium moves through bicuspid valve which has a more robust myocardium (because it pumps blood to the entire body)
Blood passes through the bicuspid valve (left AV valve) |
|
|
Left Ventricle
|
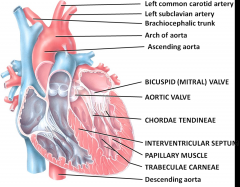
thickest part of the heart
forms the apex of the heart Blood passes from the left ventricle through the aortic valve into the ascending aorta - some of the blood in the aorta flows into the coronary arteries which branch from the ascending aorta and carry blood to the heart wall remainder of the blood passes into the arch of the aorta and descending aorta |
|
|
Flow of Blood
|
Right Atrium (deoxygenated blood) --> Tricuspid valve --> Right Ventricle --> Pulmonary Valve --> pulmonary trunk and pulmonary arteries --> in pulmonary capillaries, blood loses CO2 and gains O2 --> pulmonary veins (oxygenated blood) --> Left atrium --> Bicuspid valve --> Left ventricle --> Aortic valve --> Aorta and systemic arteries --> In systemic capillaries, blood loses O2 and gains CO2 --> Comes in through superior vena cava, inferior vena cava, and coronary sinus back to right atrium
|
|
|
Fibrous Skeleton of Heart
|
Heart valves located here
Anchor valves Prevents over-stretching Anchors cardiac muscle fibers Electrical insulation between the atria and ventricles - finer scale coordination of the contraction of the atria vs. the ventricles - without this level of insulation, being able to properly coordinate the rate of heart contraction would be very difficult |
|
|
Valve Coordination
|
Ventricular Diastole
Ventricular Systole |
|
|
Ventricular Diastole
|
ventricles fill with blood (relaxation) - global relaxation of the heart followed by systole
|
|
|
Ventricular Systole
|
blood sent to pulmonary and systemic loops
Ventricles contract and the semilunar valves open and the AV valves close |
|
|
Valve Disorders
|
Stenosis
Insufficiency Rheumatic Fever |
|
|
Stenosis
|
narrowing
problem when the aorta narrows - limits the amount of blood that can leave the heart and will increase the pressure of the blood as it leaves the heart |
|
|
Insufficiency
|
valves won't completely close - get back-flow of blood
Aortic Insufficiency - blood comes back into the left ventricle Mitral Insufficiency - blood is flowing from left ventricle into the left atrium Mitral Valve Prolapse - the valve just completely back-flows blood - this is when people need to get valvular replacement |
|
|
Rheumatic Fever
|
can lead to vegetative plaques on the valves and these nodules will keep the valves from closing
|
|
|
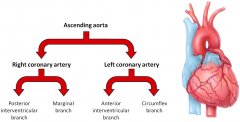
Coronary Circulation (Arteries)
|
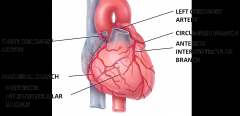
Ascending aorta --> Coronary Arteries
Left coronary Artery --> Anterior interventricular branch (services both ventricles) --> circumflex branch (left atrium and ventricle) Right Coronary Arteries --> Atrial branches (small; right atrium) --> Marginal branch (right ventricle) --> posterior interventricular branch (both ventricles) Coronary arteries are terminal arteries, they don't necessarily have anastomoses (connections with other arteries for collateral circulation - alternate routes) though they can do so - anastomoses very susceptible to atherosclerosis |
|
|
Coronary Circulation (Veins)
|
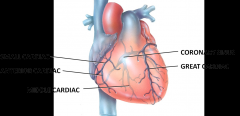
After blood passes through the arteries of coronary circulation, it passes into capillaries where it delivers oxygen and nutrients to the heart muscle and collects carbon dioxide and wastes - blood enters the veins
Left coronary artery --> ventricles and left atrium --> great cardiac vein --> posterior interventricular branch --> ventricles --> middle cardiac vein --> right atrium and ventricle --> small cardiac vein --> right ventricle --> anterior cardiac veins --> coronary sinus --> right atrium |
|
|
Great Cardiac Vein
|
wraps around and comes to the coronary sinus
drains all of the heart with the exception of aspects of the right atrium and ventricle - for that we have two separate vessels Drains the areas of the heart supplied by the left coronary artery (left and right ventricles and left atrium) |
|
|
Small Cardiac Vein
|
wraps around and goes into coronary sinus, draining the right atrium and right ventricle
|
|
|
Anterior Cardiac Vein
|
generally there are several (can be up to 5)
help to drain the right ventricle and they loop over the coronary artery and dump directly into the right atrium (independently) - can spot them because they go over the right coronary artery |
|
|
Myocardial Ischemia
|
reduced blood flow to the myocardium
Hypoxia - deficiency in the amount of O2 reaching the tissues Angina Pectoris - chest pain |
|
|
Mycardial Infarction (MI)
|
Death of an area of myocardium due to lack of blood flow
Heart attack Fibrosis --> weakened heart Ventricular Fibrillation |
|
|
Cardiac Conduction System
|
1. Sinoatrial (SA) Node - natural pacemaker - atria contract
2. Atrioventricular (AV) Node - time for atria to empty blood into ventricles 3. Atrioventricular (AV) Bundle [Bundle of His] - only site where action potentials can conduct from the atria to the ventricles (elsewhere, the fibrous skeleton of the heart electrically insulates the atria from the ventricles) 4. Right and Left Bundle Branches 5. Purkinje Fibers - ventricular contraction - moves upward from the apex, and blood is pushed toward the semilunar valves |
|
|
Cardiac Conduction System Part 2
|
SA node --> 90-100 action potentials/min (bpm)
Vagus nerve --> acetylcholine --> 75 bpm Electrocardiogram (ECG or EKG) composite of all 'electrical' activity (action potentials) generated by nodal and contractile cells Membrane potentials Resting membrane potential Depolarization vs. repolarization Depolarization: reduction in the membrane potential; the inside of the membrane becomes less negative than the resting membrane potential Repolarization: restoration of the resting membrane potential |
|
|
Normal EKG: A Single Heartbeat
|
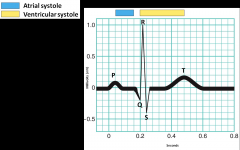
P Wave: SA node depolarization
QRS Complex: ventricular depolarization T Wave: ventricular repolarization |
|
|
Heart Rhythm
|
Normal sinus rhythm - usual rhythm of heartbeats, established by the SA node
Arrhythmia (dysrhythmia) - abnormal rhythm as a result of a defect in the conduction system of the heart Bradycardia < 50 bpm Tachycardia > 100 bpm |
|
|
Extrinsic Control of the Heart
|
Cardiac plexus - forms synaptic junctions with the nodal tissues and the coronary vessels - autonomic nervous system - two parts:
Cardiac branches of Vagus (X) nerve Cardiac branches of cervical and upper thoracic sympathetic trunk nn. (T1-4) Sympathetic Response: heart rate speeds and coronary arteries dilate Parasympathetic Response: heart rate slows and coronary arteries constrict |
|
|
Artificial Pacemakers
|
SA (100 bpm)
AV (40-60 bpm) AV bundle, etc. (20-35 bpm) Battery + impulse generator, connected to two leads |
|
|
Cardiac Cycle
|
Relaxation: all chambers in diastole
- Most of ventricular filling (75%) occurs Pressure of the atria versus pressure of the ventricles versus pressure of vasculature Atrial Systole - AV open, SL closed Ventricular Systole - AV closed, SL closed --> open |
|
|
Heart Sounds
|
S1 (lubb) - blood turbulence as AVs close
S2 (dupp) - blood turbulence as SLs close S3 - blood turbulence during ventricular filling S4 - blood turbulence during atrial systole |
|
|
Heart Murmur
|
abnormal sounds
- Clicking, gurgling, rushing - Typically benign in children - Valve disorder in adults |
|
|
Exercise and the Heart
|
Aerobic Exercise (3-5x weekly)
Cardiac output (stroke volume) Cooperation with respiratory system Angiogenesis - development of new blood vessels from pre-existing ones Physiological vs. Pathological Cardiomegaly - enlargement of the heart - Physiological - athletes get this - muscle enlarged from working out - Pathological - sickness - hypertrophy of heart |
|
|
Coronary Artery Disease (CAD)
|
Atherosclerotic plaque --> mycardial ischemia
Risk Factors: smoking, arterial hypertension, diabetes mellitus, obesity, hyperlipoproteinemia, age, being male, etc. Lipoproteins Low-density (LDLs): liver --> cells; "bad cholesterol" High-density (HDLs: cells --> liver; "good cholesterol" Inflammation Fatty streak = foam cells, macrophages, and T cells |
|
|
CAD Diagnosis
|
EKG
Stress test Radionuclide Imaging Echocardiography Electron Beam Computerized Tomography (EBCT) Coronary Computer Tomography Radiography (CCTA) Cardiac Catheterization Coronary Angiography |
|
|
CAD Treatment
|
Coronary artery bypass grafting (CABG) "cabbage" - blood vessel from another part of the body is attached to a coronary artery
Percutaneous transluminal coronary angioplasty (PTCA), and stenting |
|
|
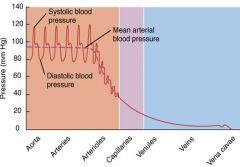
Blood Vessels
|
Arteries - away from the heart
Arterioles - resistant vessels Capillaries - permeable, exchange Venules Veins - towards the heart Angiogenesis - formation of new blood vasculature |
|
|
Angiogenesis and Disease
|
Tumor Angiogenesis Factors (TAFs) - secreted from tumors that stimulate blood vessel growth to provide nourishment for the tumor cells
Vascular Epithelial Growth Factor (VEGF) Basic Fibroblast Growth Factor (bFGF) Proliferative Diabetic Retinopathy - angiogenesis may be important in the development of blood vessels that actually cause blindness, so finding inhibitors of angiogenesis may also prevent the blindness associated with diabetes |
|
|
Blood Vessel Structure
|
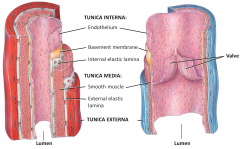
Tunica Interna (intima)
Tunica Media Tunica Externa Arteries have elastic lamina present while in veins they are absent Arteries have very well defined tunica media whereas veins do not Veins have valve flaps that allow one way flow of blood |
|
|
Tunica Interna
|
endothelium (thin layer of flattened cells) + basement membrane (provides a physical support base for epithelial layer)
internal elastic lamina - forms the boundary between the tunica interna and tunica media - facilitate diffusion of material through the tunica interna to the thicker tunica media |
|
|
Tunica Media
|
smooth muscle
Vasoconstriction vs. vasodialation external elastic lamina - forms the outer part of the tunica media and separates the tunica media from the outer tunica externa |
|
|
Tunica Externa
|
Elastic and collagenous fibers
Contains lots of nerves Vasa vasorum - small vessels that supply blood to the tissues of the vessel Helps anchor the vessels to surrounding tissues |
|
|
Transverse Section of Artery
|

|
|
|
Arteries (Efferent)
|
Elastic (conducting) Arteries
Muscular (distributing) Arteries Anastomoses |
|
|
Elastic (Conducting) Arteries
|
Largest (ex. aorta, pulmonary trunk)
Walls about 10% of vessel diameter Well-defined elastic laminae Thick tunica media (elastic lamellae) Function as pressure reservoirs - as blood pumps into them they expand and then they snap putting more force on the blood to move forward Feed into muscular arteries |
|
|
Muscular (Distributing) Arteries
|
Thick, muscular tunica media (3 --> 40+ layers) - can really regulate the blood by vasodilation or vasoconstriction
Walls about 25% vessel diameter Vascular tone - the greater the tone the greater the resistance on the blood Ex. right and left arteries |
|
|
Arterioles
|
Resistance vessels (autonomic control = sympathetic)
Thin tunica interna and thin internal elastic laminae Walls about 50% of vessel diameter Feed into capillary beds Microcirculation Metarteriole (terminal end of the arteriole) --> thoroughfare channel --> Pre-capillary sphincters (allows or restricts blood into capillary bed) --> capillaries --> venule |
|
|
Capillaries
|
Exchange vessels (blood <--> interstitial fluid)
Lack tunica media and tunica externa Diameter about 5-10 um Distribution dependent upon metabolic need |
|
|
Capillary Types
|
Continuous
Fenestrated Sinusoid |
|
|
Continuous Capillary
|
CNS, skin, lungs, skeletal, and smooth muscle, and connective tissues
|
|
|
Fenestrated Capillary
|
kidneys, small intestinal villi, choroid, plexuses, ciliary processes (eyes), most endocrine glands
Has spaces |
|
|
Sinusoid Capillary
|
Liver, red bone marrow, spleen, adenohypophysis, parathyroid and adrenal glands
Areas where exchange in capillary beds is frequent and very important where these capillaries are |
|
|
Venules --> Veins
|
Afferent
Postcapillary venules --> muscular venules --> veins Thin tunica media and tunica interna Thick tunica externa Walls about 10% of diameter Low blood pressure --> Valvular Muscle milking - when you place a major vein between or next to skeletal muscles - as these muscles contract and relax they do the same to the veins Respiratory milking |
|
|
Venous Valves
|
thin folds of tunica interna that form flap-like cusps
low blood pressure in veins allows the flow of blood returning to the heart to slow and even back up; aid in venous return by preventing backflow |
|
|
Varices
Singular - Varix |

These valves can sometimes fail and when they fail blood can back up (pool) in veins and they can be stretched
Varicose veins - treatable Not muscularized and gravity as it pulls blood back down it closes the valve (in a normal vein) - if this doesn't happen it causes varices |
|
|
Venous Thromboembolism (VTE)
|
Deep vein thrombosis (DVT) followed by pulmonary embolism (PE) - makes itself up through the limbs and goes up the lungs and occludes blood flow there
Vena Comatins - if you bundle vein with artery then the action of the pulsing artery will help move blood forward |
|
|
Blood Pressure
|
Diminished blood pressure which is why you need to push it up as you get to the venules and veins
|
|
|
Portal Systems
|
Portal vessels (veins) connecting capillary beds
Hepatic - blood is being taken to the liver Hypophyseal - blood is being taken to the neurohypothesis of the pituitary gland from the hypothalamus Renal - blood is being moved around the nephron (humans do not have this) |
|
|
Blood Distribution
|
At rest:
64% systemic veins and venules 13% systemic arteries 7% systemic capillaries 9% pulmonary vasculature 7% heart Systemic veins as blood reservoirs Venoconstriction- forces blood back to the arteries |
|
|
Circulatory Routes
|
Systemic
Coronary Cerebral Hepatic portal Nutrient arteries to lungs Pulmonary Fetal |
|
|
Aorta Circulation
|
Ascending aorta (aortic valve)
Aortic arch - descends and ends at C4-C5 Thoracic Aorta - passes through diaphragm to become.. Abdominal Aorta - divides into common iliac arteries |
|
|
Ascending Aorta Branches
|
Right and left coronary arteries
Arch gives rise to all vasculature that serves the upper limbs and neck |
|
|
Aortic Arch Branches
|
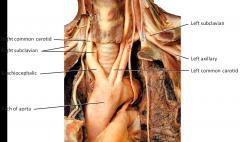
Three major branches:
Brachiocephalic Trunk- right common carotid artery and right subclavian artery Left Common Carotid Artery Left Subclavian Artery Subclavian supply the upper limbs Common Carotid largely supplies head and neck |
|
|
Common Carotid Artery Branches
|
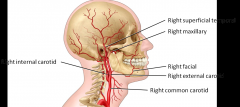
Carotid sinus - where you feel your pulse - divide into external and internal carotid arteries
Internal carotid arteries go inside your skull and branch (largely for your branch) and external carotid arteries will branch outside of your skull and supply your head and face and superficial skull |
|
|
Subclavian Artery Branches
|
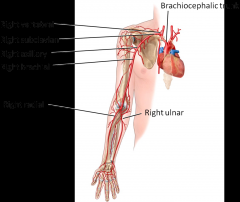
Subclavian turns into:
Axillary --> Bracial --> Radial and Ulnar Arteries |
|
|
Thoracic Aorta Branches
|

Two branches:
Visceral: Pericardial, Bronchial, Esophageal, Mediastinal branches Parietal: Posterior Intercostal, Subcostal, Superior phrenic |
|
|
Abdominal Aorta Branches
|
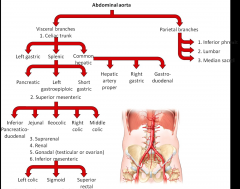
After we cross the diaphragm we are now in the abdominal aorta
Pay most attention to what is numbered as visceral branches Major branch: celiac trunk Major branch: superior mesenteric - picks up where the celiac left off - remainder of duodenum, all of small intestines, and the first 2/3's of the large intestine - division where the superior mesenteric stops and inferior mesenteric picks up is part of the colon (sphrenic flexor) Major branch: from the sphrenic flexur through the sigmoid colon through the rectum is supplied by the inferior mesenteric Series of arteries between superior and inferior mesenteric - suprarenal (sit on top of kidneys) kidneys are fed by renal arteries directly and the gonadal arteries will services the gonads Pancreas serviced by celiac and inferior mesenteric - inferior mesenteric from below and celiac provides vasculature to superior portion |
|
|
Abdominal Aorta Branches and Legs
|
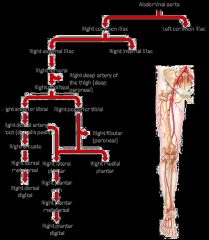
Splits to common iliac arteries (right and left)
Splits again into external and internal iliac arteries External artery also known as femoral artery which will eventual turn in popliteal artery and then tibial (posterior and anterior) and fibular artery Common iliac aa --> external iliac aa. --> femoral aa. ****** |
|
|
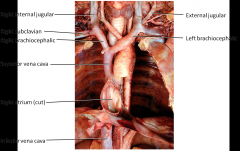
Major Systemic Veins
|
Superior Vena Cava: head, neck, thorax, and upper extremities
Inferior Vena Cava: abdomen, pelvis, and lower extremities Coronary Sinus: heart Brachiocephalic Veins: supplied by a subclavian vein and an internal jugular All major veins drain in to the right atrium |
|
|
Thoracic Veins
|
|
|
|
Venipuncture
|
Cubital vein - crosses the cubital fossa - connected the cephalic and basilic vein - major veins of the upper limb are superficial veins - first place to go for blood draw
In the lower limbs, the major veins are deep whereas the minor veins are superficial*** |
|
|
Great Saphenous Vein
|
Starts at the medial miolis - dumps into the femoral vein
Clinically important for two reasons: 1. If doctors need a graft they will go to great saphenous vein (it is superficial and large) [CABG] 2. important region for doing saphenous vein cut down - when a surgeon visualizes a superficial vein and opens the skin around it so you have direct access to the vasculature - if you have to put in a line and rehydrate immediately want to do this here |
|
|
Hepatic Portal Circulation
|
delivers blood to the liver
Superior mesenteric and splenic veins unite to form this - after passing through the liver, blood drains into the hepatic veins, which then empty into the inferior vena cava Includes, celiac, superior mesenteric and inferior mesenteric At the same time the liver is receiving nutrient-rich but deoxygenated blood via the hepatic portal vein, it also is receiving oxygenated blood through the hepatic artery, a branch of the celiac trunk |
|
|
Pulmonary Circulation
|
Carries deoxygenated blood from the right ventricle to the air sacs within the lungs and returns oxygenated blood to the left atrium
Pulmonary trunk from the right ventricle --> divides into right and left pulmonary artery (only arteries that carry deoxygenated blood) --> air exchange in capillaries --> pulmonary veins which exit the lungs and carry oxygenated blood to the left atrium (two left and two right pulmonary veins enter the left atrium) |
|
|
Fetal Circulation
|
Umbilical arteries (2): fetus --> placenta
Umbilical Vein: placenta --> fetus Ductus venosus: umbilical vein --> inferior vena cava - Birth --> ligamentum venosum (ductus venosus) - Birth --> ligamentum teres heparis (umbilical vein) Ductus arteriosus: pulmonary trunk --> aorta - Birth --> ligamentum arteriosum Foramen Ovale: blood passes through right atrium --> left atrium - Birth --> fossa ovalis |
|
|
Blood Vessel Development
|
Mesoderm --> mesenchyme --> hemangioblasts (both blood vessels and blood cells develop from this)
Angioblasts (form blood vessels)--> blood islands Space coalesce to form lumen |
|
|
Hypertension
|
Primary - persistent, idiopathic
Secondary - identifiable cause Lifestyle decisions: - Weight, exercise, alcohol consumption, salt consumption, smoking, stress |
|
|
Lymphatic System
|
lymph, lymph vessels, lymphatic organs, and red bone marrow
Reticular connective tissue + lymphocytes Functions: - Drains excess interstitial tissue - Transports lipids and lipid soluble vitamins (A, D, E, and K) - Immune responses |
|
|
Lymphocytes
|
B cells --> plasma cells (produce antibodies) --> memory B cells (can mount an even stronger immune response if the same antigen attacks the body)
T cells: - T-helper cells - work with B cells to amplify antibody production by plasma cells - T cytotoxic cells (destroy target cells) --> T memory cells ("remember" an antigen and mount a more vigorous response if the same antigen attacks the body) - T regulatory cells - can turn off immune response by supressing T cells - important for autoimmune diseases |
|
|
Lymph Circulation
|
Lymphatic capillaries -->
- Very permeable - Unidirectional flow - Lacteal and chyle (small intestine) Lymph vessels --> - Lymph nodes - Skin: follow veins - Viscera: follow arteries Lymph trunks - Lumbar trunks: lower limbs, pelvis, kidneys, etc. - Intestinal trunks: stomach, intestines, liver, pancreas, and spleen - Bronchomediastinal trunks: thorax, lungs, and heart - Subclavian trunks: upper limbs - Jugular trunks: head and neck Thoracic (left lymphatic) Duct and Right Lymphatic Duct - Cisterna chyle (receives lymph from the right and left lumbar trunks and from the intestinal trunk) --> Thoracic duct (main duct for return of lymph to blood) |
|
|
Edema
|
Swelling
Filtration >> Reabsorption - water retention about 30% threshold |
|
|
Lymph Flow
|
Aided by "pumps"
- Skeletal Muscle - aided by skeletal muscle contracting and relaxing - Respiratory - arteries pulsing will help move fluid Deeper lymphatic muscles have closer connections with arteries because the pulsing will help move lymphatic fluid through the system |
|
|
Lymphatic Organs and Tissues
|
Primary lymphatic organs
Secondary lymphatic organes and tissues |
|
|
Primary Lymphatic Organs
|
sites where stem cells divide and become immunocompetent (lymphocytes get exposure to antigen and are becoming active for that specific antigen)
- Thymus - Red bone marrow |
|
|
Secondary Lymphatic Organs and Tissues
|
sites where most immune responses occur
- Thymus - Lymph nodes and nodules (difference is a capsule - node has a capsule nodule does not) - Spleen - has a capsule |
|
|
Thymus
|
bilobed, capsulated (each lobe capsulated)
located in the mediastinum Cortex: T cell selection and maturation - t-cells are being activated against specific antigens but also learning to recognize self from non-self - 2% survive - because of the difficulty recognizing non-self - go to the medulla Medulla: - Thymic corpuscles - serve as sites of T cell death in the medulla Atrophies with age - after puberty thymus gland is shrinking |
|
|
Lymph Nodes
|
Bean-shaped and typically clustered
Capsule and compartments - capsulated Outer Cortex - Lymphatic nodules - full of B cells Inner Cortex - T cells and dendritic cells Medulla - B cells, plasma cells and macrophages Afferent vessels --> sinus --> efferent vessels (hilus) |
|
|
Inguinal Lymph Node
|
By femoral artery and vein
Drain the lymphatic vessels of the lower limbs |
|
|
Metastasis
|
Spread of a disease (or tumor)
typically via vasculature Follow lymph vessels "Firm and fixed" - become anchored to a location and are very firm - Lymphaginous - moves through lymphatic system - Hematoginous - moves through the circulation - Atagenic - messed up by doctor |
|
|
Spleen
|
Left hypochondriac region - right under the diaphragm - superior to left kidney and splenic flexor
Largest single mass of lymphatic tissue - encapsulated organ Serves a dual function - two types of pulp - white and red - White pulp: lymphocyte action - Red pulp: macrophages digesting old RBC's, platelet storage, hemopoiesis (in fetus) Blood enters through splenic artery |
|
|
Lymphatic Nodules
|
Acapsular
AKA mucosa associated lymphatic tissue (MALT) - Tonsils - five tonsils (two paired, one unpaired) - Pharyngeal (adenoid) - anterior posterior aspect of nasal pharynx - not paired - Palatine - tonsilar fossa - Lingual - base of tongue - Lamina propria (connective tissues) of mucous membranes - Aggregated lymphatic follicles (Peyer's patches) - located in the ileum of the small intestine |
|
|
Tonsillitis
|
Typically viral, but can also be group A streptococcal infection
Time, antibiotics Tonsillectomy Sometimes tonsil tissue will re-grow |
|
|
Signs of Infection
|
Lymphadenopathy - enlarged, tender
- Generalized or localized Lymphadenitis - skin over the lymph node becomes inflamed as a result of lymphadenopathy Bad when lymph node becomes large and becomes fixed and it's not painful |
|
|
Respiratory System
|
Coordinates with cardiovascular system
O2 in for chemoiosmosis CO2 waste expelled CO2 = volatile acid Nasal and oral cavities <--> pharynx <--> larynx <--> trachea <--> bronchi ,--> alveoli Can adjust the pH of our blood by adjusting our breathing |
|
|
Anatomy of Respiratory System
|
Upper: nose --> pharynx
Lower: larynx --> lungs Conducting Zone: filter, warm, and moisten air and conduct it into the lungs Respiratory Zone: main sites of gas exchange between air and blood |
|
|
External Nose
|
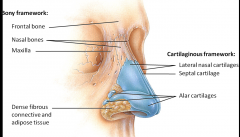
Primary route of inhalation
External Nares - openings into the external nose (nostrils) External nares --> nasal vestibule --> internal nares |
|
|
Internal Nose and Nasopharynx
|
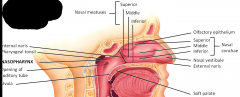
Respiratory vs. olfactory epithelium
Warms, filters, moistens incoming air Lining the lateral walls are the conchae - own independent bones - middle and superior conchae are elaborations of the ethmoid bone Olfaction Modifications of speech vibrations Nasopharynx - division of pharynx Opening of the auditory tube - goes to the middle ear As we cross the plane, move to the oropharynx |
|
|
Nasal Conchae
|
Superior
Middle Inferior |
|
|
Oropharynx and Laryngopharynx
|
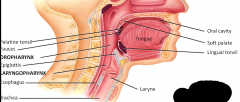
Shared space for consumption and respiration
Gloosopharyngeal (IX) and Vagus (X) nerve Hypopharynx (at the hyoid) Epiglottis - part of the laryngopharynx |
|
|
Coryza, Influenza, Etc.
|
Coryza - common cold symptoms
- Viral - Sneezing, rhinorrhea, cough, and congestion Seasonal Influenza - Fever, chills, muscle aches - Seasonal flu vaccine modified to what epidemiologists thinks will be bad H1N1 Influenza - Deadly |
|
|
Larynz
|
Connects the laryngopharynx to the trachea
"Voice box" C4-C6 9 Cartilages: 3 paired, 3 unpaired - Epiglottis - Thyroid (Adam's Apple) - Cricoid - Arytenoid (2) - Corniculate (2) - Cuneiform (2) |
|
|
Important Features of Larynx
|
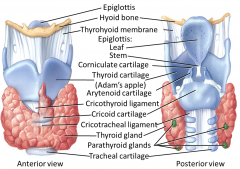
Thyroid cartilage - largest and most robust
Epiglottis - one cartilage that rises above at rest - attached to anterior rim of the thyroid cartilage Cricoid Cartilage - forms complete cartilogenous ring around the larynx - base upon which the corniculate will sit*** Trachea - has a series of hyaline cartilage rings that are incomplete Arytenoid Cartilage - attack to the vocal folds (true vocal cords) - creat sound Ventricular folds - false vocal cords - first things you can see Rima Glottidis - space between the vocal cords - space through which you are breathing Vocal chords are typically abducted |
|
|
Laryngitis and Laryngeal Cancer
|
Laryngitis - inflammation of the larynx
- Respiratory infection - Irritants Laryngeal Cancer - Cigarette smoking - when you smoke, increase risk of cancer 10x - when you drink, increase risk of cancer by 4x - smoke and drink increase risk of cancer by 40x - multiplicative effects - Radiation therapy and/or surgery |
|
|
Voice Production
|
vocal folds vibrate --> voice production
- Controlled by ten intrinsic laryngeal muscles - More tension = higher pitch - Greater air pressure = louder sound Nearly closed vocal folds --> whisper (vocal cords are adducted) Valsalva maneuver and the ventricular folds - Do it when you defecate - adduct your vocal chords and putting pressure on your abdominal pelvic cavity - helps you go to the bathroom |
|
|
Vocal Folds Abduction
|
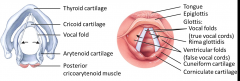
Can pivot - swing medially or laterally
When they swing laterally, they abduct - rima glottidis gets bigger Posterior cricoarytenoid muscle - pivots so they can swing around and abduct - necessary for breathing and producing voice Lateral cricoarytenoid muscle - adduct vocal chords (pulls them together) |
|
|
Trachea
|
tubular connection from larynx --> bronchi
About 12 cm length and 2.5 cm diameter Layered: - Mucosa - pdeudostratified ciliated columnar ET - Submucosa - areolar CT and seromucous glands - Media - C-shaped hyaline cartilage rings - most prominent feature - plus fibromuscular membrane (embedded trachealis muscle) - smooth muscle - contract when you forcefully exhale something - brings end of the C close together and constricts the trachea - Adventitia - areolar CT |
|
|
Tracheotomy and Intubation
|
Tracheotomy/Tracheostomy - longitudinal incision inferior to the cricoid cartilage
Cricothyrotomy - incision between thyroid and cricoid cartilage (emergency airway only) Intubation - tube passed through nose or mouth through the larynx in to trachea |
|
|
Bronchial Tree
|
Trachea --> Primary bronchi (right and left) --> Secondary (lobar) bronchi (right =3, left = 2) --> tertiary (segmental bronchi) --> bronchioles --> terminal bronchioles
- Terminus of the conducting zone - Clara cells (= club cells) - Protective, produce surfactant, reserve (stem) cells |
|
|
Bronchial Tree - Important Features
|
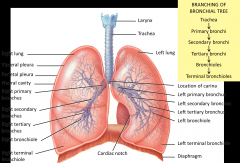
End of trachea - splits into two primary bronchi (serve right and left lungs respectively)
Ridge called the carina - separates air as it moves in - very vascularized - if something hits it you will into spasmatic coughing Right side is more robust than the left From the primary bronchi separate into secondary bronchi where you can branch into different lobes of the lung - secondary bronchi divide into tertiary bronchi Tertiary bronchi serve as bronchopulmonary segment - serviced by tertiary bronchis and has it's own blood supply - it is surgically receptible without compromising the rest of the lung*** Broncioles --> Terminal bronchioles --> respiratory bronchioles |
|
|
Bronchial Histology and Physiology
|
Trends as the branching in the bronchial tree becomes more extensive:
- Reduction of cilia and goblet cells - Reduction in cartilages - Increase in smooth muscle Sympathetic --> epinephrine and norepinephrine release --> airway dilation Bronchial arteries and veins (NB pulmonary veins) - Bronchial arteries will branch off of descending aorta - what is odd is that returning of the blood to the heart - very little of blood returns via bronchial veins - some people's don't have any at all - about 90% of the blood gets dumped into the pulmonary veins - odd because its deoxygenated blood headed back to the left atrium which will mix with highly oxygenated blood - strange**** |
|
|
Asthma
|
Spasm of the bronchiolar smooth muscle
- Bronchoconstriction - Allergens, anxiety, irritants Steroids that help alleviate some of the issues in respect to allergens and irritants and bronchodilators that help with symptoms |
|
|
Chronic Bronchitis
|
Excessive bronchial mucous secretion and cough
Excessive amount of mucous produced - makes it difficult to move air in and out of the lungs and may go to the lungs which is very irritating Mucous elevator impairment |
|
|
Lungs
|
Pleural membrane
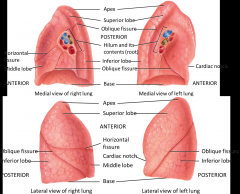
- Parietal Pleura - lines thoracic - on the body wall - Visceral Pleura - directly adherent to the lung - covers lung - Pleural cavity - space between the parietal and visceral pleura Fissures - separate lobes of the lung - Separating the middle lobe from the superior lobe is the horizontal fissure - separating the inferior from everything else is the oblique fissure Hilum - roots of the lung - includes pulmonary arteries, pulmonary veins, and depending on where you make this cut (if it's right at the lungs you'll have a right and left primary bronchi) Impression on the lung - room for the spinal cord and trachea and aortic arch - most conspicuous space is for the heart Cardiac Notch - for the heart - asymmetry in the lungs because of the position of the heart - the lungs are domed to accommodate the diaphragm |
|
|
Bronchopulmonary Segments
|

has it's own unique segmental bronchi and vasculature meaning they are independent units of each other
An individual bronchial segment can be removed individually without affecting the other bronchial segments **Learn two things from this: if you aspirate something 9/10, it will go to the right - if something is small enough to get into a bronchopulmonary segment it will usually end up in the superior segment of the inferior lobe - fluid will drain into the superior segment of the inferior lobe as well if someone is sitting in bed for a long time with some sort of lung infection |
|
|
Lobules of Lung
|
Encapsulate within a bronchopulmonary segment a respiratory region of the respiratory zone
Terminal Bronchiole - part of the conducting zone and branches into respiratory bronchioles which have alveolar ducts that lead to alveolar sacs which are surrounded by capillary beds which connect pulmonary arteries and veins - purpose it to maximize surface area so you can have a larger respiratory surface to exchange gas Terminal bronchioles --> respiratory bronchioles (start of respiratory zone) --> alveolar ducts --> alveolar sacs --> alveoli |
|
|
Smoking and the Respiratory System
|
Nicotine restricts terminal bronchioles
CO binds to hemoglobin - causes hypoxia Increased bronchial mucous production (by goblet cells) and mucosal edema Converts respiratory epithelium to squamous epithelium Destroys elastic fibers of lungs An individual can completely lose their mucous elevator Ultimately will have COPD - starts with emphysema |
|
|
Alveoli
|
Two types of cells that comprise the walls:
- Type I Alveolar Cells - diffusion membrane for gases - Type II Alveolar Cells - septal cells - secrete alveolar fluid to help lower the surface tension Alveolar macrophage - keeps an accumulation of foreign cells in lung by phagocytizing the material |
|
|
Respiratory Membrane
|
.5 um thick
Layered (epi-/endothelial sandwich) - Alveolar wall (type I and type II alveolar cells) - Epithelial basement membrane - Capillary basement membrane - Endothelium of capillary 70m2 = size of a handball court |
|
|
Emphysema
|
Alveolar wall destruction
Loss of surface area for respiration Destruction of elastic capacity of lungs --> COPD Lowered blood O2 saturation May be a precursor to lung cancer Barrel chested Mucous elevator is gone and are potentially suffering chronic bronchitis |
|
|
Lung Cancer
|
Leading cause of cancer deaths in the U.S.
85% smoking related (risk factor 10-30x greater) Bronchiogenic carcinoma - Adenocarcinoma: glandular ET (most common) - Squamous cell carcinoma: larger bronchial tube ET - Small Cell Carcinoma: primary bronchi ET |
|
|
Respiration
|
Pulmonary Ventilation: atmosphere <--> lungs
External (Pulmonary) Respiration: lungs <--> blood Internal (Tissue) Respiration: blood <--> interstitial fluid and cells Cellular Respiration: manufacturing ATP |
|
|
Pulmonary Ventilation (breathing)
|
Pressure - driven (1 atm = 760 mmHg)
Boyle's Law: PV = k Inhalation: P thoracic cavity < P atmosphere Exhalation: P thoracic cavity > P atmosphere Primary Muscles: diaphragm and intercostal muscles Accessory Muscles: abdominals, SCM, and scalene muscles Alter pressure by altering the volume |
|
|
Muscular Control of breathing
|
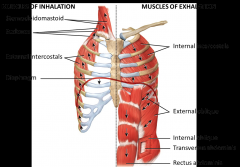
Diaphragm - most important for respiration - sets the boundary between the abdominal and thoracic cavity - moves inferiorly which increases the volume of the thoracic cavity therefore decreasing pressure
Generally tidal volume during quiet breathing is 500 mL Accessory muscles for inhalation (increase the volume of the diaphragm) - sternocleidomastoid and posterior, middle, and anterior scalenes (attach to ribs and yank them upwards) - external intercostal grab the ribs and pull them up and out Muscles of exhalation - internal intercostals pull ribs inwards and down - abdominals are also important for exhalation because they have to do with the abdominopelvic cavity, force increases pressure and displaces diaphragm which decreases volume and pushes air out of the lungs |
|
|
Respiratory Center of the Brain
|
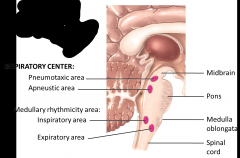
Medullary Rhythmicity Center
Apneustic Area Pneumotaxic Area |
|
|
Medullary Rhythmicity Center
|
Inspiratory area (2-3 sec): diaphragm (phrenic nn.) and external intercostal muscles (intercostal nn.) - when it is not stimulated the diaphragm relaxes
expiratory area: activates only during forceful breathing: internal intercostal muscles and abdominal muscles |
|
|
Apneustic Area
|
stimulates the inspiratory area
Prolongs inhalation Generally will slow respiration Mnemonic: ASIA - apneustic stimulates the inspiratory area |
|
|
Pneumotaxic Area
|
Inhibits the inspiratory area and shortens inhalation
Overrides the apneustic area |
|
|
Regulation of Respiratory Center
|
Cerebral Cortex (cortical)
- voluntary changes - Limited by [CO2] and [H+] Hypothalamus and Limbic - Emotional breathing (crying, laughing, etc.) Chemoreceptors - Central chemoreceptors (medulla): changes in CSF [CO2] and [H+] - Peripheral Chemoreceptors: aortic and carotid bodies - changes in blood [O2], [CO2], [H+] Bear Receptors - respond to being stretched Can alter your levels of cardiac rate by massaging carotid sinus - shouldn't do this - activates the bear receptors and glossopharyngeal will slow down the heart rate because the bear receptors will say that the pressure is high |
|
|
Inflation (Hering-Breuer) Reflex
|
Mediated by baroreceptors in bronchi/bronchioles
- Stretched (over-inflation) --> Vagus (X) stimulation --> inhibition of inspiratory and apneustic areas Likely a protective mechanism |
|
|
Exercise and Respiration
|
Pulmonary perfusion tied to cardiac output
Increases rate of oxygen diffusion Changes in depth of respiration (moderate) Changes in rate of respiration (strenuous) |
|
|
Pneumonia
|
Acute infection of alveoli
Immune responses --> ventilation impairment Commonly steptococcus pneumoniae |
|
|
Development of Respiratory System
|
4 weeks: respiratory diverticulum (outgrowth of foregut) aka lung bud
- Endoderm --> epithelium and glands - Splanchnic mesoderm --> CT and smooth muscles Proximal RD --> tracheal bud --> bronchial buds Weeks 6-16: all conductive elements form Weeks 16-26: most respiratory elements form Weeks 26+: maturation |
|
|
Respiratory Distress Syndrome
|
Infants born 26-28 weeks severely at risk
Alveoli collapse during exhalation Forced ventilation Surfactant (lowers surface tension) - don't have enough of it |
|
|
Aging and the Respiratory System
|
Loss of elasticity
Decrease in dust cell activity Decrease in ciliary action More prone to pulmonary infections |
|
|
Urinary Trivia
|
Kidneys receive about 25% of cardiac output at rest
Number of nephrons set at birth Kidney dysfunction may only be detectable at 25% of normal function Renalectomy may cause hypertrophy of remaining kidney - May increase to 80% function of both kidneys |
|
|
Anatomy of Urinary System
|
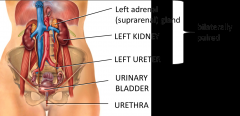
Bilaterally paired kidneys - right sits a little lower than the left (liver causes this by depressing the kidney down)
Attached to the kidney at the hila are vasculature Ureter - transport urine from the kidneys to the urinary bladder Suprarenal gland (sympathetic) - located superior to the kidneys |
|
|
Renal Functions
|
Maintenance of extracellular volume and osmolarity
- [ions] Na+, K+, Ca2+, Cl-, and HPO4 2- - pH: secretes H+, conserves HCO3- - volume: H2O - [glucose] glutamine --> gluconeogenesis or excrete Endocrine: excrete 3 major hormones - calcitriol: increase Ca2+ (PCT) - Erythropoietin: erthrocyte production (peritub.) - Renin: increase BP (juxtaglomerular apparatus) Excretion: catabolic wastes, bioactive substances - excrete glucose if you have diabetes |
|
|
Renin, Kidneys, and Liver
|
Kidney --> Renin
Liver: Angioteninsogen (when it has renin) --> turns into angiotensin I (with ACE you'll get) --> Angiotensin II which acts on the suprarenals to produce aldosterone Lungs: ACE --> leads to production of angiotensin II ACE Inhibitor: used for hypertension - blocks pathway so you don't get as much angiotensin II or aldosterone - look out for large drops in blood pressure |
|
|
Retroperitoneal
|
Sprarenal glands
Aorta and IVC Deodenum (proximal segment) Pancreas (tail) Ureters Colon (ascending and descending) Kidneys Esophagus (thoracic) Rectum (prox. 2/3) Secondarily RP: Duodenum, pancreas, colon |
|
|
Peritenium
|
Kidneys are behind the peritenium
Certain organs are retroperitenium - duodenum, ureter, kidney, bladder Simple squamous epithelium with basement membrane - need to peel away to get to the kidney |
|
|
Renal Fascia
|
Connective tissue that surrounds the kidney
|
|
|
Perirenal Fat
|
can be all around the neurovasculature
Fat and fascia important for anchoring the kidneys in place so they don't move too much Kidneys move a little bit with respiration as the diaphragm displaces, they go down and then will go back up |
|
|
Renal Cortex and Renal Medulla
|
Medulla is organized into renal pyramids
Cortex is all of the tissue that surrounds the medulla Renal Column - much of the nephron is embedded in the cortex and the Loop of Henle goes into the medulla - extend between renal pyramids Papilla - where the urine drops into the calyces - once urine makes it to the renal papilla cannot be reabsorbed Papilla --> Minor Calyces --> Major Calyces --> Renal pelvis --> Ureter --> Urinary bladder |
|
|
Nephroptosis
|
"Floating kidney"
Weakened fibrous attachments or sudden loss of adipose CT --> hydronephrosis (death of nephron) Nephroplexy for some symptomatic cases Great risk because the ureters can kind and urine can't flow through so pressure builds up and the kidney can expand due to that pressure which can lead to damage to the kidney |
|
|
Renal Circulation
|
Receive 20-25% cardiac output at rest
- About 1,800 L/day - 10% of that --> filtrate - 1% of filtrate (enters the nephron and has the ability to exchange material) --> urine Anterior and posterior branches Segmental aa --> Renal segments - Surgically resectable |
|
|
Right Renal Vein << Left Renal Vein
Right Renal Artery >> Left Renal Artery |
Right kidney has shorter renal vein than left kidney
Superior mesenteric artery can put pressure on the renal vein and can even occlude blood flow - called nutcracker syndrome - compromises the tissue of the testis and ovaries as well Right kidney artery is longer than left kidney artery |
|
|
Renal Segments
|
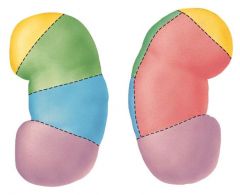
Superior and inferior segment and in-between these segments have anterior superior and anterior inferior and a posterior segment (posterior in the back of anterior superior and anterior inferior)
Each part is surgically receptible - can remove one without harming the other segments |
|
|
Kidney Arteries
|
Segmental arteries --> Interlobar arteries --> Arcuate arteries --> Interlobular arteries --> Afferent arterioles
Segmental arteries flow into interlobar arteries which are nestled between the renal pyramids and columns - as they cross around the base of the pyramids they turn into arcuate arteries --> from there they turn into interlobular arteries (really small) then afferent arterioles (go into the capillaries of the glomerulus) |
|
|
Blood Flow through Kidney
|

Renal Artery --> Segmental Arteries --> Interlobar Arteries --> Arcuate Arteries --> Interlobular Arteries --> Afferent Arterioles --> Glomerular Capillaries --> Efferent arterioles --> Peritubular Capillaries --> Interlobular Veins --> Arcuate Veins --> interlobar Veins --> Renal Vein
|
|
|
How the Nephron Works
|
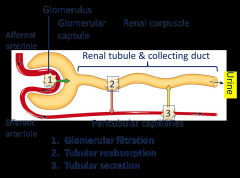
1. Glomerular Filtration - moving blood from glomerulus into the nephron itself
2. Tubular Reabsorption - when we take material that are in the urine that we want to reclaim back into the blood 3. Tubular Secretion - what we want to get rid of in the blood we secrete out Afferent arterioles go into glomerular capsule (glomerular capsule + glomerulus = renal corpuscle) |
|
|
Glomerular Filtration
|
150-180 liters day (65x blood plasma volume)
1-2 L of urine daily Filtration membrane (endothelial-capsular membrane) Mesangial cells - smooth muscle cells - Extraglomerular - regulate blood pressure (RAA) - Intraglomerular - regulate glomerular filtration rate |
|
|
Renal Corpuscle
|
Glomerular capsule + glomerulus
Bunch of cells called podocytes - help regulate the movement of material out of the capillaries and into the capsule that will then become filtrate |
|
|
Filtration Membrane
|
Three Filters
- Fenestration (pore) of Glomerular Endothelial Cell: prevents filtration of blood cells - Basal Lamina of Glomerulus: prevents filtration of larger proteins - Slit Membrane Between Pedicels: prevents filtration of medium-sized proteins |
|
|
Cortical Nephron
|
Renal corpuscles lie in the outer portion of the renal cortex - loops lie mainly in the cortex and penetrate only into the outer region of the renal medulla
Ubiquitous - found everywhere Shorter nephron loops Lower GFR |
|
|
Juxtamedullary Nephron
|
Less common
Higher GFR Longer nephron loops - extend into the deepest region of the medulla - thin/thick limbs (two different portions - both ascending limbs), vasa recta (receive blood from here) More concentrated urine |
|
|
Glomerulonephritis (GN)
|
Inflammation of kidney (glomeruli)
Suite of diseases - Common: allergic reaction to Strep. toxins (IgA nephropathy, aka Berger's disease) Filtration membranes pass blood and protein Hematuria, possibly proteinuria May lead to chronic renal failure (25-35%) |
|
|
Proximal Convoluted Tubule
|
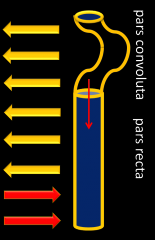
Major site of reabsorption**
- Salts and H2O (~66%), glucose and amino acids (100%), citrate (~80%), PO4 3- (~80%), K+ (~65%), Urea (~50%) - all of these move back into the blood Two regions: pars convoluta (allows things back into the blood) and pars recta (allows things out) Things that go out of blood: medications, NH4+ In order to move water across a membrane, need to set up an osmotic gradient - move sodium and then water follows the sodium |
|
|
Nephron Loop (of Henle)
|
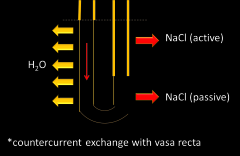
Enter nephron loop from the proximal tubule
Two distinct regions: descending loop and ascending loop Descending - reabsorb water Ascending - reabsorb salts (NaCl) Bottom portion where it is thinner is more passive and upper portion where it is thicker have more active movement Specialized vessels called vasa recta - vessels that are straight and they set up a counter-current exchange as to extract water from the loop of Henle as best as possible - allows us to have more concentrated urine by absorbing water out - important for desert-dwelling organisms Juxtamedullary nephons have vasa recta too |
|
|
Distal Convoluted Tubule and Collecting Ducts
|
Both reabsorption and secretion
- Absorb water - vasopressin works on principle cells - Absorb Ca2+ - Move sodium back in as a response to more water - modulated by aldosterone Opportunity to use the kidneys to help regulate pH - secrete and/or absorb HCO3 and H+ - help maintain pH |
|
|
Juxtaglomerular Apparatus
|
Regulates renal blood flow and GFR which is also important to blood pressure**
Macula densa (good chemoreceptors - can detect the ratio of certain solue namely salts/water in urine and act accordingly in respect to the body) --> paracrine vasopressor Juxtaglomerular cells --> renin Proximal to the distal tubule Mesangium cells - extraglomerular (found outside can help regulate pressure in the arterioles) intraglomerular (can regulate filtration rate) |
|
|
Diuretics
|
Slow renal reabsorption of water via diuresis
Reduce blood volume Treat hypertension Caffeine (increases glomerular filtration rate) Alcohol (inhibits ADH production) - 1 g. consume --> urine excretion increase ~10 mL |
|
|
Renal Failure
|
Acute
Chronic |
|
|
Acute Renal Failure (ARF)
|
Suppression of urine flow
- Oliguria: daily urine output 50-250 mL - Anuria - daily urine output < 50 mL - Low blood volume, damaged tubule, allergic reaction, trauma, etc. |
|
|
Chronic Renal Failure (CRF)
|
Progressive and irreversible
End stage: 90% of nephrons lost, GFR 10-15% of baseline Require dialysis or transplant (if they don't have compensation from the other side) Can manage with one kidney |
|
|
Dialysis
|
Hemodialysis - blood filtered by machine
Continuous Ambulatory Peritoneal Dialysis (CAPD) - peritoneum used as a filtration membrane - Sterile dialysis solution collects waste products in the peritoneum, then is drained |
|
|
Urine Transport
|
Bilateral uterers: length - 25-30 cm diameter - 1-10 mm
Layered - Adventitia - Muscularis - Mucosa: transitional epithelium + lamina propria Peristalsis, hydrostatic pressure, gravity - Peristaltic waves 1-5 per minute - Innervated by the renal plexus Physiolgical valve (pressure) distally From the minor calyces --> major calyces --> pelvis --> ureters --> transported down to urinary bladder |
|
|
Ureter Histology
|
Different layers of the tissue - innermost layer is transitional epithelium (distensible - can be stretched)
Layer of smooth muscle (muscularis) - squeezes urine downwards (though most of it is done through gravity) - important for moving kidney stones |
|
|
Urine Transport and Storage
|
Urine will end up in urinary bladder - has extreme amount of smooth muscle - can expand or contract depending on conditions
Trigone - formed by where the ureter opens Internal Urethral Orifice - has sphincter and enters the urethra (where urine comes out) afterwards Urethral openings have no sphincters on them but there are physiological valves to close them off - when the bladder fills up to 300-400 mL it will tip backwards and will seal off the openings so urine doesn't flow back up into the urethra - have specialized bear receptors that will let you know when you have to go |
|
|
Female Pelvis
|
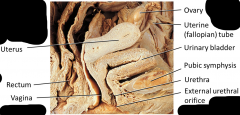
Urinary bladder
Urethra - generally located just external to the vagina posterior to the clitoris (sometimes inside which is not uncommon) |
|
|
Urinary Bladder
|
Average capcity = 700-800 mL
Trigone Internal urethral orifice and sphincter (smooth) External urethral sphincter (skeletal muscle) Vesical (superior, middle, inferior) arteries Innervation: - Nerves from hypogastric plexus - Pelvic splanchnic nerve (S2 and S3) |
|
|
Micturition
|
S2 & S3 segments = micturition center
Micturition Reflex - 200-400 mL --> baroreceptor activation - S2 & S3 segments = micturition center - Parasympathetic --> detrusor contraction and internal uretrhal sphincter relaxation (this is where you'll make a decision consciously to slench that skeletal muscle sphincter) - Inhibits SMNs to external urethral sphincter - May be voluntarily halted Cortical control too |
|
|
Incontinence
|
Lack of voluntary control over micturition reflex
Normal in children under 2-3 Stress incontinence: young females - Weak pelvic floor musculature Urge incontinence: elderly - Irritation of urinary bladder Overflow Incontinence - involuntary leakage Functional incontinence |
|
|
Female Urethra
|
~4 cm
External urethra orifice typically between the clitoris and vagina Layered: - Muscularis - Mucosa: epithelium and lamina propria - Transitional --> Columnar --> Stratified squamous epithelium |
|
|
Male Urethra
|
~20 cm
Urine and semen Three regions: - Prostatic urethra: through prostate - Membranous (intermediate) urethra: under perineal muscles - Spongy urethra: through penis Glands: prostate, seminal vesicles, bulbourethral (Cowper's) glands, and urethral (Littre) glands |
|
|
Differences between Male and Female Urethra
|
Females have dedicated urethra only for urine - males urethra serves as a place for urine and gametes - males have prostate gland and seminal vesicles which secrete components for semen which are delivered up through the vas deferens where they are stored waiting for ejaculation
Men and women have different regions of the urethra Women are more susceptible to UTI - shorter urethra which is also closer to the rectum |
|
|
Urinalysis
|
95% water
5% solutes - Urea, ions, metabolic wastes |
|
|
Development of Urinary System
|
Mesoderm --> intermediate mesoderm (located on the urogenital ridges - kidneys and gonads come from intermediate mesoderm)
Pronephros (and pronephric duct) - degenerates and disappears @ 6th week Mesonephros (and mesonephric duct) - degenerates and disappears @ 8th week Mesonephric duct --> Uteric bud Metanephros Cloaca --> urogenital sinus and rectum Three kidneys develop: prnephros, mesonephros, and metanephros (sticks around) Gonads and kidneys develop from the same source of tissue** |
|
|
Abnormalities of Development of Urinary System
|
Unilateral renal agenesis (1/1,000 births, males)
Malrotated kidneys Ectopic kidney Horseshoe kidney |
|
|
Aging and the Urinary System
|
kidneys decrease in size with age
blood flow and filtration decreases - Rates decline 50% between age 40-70 - At 80, only 60% of glomeruli are functioning Polyuria, nocturia, dysuria Incontinence Hematuria |
|
|
Digestive System Anatmoy
|
Muscular tube open at both ends with attached accessory structures - two major parts
- Gastrointestinal Tract - Accessory Digestive Organs |
|
|
Gastointestinal Tract (Alimentary Canal)
|
Oral cavity --> Pharynx (oro + laryngo) --> Esophagus --> Stomach --> Small Intestine --> Large Intestine
|
|
|
Accessory Digestive Organs
|
Teeth, tongue, salivary glands, gall bladder, liver, pancreas
|
|
|
GI Tract Functions
|
Mouth - bite, chew, swallow
Pharynx and esophagus - transport Stomach - mechanical disruption; absorption of water and alcohol Small Intestine - chemical and mechanical digestion and absorption Large intestine - absorb electrolytes and vitamins (B and K) Rectum and anus - defecation |
|
|
Layers of the GI Tract
|
Mucosal layer - helps to lubricate - humidifes the air keeping the mucosa from cracking and letting pathogens in
Submucosal layer - may have blood vessels running through Muscularis layer - two layers - longitudinal and circular muscle fibers all through GI tract - Circular ones act like sphincters - mouth is the first sphincter - help squeeze food through Parasympathetic - digestion and sex Sympathetic - running, heart rate increase, increase airflow in lungs Serosa layer - has serous fluid that allows things to slip around (don't want them sticking together) |
|
|
Peritoneum
|
Double-layer serous membrane covers some of the digestive system structures = 2 layers
- Parietal layer: lines abdominopelvic wall and folds back on itself forming a double membrane = mesentary - lines the walls of body cavity - Visceral Layer - covers organs Peritoneal Cavity - potential space containing a bit of serous fluid |
|
|
Functions of Mesentary (parietal layer of peritoneum)
|
Supports the intestines = mesocolon; stomach = omenta: and liver = falciform ligament
Prevents intestinal twisting Stores fat Pathway for blood vessels and nerves |
|
|
Greater Omentum
|
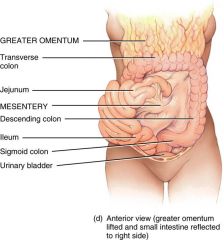
type of mesentary - (mesentary = folds of serous membrane that connect the organs to the cavity wall)
grows faster than normal the more fat you put on your body, the more blood vessels you have to make and then your heart has to work harder to pump blood through the body Only attached through the transverse colon and the stmoach |
|
|
Lesser Omentum
|
attaches the stomach to the liver
Ligament - describes an attachment of one organ to another organ by some sort of connective tissue |
|
|
Peritonitis
|
Acute inflammation of the peritoneum
Cause: contamination by infectious microbes during surgery or from rupture of abdominal organs |
|
|
Oral Cavity (Buccal Cavity) - Mouth
|
Lined with epithelium - non-keratinized stratified epithelium - withstands abrasion from masticated food
Buccinator - innervated by facial nerve Boundaries - Anterior = lips (labia) --> orbicularis oris mm - mucus membrane on inner surface - lips attached to gums by labial frenulum - Lateral = cheeks = formed by buccinator mm. - covered by mucus membrane on inside - Superior = palate (hard = maxillary bone & soft = skeletal mm) - Inferior = tongue - accessory digestive organ (2/3 oral cavity - anchored by lingual frenulum) (1/3 oropharnyx) |
|
|
Tongue
|
Rough due to Papillae (three types)
1. Filliform - cone-shaped, smallest, no taste buds, most abundant type, friction for licking 2. Fungiform - mushroom-shaped, well-vascularized (red tongue), has taste-buds 3. Vallate - 12 large papillae, inverted "V" shape, back of tongue, has taste buds |
|
|
Chemoreceptors
|
Olfactory (smell) and gustatory (taste): for receptors to work, chemicals must be volatile and soluble in water
Olfactory epithelium - top of nasal cavity at the bottom of the ethmoid bone - olfactory foramina allows neurons to get to the olfactory bulbs on the brain Location of olfactory receptors: 1. Olfactory epithelium 2. Olfactory receptor cells 3. Supporting cells 4. Basal cells 5. Olfactory sensory fibers |
|
|
Special Senses
Chemoreceptive Senses |
responsive to chemicals in aqueous solution
Taste |
|
|
Taste
|
Location of taste buds
- Oral cavity, 10,000 buds on infant tongue, papillae (3 forms - filiform, fungiform, circumvallate) |
|
|
Structure of Taste Buds
|
Gustatory Hairs
Gustatory Pores Gustatory Taste Cells Basal Cell Sensory Nerve Fiber Series of cells that help papillae for taste - know general idea that there are different taste receptors buried in various papillae and are useful for tasting different things |
|
|
Taste Sensations - Receptors
|
![1. Sweet 2. Salty 3. Sour 4. Bitter [Water Receptors and Umami Receptors]
Sweet and salty at the front of the tongue
Umami receptors - good for savory things [MSG binds well with theses]
Can have receptors all over the place](https://images.cram.com/images/upload-flashcards/99/29/91/4992991_m.png)
1. Sweet 2. Salty 3. Sour 4. Bitter [Water Receptors and Umami Receptors]
Sweet and salty at the front of the tongue Umami receptors - good for savory things [MSG binds well with theses] Can have receptors all over the place |
|
|
Teeth
|
Mastication
4 types: - Incisors (8) for cutting - Canines (4) tearing and piercing - Premolars (8) grinding and crushing - Molars (12) grinding and crushing 32 teeth total in adult |
|
|
Baby Teeth
|
milk teeth are temporary
Incisors: 8 Canines: 4 Molars: 8 20 total teeth Premolars are missing in children - mandible isn't big enough for all adult teeth |
|
|
Dental Formula
|
Divide mouth into four quadrants
Top Row: 2 1 2 3 Bottom Row 2 1 2 3 Order (l -> r) I; C; P;M |
|
|
Teeth Structure
|
Pulp cavity
Dentin Enamel Gingivitis - bacterial infection of gums Plaque - sticky matrix on surface of teeth made by bacteria + trapped food particles - if hardens - tartar |
|
|
Pulp Cavity
|
center of tooth; receives BV's and nerves from the root canal (narrow tunnel at base of tooth) which support and nourishes the dentin
|
|
|
Dentin
|
non-living boney matrix of tooth
- Largest portion of tooth - Surrounded by enamel |
|
|
Enamel
|
above the gum (gingiva) line only
- Hardest known biological substance made of calcium phosphate crystals (Vitamid D and Calcium) |
|
|
Salivary Glands Composition
|
Fluid = Saliva
pH = 7.0 1-1.5 L/day Composition 1. 97% water 2. Immunoglobulin A, 3. Lysozyme 4. Na+, K+, HCO3-, Cl- 5. Amylase: digestive enzyme breaks down sugars 6. Mucus Swallowing reflex is inhibited when you are asleep - breathing and vomiting can happen during sleep - do not make saliva while you are asleep Drooling because there is still saliva in your ducts when you fall asleep |
|
|
Salivary Glands Function
|
1. Cleanse mouth
2. Antibacterial 3. Carbohydrate digestion started 4. Aids in chewing and swallowing |
|
|
Salivary Glands Types
|
Intrinisic = inside oral cavity
- buccal glands Extrinsic = 3 types - outside oral cavity and connected by salivary ducts 1. Parotid 2. Submandibular 3. Sublingual |
|
|
Parotid - Extrinsic Salivary Gland
|
Largest
Infected with Myxovirus = mumps Parotid (Stensen's) Duct = connection to oral cavity Adult males with mumps = sterilization If mumps were to afflict us now, we could get pancreatitis which could lead to diabetes |
|
|
Submandibular - Extrinsic Salivary Gland
|
Beneath mandible - found on the angle of the mandible - gland will fall down to the neck that looks like jowels - classic gleaking gland (saliva will come shooting out of it)
Submandibular (Wharton's) ducts |
|
|
Sublingual - Extrinsic Salivary Gland
|
Under tongue - found between your lower gum of the mandible and the base of your tongue - 12-18 ductules that drain that gland up to the mouth
Sublingual (Rivinus') Ducts Oropharynx - common to both the respiratory and digestive system |
|
|
Physiology of the Esophagus - Swallowing
|
Voluntary phase - tongue pushes food to back or oral cavity
Involuntary phase - pharyngeal stage - Breathing stops and airways are closed - Soft palat and uvula are lifted to close off nasopharynx - Vocal cords close - Epiglottis is bent over airway as larynx is lifted |
|
|
Swallowing
|
Upper sphincter relaxes when larynx is lifted
Peristalsis pushes food down - Circular fibers behind bolus - Longitudinal fibers in front of bolus shorten the distance of travel Travel time is 4-8 seconds for solids and 1 second for liquids Lower phincter relaxes as food approaches |
|
|
Peristalsis
|
Wave-like contractions of the smooth muscle tissue
|
|
|
Gastro-esophageal Junction
|
Way for gases to come back up - burps
Escape mechanism for these gases Phreno-esophageal Ligament - allows the stomach to move up when it tears - causes hernias which is an unnatural opening in a muscle |
|
|
Hernias
|
Acid rich - cause heartburn
Sliding hiatus hernia - most common If you pinch off the blood supply to the fundus (dome) then it can rupture and that's bad - may try to push it back down through surgery Symptoms of hernias: heartburn, metallic taste in mouth, wet burps Esophogeal Cancer - cut it out - pull stomach up and attach it to the base of the throat and eat that way |
|
|
Complications of Peptic Reflux
|
Peptic esophagitis
Inflammation of esophageal wall Ulceration |
|
|
Stomach
|
Body of the stomach - where most digestion happens
Constriction - junction between the end of the stomach and the duodenum - causing the restriction is a strong sphincter called the pyloric sphincter Duodenum is not well developed to deal with a lot of acid coming through which is the necessity of the pyloric sphincter |
|
|
Historical Perspective of Stomach
|
Martin - patient of Beaumont - look into his stomach any time he wanted to
For years Beaumont studied him to figure out the function of the stomach Stomach stores food for about 4 hours, while it is storing it is breaking it down using pepsin and other acids, and mechanically mixing it |
|
|
Muscularis Externa
|
3 mm layers
1. Outer = longitudinal 2. Middle = Circular 3. Inner = Oblique Helps to undulate the food and mechanically mix it with the acids that are in there The nerve that controls this parastaltically? - vagus nerve (epiglottis controlled by vagus as well) Vagus controls first 2/3s of large intestine as well Vagus also slows down your heart and constrict airways in your lungs |
|
|
Gastric Rugae
|
Mucosa + Submucosa
Inside the stomach are rugae Present when stomach is empty and go away when the stomach expands Don't confuse rugae with the gastric pits - gastric pits are microscopic while rugae are macroscopic - you can see them when the stomach is empty |
|
|
Gastric Pits
|
Have to distend the stomach to see them
Some are called parietal calls (make hydrochloric acid and intrinsic factor which helps with B12 absorption which helps with new red blood cell production) Chief cells make pepsin which is an enzyme that helps digestion of proteins |
|
|
Gastric Emptying
|
slow process
- Gastrin and PSN Promotes; SNS inhibits 4 hours to empty after eating Food lingers in stomach the longest of GI organs Food --> Chyme Chyme emptied to duodenum via pyloric sphincter |
|
|
Chronic Gastric Ulcer
|
Causes: hydrochloric acid, pepsin
Helicobacter pylori |
|
|
Hepatic Portal Triad
|
Vein, common bile duct, artery
|
|
|
Omental Bursa
|
Stomach: transverse colon attached to the greater omentum
Bed of the stomach is the pancreas because it's blocked by the stomach and spinal column and ribs behind it Tranverse mesocolon hangs from the spleen - ribs - 8; blood balloon - capsule ruptures very easily - most common for internal bleeding |
|
|
Gastric Arteries
|
Lots of vascularity to stomach
Lipid soluble enter the blood system Celiac trunk branches to other organs: splenic artery (supplies the spleen and major tributary to the pancreas) liver and gall bladder from proper hepatic Stomach is a foregut organ through middle of duodenum |
|
|
Gastric Veins
|
Veins that parallel the arteries
Hepatic portal vein and is the key goal for blood drainage from the gut to the capillaries then to the hepatic vein on top of liver then to the inferior vena cava Splenic vein contribute to the hepatic portal vein Superior mesenteric vein contribute to the hepatic portal Inferior and superior messenteric vein (high gut = inferior, mid gut (first 2/3 of the intestin) = superior) |
|
|
Superior Mesenteric Artery and Vein
|
both come from under the pancreas
|
|
|
Mechanical Digestion - Physiology
|
Gentle mixing waves - every 15-25 seconds - mixes bolus with 2 quats/day of gastric juice to turn it into chyme ( a thin liquid with nutrients)
More vigorous waves - travel from body of stomach to pyloric region Intense waves near the pylorus - open it and squit out 1-2 teaspoons full with each wave Major enzyme - pepsin which works well in the presence of hydrochloric acid |
|
|
Chemical Digestion - Physiology
|
Protein digestion begins
- HCl denatures (unfolds) protein molecules - HCl transfoms pepsinogen into pepsin that breaks peptides bonds between certain amino acids Fat digestion continues - Gastric lipase splits the trigktcerides in milk fat - Most effective at pH 5-6 (infant stomach) Hcl kills microbes in food Mucous cells protect stomach walls from being digested with 1-3 mm thick layer of mucous |
|
|
Cephalic Phase
|
"Stomach Getting Reading"
Cerebral cortex - sight, smell, taste, and though - Stimulate paraympathetic nervous system Vagus nerve - Increases stomach muscle and glandular activity (fore gut and mid gut; not hind gut) |
|
|
Sympathetic and Paraympathetic Neurotransmitters
|
sympathetic neurotransmitter - inhibit digestion
paraympathetic neurotransmitter - cause digestion to increase Acetylcholine (in muscles) - gastric motility and secretion Vagus nerve ends when you get to the large intestine Sympathetic everywhere in body but parasympathetic only near spinal chord |
|
|
Absorption of Nutrients by the Stomach
|
Water especially if it is cold
Electrolytes Some drugs (especially aspirin) and alcohol Fat conent in the stomach slows the passage of alcohol to the intestine where absorption is more rapid Gastric mucosal cells contain alcohol dehydrogenase that converts some alcohol to acetaldehyde - more of this enzyme found in males than females Females have less total body fluid that same size male so end up with high blood alcohol levels with same intake of alcohol |
|
|
Vomiting (Emesis)
|
Forceful expulsion of contents of stomach and duodenum through the mouth
Cause: Irritation or distention of stomach Unpleasant sights, general anesthesia, dizziness and certain drugs Sensory input from medulla cause stomach contraction and complete sphincter relaxation Contents of stomach squeezed between abdominal muscles and diaphragm and forced through open mouth Serious because loss of acidic gastric juice can lead to alkalosis |
|
|
Small Intestine
|
Convoluted Tube - length varies with muscular tone
Longest part of GI; smallest in diameter Extends from Pyloric Sphincter --> Ileocecal valve Diameter - 2.5 cm 3 Regions: Duodenum, jejunum, ileum |
|
|
Duodenum
|
10 in. long: superior part (retroperitoneal)
3 accessory organs associated - Pancreas (Pancreatic duct) - Gall bladder (Cystic D.) - Liver (Hepatic D.) Features Brunner's Glands - makes alkaline mucus that neutralizes chyme Purpose - absorption |
|
|
Jejunum
|
Smaller than duodenum because more absorption that occurs less comes out
|
|
|
Liver - Characteristics and Key Functions
|
Largest internal organ
4 Lobes: Right and left lobes anchored by falciform ligament; Caudate and Quadrate (underside) Digestion: - Bile production (alkaline yellow-green fluid): break down heme - Bile salts (cholesterol derivative): emulsify (break droplets apart) large fat globules for enzyme attack |
|
|
Functions of Liver
|
Destroys or store toxins
Remove foreign debris or old RBC's, hormones in circulation, antibodies Plasma protein synthesis (hepatocytes) Albumin - #1 protein in blood (WBC) |
|
|
Gallbladder - Characteristics and Functions
|
Muscular, greenish sac attached to liver (ventral side)
Stores and concentrates bile (released thru Cystic duct) Common Bile Duct + Pancreatic Duct = Hepatopancreatic Ampulla --> Duodenal Papilla Opening is controlled by Hepatopancreatic Sphincter (Sphincter of Oddi) The hormone Cholecystokinin (CCK) Cx of gallbladder and releases Sphincter of Oddi = releases bile and pancreatic juices to duodenum |
|
|
Pancreas Characteristics and Functions
|
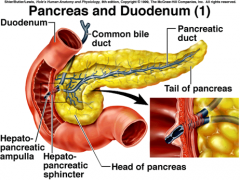
Tadpole shaped gland
Retroperitoneal Endocrine Gland - insulin, glucagon, somatostatin - inhibits (islet cells) Exocrine Gland - pancreatic juice (acini cells) - Water, HCO3-, amylase (starch digestion), lipase (fat digestion), endopeptidases (protein digestion) [ex. Chymotrypsin - cleaved from Chymotrypsinogen = zymogen) Juices delivered to duodenum by merger of pancreatic duct with common bile duct --> duodenal papilla |
|
|
Duct Pathways of Digestion System
|
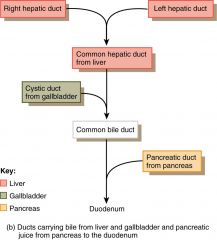
|
|
|
Jejunum - Small Intestine Region
|
Middle portion
between duodenum and ileum 8 ft long Larger lumen > ileum absorption of nutrients |
|
|
Ileum - Region of Small Intestine
|
Longest section of SI
Posterior portion Terminates at the Ileocecal Valve (opens into the cecum of the LI) Peyer's Patches (MALT) fight infection - within the walls of intestine |
|
|
Structural Modification of Small Intestine
|
4 Tunics aid absorption
Plicae Circulares (circular folds) Villi (finger=like) Microvilli All of these structures increase SA = 200 m2 |
|
|
Plicae Circulares (Circular Folds) Small Intestine
|
deep folds of mucosa and submucosa (1 cm tall) --> chyme spirals through - mixes with enzymes
|
|
|
Villi - Structural Modification of Small Intestine
|
projections of mucosa (simple columnar epithelium cells)
Anchored to lamina propria (BV's and LV's) Narrow pouched between Villi - Intestinal Crypts - Deep in crypts are paneth cell - lysozyme |
|
|
Microvilli
|
Hair-like projections of the cell membrane of villi
Brush Border - enzymes for protein, sugar, and carbohydrate digestion |
|
|
Function of Small Intestine
|
Digestion
Absorption - Monosaccharides, amino acids, water, lipids, vitamins, electrolytes |
|
|
Ileocecal Region
|
Colon - part of large intestine
Cecum - first 6 inches Appendix - full of MALT tissue for the large intestine |
|
|
Large Intestine
|
Extends from Ileocecal Valve to Anus
Length - 5 ft; Diameter - 2.5 in 4 Regions: - Cecum, Colon, Rectum, Anal Canal |
|
|
Cecum - Region of Large Intestine
|
First region of large intestine
Sac-like portion beneath ileocecal valve Appendix hangs from medial surface in lower right quadrant MALT: traps enteric bacteria = infection = appendicitis |
|
|
Appendix
|
Served by its own artery
|
|
|
Mucosa and Musculature of Large Intestine
|
Bands (haustra) are used for creation stronger peristaltic waves to move the condensed leftovers along
Splenic and hepatic flexure are located at the turns of the intestine |
|
|
Colon - Region of Large Intestine
|
4 Subdivisions
1. Ascending colon: right side of abdominal cavity makes 90 degree turn under liver = hepatic flexure 2. Transverse colon: horizontal across abdominal cavity turns down under spleen = splenic flexure 3. Descending colon: down left side of abdominal cavity 4. Sigmoid Colon: S-shaped portion in pelvic cavity |
|
|
Rectum - Region of Large Intestine
|
Continuous with sigmoid colon
Stores feces Rectal valves: transverse folds separate feces from flatus (intestinal gas) Colonic bacteria produce flatus from indigestible carbohydrates (beans, broccoli) Stretching rectal walls initiates defecation reflex |
|
|
Anal Canal - Regions of Large Intestine
|
Opens to exterior via anus
Lined with stratified squamous epithelium 2 Anal sphincters - Internal Anal Sphincter (smooth mm) - involuntary - External Anal Sphincter (skeletal mm) - voluntary |
|
|
Structural Modification of Large Intestine
|
Structural modifications
- Muscularis Externa - Haustra - Epiploic Appendages |
|
|
Muscularis Externa - Structural Modification of Large Intestine
|
Teniae coli "tiny ribbons" - 3 bands of smooth muscle
Function: produce powerful and long lasting peristalsis - moves large quantities of chyme to rectum (3x/day) |
|
|
Haustra - Structural Modification of Large Intestine
|
Sac-like pouches of colon wall
Haustral Cx - slow segmentation of chyme (every 30 min) - mix, churn, and absorbs water and electrolytes from chyme |
|
|
Epiploic Appendages
|
Fat-filled bags hanging from serosa
Function - unknown |
|
|
Function of Large Intestine
|
Formation of feces from indigestible materials
Absorption of vitamin K, B, and 1800 mL of water/day 200 mL of H2O in feces |