Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
What XR view can be done to diagnose a sternoclavicular joint dislocation?
|
Serendipity View (or CT scan)
Serendipity view: Patient supine, beam is angled 40 deg. cephalad off verticle centered on the sternum |
|
|
What is the most common SC joint dislocation direction and how is it treated?
|
Anterior dislocation—more common, treated by closed reduction. The majority will remain unstable regardless of initial treatment modality, but these are typically asymptomatic
|
|
|
What is the most serious direction of dislocation of the SC joint and how is it treated?
|
Posterior dislocation—more serious—30% associated with significant compression of posterior structures. May cause dysphagia or difficulty breathing and sensation of fullness in the throat. Treated by closed reduction with a towel clip in the operating room. A thoracic surgeon should be on standby
|
|
|
How is chronic dislocation of the SC joint treated?
|
Chronic dislocation—treated by resection of the medial clavicle, with preservation and reconstruction of costoclavicular ligaments
|
|
|
What is a pseudodislocation of the SC joint (bold)?
|
Pseudodislocation—The medial clavicular epiphysis is the last to close at a mean age of 25 years. In patients younger than this, sternoclavicular dislocation is often a Salter-Harris type I or II fracture
|
|

What is the most common location for a clavicle fracture?
|

▪ Middle—80%
▪ Distal—15% ▪ Medial—5% When the distal end of the clavicle is fractured, the ligaments may either remain intact and maintain apposition of the fracture fragments (type I) or rupture, allowing wide displacement of the fragments (type II) |
|
|
What 2 non-orthopedic injuries are open clavicle fractures associated with? (bold)
|
Open clavicle fractures are associated with high rates of pulmonary and closed-head injuries
|
|
|
Most mid-third clavicle fractures are treated nonoperatively in a sling.
Is there a difference with figure 8 sling vs regular? What populations and fractures characteristics have a higher risk of nonunion? (All Bold) |
No difference in outcome regular sling vs figure of 8
Females and elderly are at higher risk of nonunion. Comminuted fractures and fractures shortened > 2cm have a higher risk of nonunion Lateral fractures have a higher risk of nonunion than midshaft |
|
|
What are options for fixation off clavicle fractures?
|
Dynamic compression plate: Can be place superiorly (better strength, more prominent so more commonly requires removal) or anteroinferiorly
IM rod and screw can be placed percutaneously but have higher rates of hardware irritation and complication |
|
|
What is the classification system for proximal humerus fractures?
|
Neer. Described as parts where a part is > 1cm or 45-degree displacement. Parts are the articular surface, greater tuberosity, lesser tuberosity, and shaft
One-part (most common): Impaction of the humeral neck. Tx with sling for comfort and early motion Two-part: Displacement of greater tuberosity > 1cm. Repair ranges from close to ORIF Three-part: Displacement of greater or lesser tuberosities and articular surface Four-part: Displacement of shaft, articular surface, and both tuberosities. "Head splitting" is a variant, with split through the articular surface |
|
|
What percentage of bone stock loss in a hill sachs lesion leads to instability?
|
< 20% is stable
20-50 is unstable and can tx with xfrer of lesser tuber. > 45 is unstable and tx w/ prosthesis vs rotational osteotomy |
|
|
What is a term for a Fracture of the glenoid neck and clavicle
|
Floating shoulder
|
|
|
What would nonunion of a greater tuberosity following arthroplasty for proximal humerus fractures cause?
|
Loss of active shoulder elevation (pseudoparalysis)
|
|
|
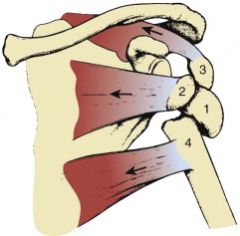
What are the VI classes of AC separation?
|
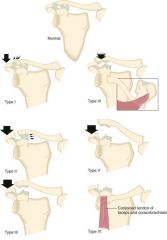
In a type I injury, a mild force applied to the point of the shoulder does not disrupt either the AC or coracoclavicular (CC) ligament. In a type II injury, a moderate to heavy force applied to the point of the shoulder disrupts the AC ligaments but the CC ligaments remain intact. In a type III injury, when a severe force is applied to the point of the shoulder, both the AC and the CC ligaments are disrupted. In a type IV injury, not only are the ligaments disrupted but the distal end of the clavicle is also displaced posteriorly into or through the trapezius muscle. In a type V injury, a violent force applied to the point of the shoulder not only ruptures the AC and CC ligaments but also disrupts the muscle attachments and creates a major separation between the clavicle and the acromion. A type VI injury is an inferior dislocation of the distal clavicle in which the clavicle is inferior to the coracoid process and posterior to the biceps and coracobrachialis tendons. The AC and CC ligaments have also been disrupted
|
|
|
When can a humeral shaft fracture be treated nonoperatively? When is operative fixation required?
|
Functional bracing if there is less than 20 degrees of anterior angulation, less than 30 degrees of varus/valgus angulation, or less than 3cm of shortening
Operative fixation: Open fracture, floating elbow, polytrauma, pathologic fracture, associated brachial plexus injury |
|
|
With humeral shaft fracture fixation, what are the risks of using a nail vs plate fixation?
What is the concern with placement of distal locking screws? |
A nail may have a higher complication rate associated with higher reoperation rates. Nails have higher incidence of shoulder pain
Distal locking screws: radial nerve at risk with lateral to medial screws. Musculocutaneous nerve with anteroposterior screws |
|
|
What is a common complication of humeral shaft fractures?
|
Radial nerve palsy (5-10%). Up to 92% reesolve with observation for 3-4 months. Brachioradialis and ECRL are the first to return. EPL and EIP are the last (last innervated nerves)
Explore the radial nerve with the following: open fractures, consider after secondary palsy (new palsy after reduction), spiral or oblique fractures of distal third (Holstein-Lewis fractures) |
|
|
What are the classifications of a capitellum fracture?
|
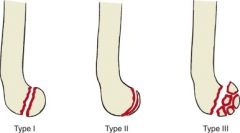
Type I: Hahn-Steinthal; complete fracture
Type II: Kocher-Lorenz; shear fracture of articular cartilage Type III: Comminuted McKee Modification Type IV - Coronal shear fracture including capitellum and troachlea |
|
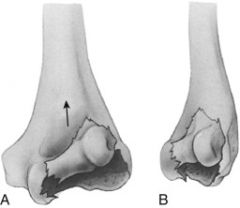
What is this depicting?
|
A Type IV capitellum fracture in which there is a coronal shear fracture including the capitellum and trochlea
|
|
|
What is the classification system for olecranon fractures?
|
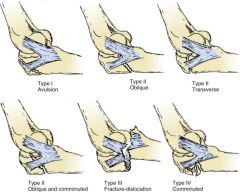
Colton Classification:
Type I: Avulsion Type II (A-D): Oblique fractures with increasing complexity Type III: Fracture-dislocations Type IV: Atypical high-energy multifragmented fractures |
|
|
What is the classification system for coronoid fractures?
|
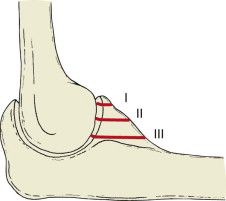
Regan and Morrey classified into 3 types:
Type I: Fracture of the tip of the coronoid process Type II: Fracture of 50% or less of the coronoid Type III: Fracture of more than 50% |
|
|
What is the classification system & treatment for radial head fractures?
|

Type I - Nondisplaced (splint for no more than 7 days then allow motion)
Type II - Partial articulation with displacement (Nonsurgical, pain mgmt & active ROM if elbow is stable & no block to motion with good reduction; otherwise ORIF) Type III - Comminuted fractures involving the entire head (Radial head replacement. ORIF if fewer than 3 pieces. Excise only in elderly low-demand patients) Type IV - Fractures associated with ligamentous injury or other fractures (requires surgical repair with ORIF or radial head replacement; do not excise) |
|
|
What is the safe zone for ORIF of radial head/neck fractures?
How do you avoid PIN injury when performing ORIF for the radial head? |
110-degree arc (i.e., 25%) along lateral side, defined by radial styloid and Lister tubercle
Pronate the arm to avoid PIN injury |
|
|
What are the types of simple (no assoc. fracture) elbow dislocations and which type is the most common? How are simple dislocations treated?
|
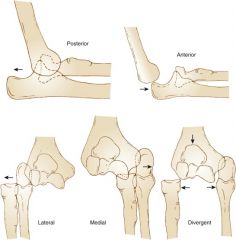
Posterior, Anterior, Lateral, Medial, and Divergent
80% of dislocations are posterolateral. Treatment is with reduction, brief (1 week) immobilization, then allow motion. Long-term results are good |
|
|
What is the terrible triad of the elbow?
|
Elbow dislocation with lateral collateral ligament injury, radial head fracture, and coronoid fracture. The LCL injury is typically a ligamentous avulsion from the origin on the distal humerus
|
|
|
How are terrible triad of the elbow injuries treated?
|
These are always unstable and always require treatment:
Coronoid ORIF Radial head ORIF or replacement LCL repair (typically to distal humerus) Possible MCL repair depending on stability |