Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
234 Cards in this Set
- Front
- Back
|
What are the general characteristics of nematodes (roundworms)?
|
Nonsegmented round worms, flexible outer coating (cuticle), muscular layer underneath cuticle, and contain nervous/digestive/renal/reproductive organs.
|
|
|
What is the morphology of adult Ascaris?
|
Largest (but not longest) intestinal helminth in humans. Up to 40cm long and 6mm wide. Creamy white to pinkish.
|
|
|
What are the clinical minifestations of Ascaris?
|
Most patients are asymptomatic.
GI: 1) mild to moderate abdominal discomfort 2) intestinal obstruction 3) Biliary or pancreatic obstruction from aberrant migration 4) large #s can cause abdominal distension Pulmonary: 1) mild cough 2) Loeffler's syndrome (eosinophilic pneumonitis causing transient pulmonary infiltrate, dyspnea, dry cough, occ fever, and eosinophilia) |
|
|
How do you diagnose Ascaris?
|
Eggs appear in stool 2 to 3 months after infection/pulmonary symptoms occur.
|
|
|
How do you treat Ascaris?
|
Pulmonary disease is self-limiting. For GI disease, use mebendazole (300-500mg) and albendazole (400mg). Single dose therapy appears 100% curative.
|
|
|
What is the epidemiology of Ascaris?
|
Highest intensity infection in children 5 to 15.
|
|
|
What is the prevalence of Ascaris?
|
1 billion worldwide.
|
|
|
Describe the Ascaris life cycle.
|
Embryonated eggs are ingested --> hatch in bowel --> larvae enter bloodstream and migrate over 4-7 days to lungs --> break through alveoli --> ascend airway --> swallowed --> developed into adults that live 1-2 years --> lay eggs that are purged in feces
|
|
|
What is the morphology of Ascaris eggs?
|
Yellow-ish brown, thick shell that appears lumpy/bumpy, and have an internal mass of disorganized granules.
|
|
|
Where is Ascaris found?
|
S. America, Africa, and Asia.
|
|

|
Adult Ascaris
|
|

|
Adult Ascaris
|
|
|
Adult Ascaris
|
|
|
Adult Ascaris
|
|
|
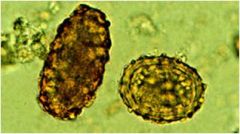
Ascaris eggs (left = unfertilized, right = fertilized)
|
|

|
Ascaris eggs
|
|
|
What is the definitive host of Ascaris?
|
Humans
|
|
|
What is the intermediate host of Ascaris?
|
It doesn't have one.
|
|
|
Hookworm is the common name of what two worms?
|
Ancylostoma duodenale and Necator americanus
|
|
|
Describe the hookworm life cycle.
|
Larvae penetrate skin --> enter bloodstream --> travel to lung, enter alveolar spaces --> swallowed --> mature in small intestine (live for 1-9 years) --> eggs passed in feces --> hatch and develop in soil --> larvae climb blades of grass
|
|
|
What is the definitive host of Hookworms?
|
Humans
|
|
|
What is the intermediate host of hookworms?
|
They don't have one.
|
|
|
What is the morphology of Necator americanus?
|
They have cutting plates and are 0.2-0.4 inches long.
|
|
|
What is the morphology of Ancylostoma duodenale?
|
They have teeth and are 0.3-0.5 inches long.
|
|
|
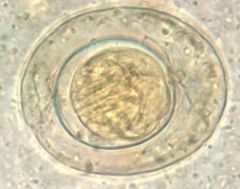
What is the morphology of hookworm eggs?
|
Thin shelled, colorless, and ovoid.
|
|
|
What are the clinical manifestations of hookworms?
|
1) Pneumonitis associated with wheezing, dyspnea, dry cough (usually a few days to weeks after infection) 2) urticarial rash 3) iron deficiency anemia (chronic) 4) mild abdominal pain 5) papulovesicular dermatitis at entry site if sensitized ("ground itch") 6) cutaneous larva migrans if worms migrate laterally
|
|
|
How do hookworms negatively affect pregnancy?
|
Hookworms suck blood (A. duodenale more than N. americanus). This causes IUGR, low birth weight, and stunting.
|
|
|
How do you treat hookworms?
|
Always treat! Mebendazole 100mg BID x 3days or albendazole 400mg once.
|
|
|
What is the epidemiology of hookworms?
|
Highest prevalence in teenage and young adult males; 1/3 of pregnant women in developing world have hookworm.
|
|
|
What is the prevalence of hookworms?
|
600 million worldwide
|
|
|
Where are hookworms found?
|
Most prevalent in warm, humid areas.
N. americanus: N. and S. America, Africa, and India A. duodenale: Europe, Mediterranean, W. coast of S. America Both: China, India, Asia, and S. Pacific |
|

|
Necator americanus (Hookworm)
|
|

|
Acylostoma duodenale (Hookworm)
|
|

|
Acylostoma duodenale (Hookworm)
|
|

|
Acylostoma duodenale (Hookworm)
|
|

|
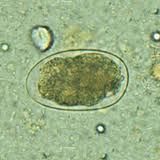
Hookworm egg
|
|
|
Hookworm egg
|
|

|
Hookworm egg
|
|
|
Rhabditifrom form of hookworm larva
|
|
|
Filariform form of hookworm larva
|
|
|
Hookworm
|
|
|
What worm has the common name "Whipworm?"
|
Trichuris
|
|
|
What is the morphology of adult Trichuris?
|
4cm long, hairlike part contains the head, wider part has reproductive organs
|
|
|
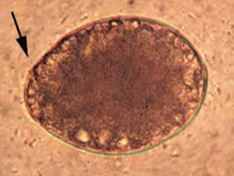
What is the morphology of Trichuris eggs?
|
Barrel-shaped, yellow-brown color, doubly operuclated
|
|
|
What are the clinical manifestations of Trichuris?
|
Usually asymptomatic. Adults live in cecum, so large #s can cause:
1) Loose and infrequent stools with mucus 2) tenesmus (ineffective and painful straining during bowel movements) 3) occ blood to frank blood 4) rectal prolapse in heavily infected children 5) Colitis mimicking IBS (abdominal pain and diarrhea) 6) Impaired growth and anemia |
|
|
How do you diagnose Trichuris?
|
Eggs are doubly operculated; appear in stool 2-3 months post infection.
|
|
|
How do you treat Trichuris?
|
Ivermectin, mebendazole, or albendazole (single does Rx seem good, but for clinically significant infections treat for 3 days)
|
|
|
What is the epidemiology of Trichuris?
|
Highest worm burden is in children
|
|
|
Where is Trichuris located?
|
Worldwide distribution, but more common in tropical areas and regions where sanitation is poor
|
|

|
Adult Trichuris
|
|

|
Adult Trichuris
|
|

|
Trichuris egg
|
|

|
Trichuris eggs
|
|
|
Describe the Trichuris life cycle.
|
Eggs are ingested --> larvae hatch and migrate to cecum where they mature --> Adult weaves head through cytoplasm of several columnar cells (may live 4-8 years)
|
|
|
What is the definitive host of Trichuris?
|
Humans
|
|
|
What is the intermediate host of Trichuris?
|
It doesn't have one
|
|
|
Describe the Strongyloides life cycle.
|
Rhabditiform larvae eggs are shed in stool --> Develop into free-swimming adult worms --> produce eggs --> hatch into rhabditiform larvae --> mature into filariform larvae (infective) --> penetrate skin of host --> travel to lungs and are swallowed --> become adults in intestines --> deposits eggs --> hatch into rhabdiform larvae
NOTE: Rhabdiform larvae can mature into filariform larvae in intestine --> penetrate intestinal lining or skin --> continue rest of life cycle (this path is called "autoinfection") |
|
|
What is the definitive host of Strongyloides?
|
Humans
|
|
|
What is the intermediate host of Strongyloides?
|
It doesn't have one
|
|
|
What is the morphology of rhabditiform Strongyloides larvae?
|
Short buccal cancal and prominent genital primordium
|
|
|
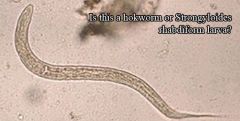
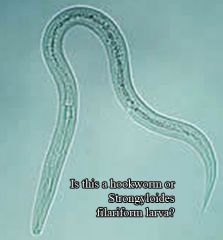
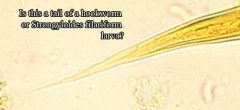
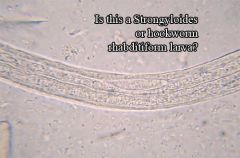
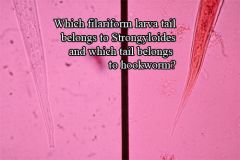
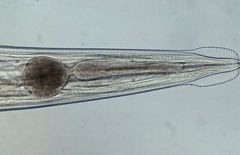
What is the morphology of the filariform Strongyloides larvae?
|
Forked tail and 1:1 esophageal to intestine ratio (hookworm has 1:2 ratio at this stage)
|
|
|
What are the clinical manifestations of Strongyloides?
|
50% of cases are symptomatic: diarrhea, abdominal pain, nausea, and vomiting.
Other GI symptoms: epigastric pain, post-pandrial fullness, heartburn, occ brief diarrhea, occ constipation, blood occ detected Pulmonary: wheezing, transient infiltrates Skin: urticarial rash, larva currens |
|
|
What is hyperinfection syndrome?
|
A combination of an immunocompromised state (usually from high dose steroids) and a large parasite burden (ex: Strongyloides).
GI and pulmonary symptoms are due to large burden of parasites. Neuro: gram negative polymicrobial meningitis Systemic: fever, hypotension --> gram negative sepsis |
|
|
How do you diagnose Strongyloides?
|
Stool O/P has low sensitivity (worm burden is often low, low and irregular egg production, uneven distribution of larvae in feces) so you must do multiple stools on multiple days.
You can also check serology, but sensitivity and specificity vary by lab and it doesn't differentiate between past and present infection. |
|
|
How do you treat Strongyloides?
|
Always treat!
Ivermectin 200ug/kg for 2 days OR albendazole 400mg qd x 3 days OR Thiabendazole 22mg/kg bid x 2 days |
|
|
Does Strongyloides demonstrate eosinophilia when there is hyperinfection?
|
No
|
|
|
Where is Strongyloides found?
|
Worldwide, similar to hookworm.
|
|
|
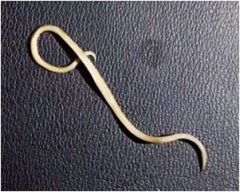
Strongyloides
|
|

|
Strongyloides
|
|
|
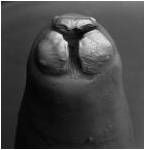
Left = strongyloides (forked tail)
Right = hookworm (pointed tail) |
|

|
Strongyloides
|
|
|
What is the life cycle of Paracapillaria philippinensis?
|
Unembryonated eggs are passed in stool of birds or humans --> Mature and become embryonated in environment --> Eggs ingested by freshwater fish --> Larvae hatch and penetrate the intestine --> Migrate into tissue --> Humans ingest undercooked fish --> Adult worms reside in human small intestine, where the burrow into the mucosa --> Deposit unembryonated eggs
Note: Some unembryonated eggs and hatch in the intestines and autoinfect! This leads to hyperinfection. |
|
|
What is the definitive host of Paracapillaria philippinensis?
|
Fish (humans from eating undercooked fish)
|
|
|
What are the clinical manifestations of Paracapillaria philippinensis?
|
Often asymptomatic. Over time develop borborygmus (excessive bowel sounds), abdominal pain, and watery diarrhea. If not treated over weeks to months get a large electrolyte losses and dehydration due to diarrhea, which can lead to death.
|
|
|
How do you diagnose Paracapillaria philippinensis?
|
Stool O/P (eggs appear similar to Trichuris)
|
|
|
How do you treat Paracapillaria philippinensis?
|
10 day course of albendazole and supportive care.
|
|
|
Where is Paracapillaria philippinensis found?
|
Primarily SE Asia
|
|
|
What worm has the common name "Pinworm?"
|
Enterobius vermicularis
|
|
|
What is the life cycle of Pinworms?
|
Humans ingest infective eggs by scratching their perianal area or by handling contaminated cloths/bed linens --> Hatch in small intestine --> Adults live in cecum --> Gravid females migrate to perianal folds at night to lay eggs --> Larvae inside mature in 4-6 hours and eggs become infective again
Note: Retroinfection is possible (newly hatched larvae from anal skin crawl back into rectum). |
|
|
What is the definitive host of Enterobius vermicularis?
|
Humans
|
|
|
What is the morphology of Pinworms?
|
Females have characteristic bulb and are 8-13mm.
Males have curled tail and are 2-5mm. Both have oxyurid esophagus. |
|
|
What is the morphology of Enterobius vermicularis eggs?
|
Elongate with one side that is flattened and the other curved. Thick colorless shell. 50-60um long.
|
|
|
What are the clinical manifestations of Pinworms?
|
Asymptomatic or perianal itching.
|
|
|
How do you diagnose Pinworms?
|
Stool O/P is not helpful (eggs rarely come out in stool).
In the early AM before defecating do a "scotch tape" test. |
|
|
How do you treat Enterobius vermicularis?
|
Albendazole 100mg for <1yo or 400mg single dose, mebendazole 100mg single dose, pyrantel pamoate 11mg/kg single dose, ivermectin 0.2mg/kg single dose (not FDA approved)
Repeat Rx in two weeks. Treat all members of household and make sure they are handwashing + washing linens. |
|
|
What is the epidemiology of Pinworms?
|
Most prevalent in children
|
|
|
Where are Pinworms found?
|
Worldwide
|
|

|
Female pinworm (has characteristic bulb)
|
|

|
Adult pinworm
|
|
|
Female pinworm (characteristic bulb)
|
|

|
Male pinworm (curled tail)
|
|

|
Pinworm egg
|
|

|
Pinworm eggs
|
|
|
Describe the Taenia solium life cycle.
|
Embryonated eggs or gravid proglottids in feces are eaten by pigs --> Oncospheres hatch, penetrate intestinal wall, and circulate to muscles --> Develop into cysticerci in muscles --> Humans ingest undercooked meat infected with cysticerci --> Scolex attaches to intestine --> Adult matures in the intestine --> pass eggs or gravid proglottids in feces
|
|
|
What is cysticercosis?
|
If humans ingest eggs of T. solium, then they can migrate to places, form cysticerci, and cause damage.
|
|
|
What is the definitive host of Taenia solium?
|
Humans
|
|
|
What is the intermediate host of Taenia solium?
|
Pigs
|
|
|
What is the morphology of Taenia solium?
|
2-7m in length. Have 4 suckers which anchor scolex. Rostellum in the middle of suckers has 6 hooks (referred to as "armed"). Head is 1-2mm in diameter and Strobila has ~1000 proglottids.
|
|
|
What is the morphology of Taenia solium eggs?
|
Spherical and yellow-brown in color. Thick shell with radial striations. 30-35um long. Contains a 6 hooked embryo.
|
|
|
What are the clinical manifestations of Taenia solium?
|
Frequently asymptomatic. Rarely appendicitis or cholangitis. Proglottids are sometimes mobile and crawl down thigh (producing tickling). May cause nutrient deficiencies if individual is already on verge of starvation.
|
|
|
How do you diagnose Taenia solium?
|
Eggs and proglottids in feces or antibody detection. Typically pass ~6 proglottids per day.
|
|
|
How do you diagnose Cysticercosis?
|
Demonstrate cysticercosi in tissue (can calcify and appear on plain film). Ab detection also works.
|
|
|
How do you treat Taenia solium?
|
Praziquantel 5-10mg/kg PO single dose; Niclosamide 2g PO single dose
|
|
|
Where is Taenia solium found?
|
Worldwide, but especially in Latin America, Iberian peninsula, slavic countries, SE Asia, Africa, India, and China.
|
|

|
Taenia solium (note hooks)
|
|
|
Proglottid of Taenia solium (fewer primary lateral uterine branches than saginata)
|
|

|
Egg of Taenia solium or saginata (you can't tell the difference between their eggs)
|
|

|
Egg of Taenia solium or saginata (you can't tell the difference between their eggs)
|
|
|
Describe the life cycle of Taenia saginata.
|
Same as T. solium (except it uses cattle instead of pigs)
|
|
|
What is the definitive host of Taenia saginata?
|
Humans
|
|
|
What is the intermediate host of Taenia saginata?
|
Cattle
|
|
|
What is the morphology of Taenia saginata?
|
Comparible to T. solium, except it has no rostellum or hooks and proglottids have more primary lateral uterine branches.
|
|
|
What is the morphology of Taenia saginata eggs?
|
Identical to T. solium (characteristic radial striations)
|
|
|
Which worm causes cysticercosis?
|
Only T. solium. T. saginata does NOT cause cysticercosis.
|
|
|
How do you diagnose T. saginata?
|
Eggs and proglottids in feces; Ab detection
|
|
|
What are the clinical manifestations of cysticersosis?
|
Symptoms depend on where cysticerci are formed.
Neuro: SOL, seizures, death Ocular, spinal, cardiac lesions Subcutaneous nodules |
|
|
How do you treat cysticercosis?
|
Anti-seizure meds, steroids, albdendazole 400mg PO bid x 30 days, praziquantel 100mg/kg for 1st day and 50mg/kg for 29 days
Surgical intervention if obstructive hydrocephalus |
|

|
Adult T. saginata
|
|

|
Proglottid of T. saginata
|
|
|
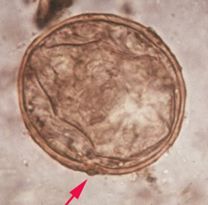
Describe the life cycle of Echinococcus granulosus.
|
Intermediate host eats feces with embryonated eggs --> Oncosphere hatches and bores through intestines --> Forms hydatid cyst in tissue (usually liver/lungs) --> Cysts give off protoscolices
Definitive host can eat tissue with cysts --> Poop out more eggs from adult worms in intestines |
|
|
What is the definitive host of Echinococcus granulosus?
|
Dogs
|
|
|
What is the intermediate host of Echinococcus granulosus?
|
Sheep, humuans
|
|
|
What is the morphology of Echinococcus granulosus?
|
5mm head and only has several proglottids. Has 4 suckers and a rostellum with 6 hooks.
|
|
|
What are the clinical manifestations of Echinococcus granulosus?
|
Often silent for many years.
Abdominal pain, biliary duct obstruction, chest pain, cough, hemoptysis (coughing of blood). Rupture --> fever, urticaria, anaphylaxis Brain, heart, bone |
|
|
How do you diagnose Echinococcus granulosus?
|
Imaging techniques, fine needle aspirate, or Ab detection
|
|
|
How do you treat Echinococcus granulosus?
|
Surgery, Albendazole 400mg x 1-6months, PAIR
PAIR = Puncture, aspirate, introduce protoscolicide (hypertonic saline), re-aspirate |
|
|
Where is Echinococcus granulosus found?
|
Sheep and cattle raising countires (esp. Australia). Increasing # of cases in W. US.
|
|
|
Describe the life cycle of Echinococcus multilocularis.
|
Similar to E. granulosus, except that hydatid cysts can spread.
|
|
|
What is the definitive host of Echinococcus multilocularis?
|
Foxes
|
|
|
What is the intermediate host of Echinococcus multilocularis?
|
Various rodents or humans
|
|
|
How do you treat Echinococcus multilocularis?
|
Surgery, albendazole
|
|
|
Describe the life cycle of Hymenolepis diminuta.
|
Embryonated eggs are eaten by insects --> penetrate intestinal wall and form cysticerci --> humans/rats ingest infected insects --> larva grow into adult worms in intestines --> eggs in feces
|
|
|
What cestode can complete its life cycle without an intermediate host?
|
Hymenolepis diminuta
|
|
|
What is the definitive host of Hymenolepis diminuta?
|
Rat intestines
|
|
|
What is the intermediate host of Hymenolepis diminuta?
|
Insects
|
|
|
What is the morphology of Hymenolepis diminuta eggs?
|
Space between inner and outer membrane is defining characteristic
|
|
|
What are the clinical manifestations of Hymenolepis diminuta?
|
Abdominal pain
|
|
|
How do you treat Hymenolepis diminuta?
|
Praziquantel 2mg/kg PO once
|
|
|
How do you diagnose Hymenolepis diminuta?
|
Eggs in feces
|
|
|
Hymenolepis diminuta egg (space between inner and outer membrane)
|
|
|
What cestode has the common name of "broad" or "fish tapeworm?"
|
Diphyllobothrium latum
|
|
|
Describe the life cycle of Diphyllobothrium latum.
|
Unembryonated eggs pass in feces into water --> hatch (embryonate) into ciliated coracidium embryos in water --> swim until ingested by crustaceans --> develop into procercoid larva in crustacean --> fish eats crustacean --> larva develop into plerocercoid larva --> humans eat undercooked fish --> plerocercoid larva develops into adult in small intestine --> proglottids release immature eggs
|
|
|
What is the definitive host of Diphyllobothrium latum?
|
Humans
|
|
|
What is the intermediate host of Diphyllobothrium latum?
|
Crustaceans (copepods), then fish
|
|
|
What is the morphology of Diphyllobothrium latum?
|
Proglottids are wider than long
|
|
|
Whatis the morphology of Diphyllobothrium latum eggs?
|
Inconspicuous knob on one side and operculum on the other
|
|
|
What are the clinical manifestations of Diphyllobothrium latum?
|
Can be asymptomatic.
Abdominal pain, vomiting, diarrhea, weight loss Intestinal obstruction Competes for B12 --> pernicious anemia |
|
|
How do you diagnose Diphyllobothrium latum?
|
Eggs in feces, chain of proglottids in feces
Rosette-shaped uterus in proglottids |
|
|
How do you treat Diphyllobothrium latum?
|
Praziquantel 5-10mg/kg single dose
Niclosamide 2g single dose |
|
|
Diphyllobothrium latum egg
|
|

|
Diphyllobothrium latum egg
|
|
|
What are the major Schistosomes?
|
S. mansoni, S. haemotabium, and S. japonicum
|
|
|
What Schistosomes have a restricted range?
|
S. intercalatum, S. guineensis, and S. makongi
|
|
|
Describe the Schistosome life cycle.
|
Eggs from stool pass from feces into water --> hatch, releasing miracidia larva --> miracidia penetrate snail tissue --> become sporocysts in snail (successive generations) --> snail releases free swimming cercariae into water --> penetrate human skin --> travel through circulation to portal circulation and mature into adults --> paired adult worms migrate to mesenteric venules of bowels/rectum or venous plexus of bladder --> lay eggs that circulate to liver and shed in stool
|
|
|
What is the definitive hosts of Schistosomes?
|
Humans
|
|
|
What is the intermediate hosts of Schistomomes?
|
Snails
S. mansoni --> biomphilaria S. haemotabium --> bulinus S. japonicum --> oncomelania |
|
|
What is the morphology of Schistosomes?
|
Males are shorter, more robust, and form gynecophoral canal.
Females are longer and more slender. |
|
|
What is the morphology of Schistosome eggs?
|
S. mansoni is long, nonoperculate, and has prominent lateral spine.
S. haematobum long, nonoperculate, and has prominent terminal spine. S. japonicum is round, nonoperculate, and has a nonprominent spine (nub) |
|
|
What is the morphology of Schistosome cercariae?
|
Short head with a longer forked tail
|
|
|
What is the morphology of Schistosome miracidia
|
Surface is coated with a dense cilia
|
|
|
What are the clinical manifestations of acute Schistosomiasis?
|
Symptoms occur w/ onset of egg laying (4-6 weeks post exposure) in patients from non-endemic areas.
Caused by S. mansoni and S. japonicum. Symptoms: fever, seats, chills, cough, headaches, diarrhea, RUQ pain Findings: Lymphadenopathy, hepatosplenomegaly, eosinophilia, may be negative for eggs on fecal exam |
|
|
What are the types of chronic Schistosomiasis?
|
Intestinal (S. mansoni and S. japonicum) and urinary (S. haematobium)
|
|
|
What are the clinical manifestations of chronic intestinal Schistosomiasis?
|
Symptoms: fatigue, bloody diarrhea, RUQ pain, cramps
Findings: hepatosplenomegaly, periportal fibrosis, portal hypertension, portosystemic shunts, intestinal polyps, iron deficiency anemia, hepatocellular function often normal |
|
|
What causes "Pipe Stem fibrosis?"
|
S. mansoni or S. japonicum
|
|
|
What are the clinical manifestations of chronic urinary Schistosomiasis?
|
Symptoms: hematuria and dysuria
Findings: hydroureter, hydronephrosis, repeated bacterial infections, renal failure, and associated with squamous cell carcinoma |
|
|
How do you diagnose Schistosomiasis?
|
Demonstration of eggs in urine or feces with Kato-Katz method; may need to be repeated; quantitative (light = 1-100 eggs/gram feces, moderate = 100-400, heavy = <400)
Concentration techniques helpful Other dx methods: Abs in peripheral blood, urine dipstick for parasite Ag, demonstration of schistosome Ags and DNA in peripheral blood (experimental) |
|
|
How do you treat Schistosomiasis?
|
Praziquantel 40mg/kg single dose or 30mg/kg 2x is 85% curative
Oxamniquine for S. mansoni only (drug resistance occurs) Metrifonate for S. haematobium (withdrawn) Artemesinin derivates (antimalarial, effective against immature stages) |
|
|
What is the epidemiology of Schistosomes?
|
Disease is limited to water source. A disease of young children and young adults, though intensity of disease is highest in the young.
|
|
|
What is the prevalence of Schistosomes?
|
>200 million worldwide are infected
|
|
|
Where are Schistosomes found?
|
S. mansoni: Africa, Middle East, S. America
S. haematobium: Africa, Middle East S. japonicum: East Asia S. intercalatum: West Africa S. guineensis: West Africa S. mekongi: Laos, Cambodia, Thailand |
|

|
Schistosome cercariae
|
|
|
S. japonicum egg
|
|

|
S. haematobium egg
|
|

|
S. mansoni egg
|
|

|
Schistosome miracidium (note dense coat of cilia)
|
|
|
What is the mechanism of action of Albendazole?
|
Inhibits glucose uptake and specifically binds tubulin. This inhibits microtubule assembly. Worms are immobilized and die slowly.
|
|
|
What trematodes have the common name "liver flukes," "lung flukes," and "intestinal flukes?"
|
Liver flukes = Clonorchis, Opisthorchis, and Fasciola
Lung fluke = Paragonimus Intestinal fluke = Fasciolipsis |
|
|
What two trematodes share the same disease profile?
|
Clonorchis and Opisthorchis
|
|
|
Describe the life cycle of Clonorchis/Opisthorchis.
|
Embryonated eggs passed in feces --> Snail eats eggs --> embryo transforms inside of snail from Miracidia --> Sporocysts --> Rediae --> Cercariae --> Sheds free-swimming Cercariae --> Eaten by fish --> develops into metacercariae (infectious stage for humans) --> Humans eat undercooked fish --> Goes through sphinctor of Oddi to reach biliary duct --> Adults lay eggs in feces
|
|
|
What is the definitive host for Clonorchis/Opisthorchis?
|
Humans
|
|
|
What are the intermediate hosts for Clonorchis/Opisthorchis?
|
Snails, then fish
|
|
|
What are the 3 types of liver flukes we care about?
|
C. sinensis = Chinese liver fluke
O. viverrini = SE Asian liver fluke O. felineus = Cat liver fluke |
|
|
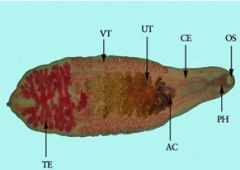
What is the morphology of adult Clonorchis/Opisthorchis?
|
~7mm in length. Have oral and ventral sucker. Test in posterior, uterus in middle. O. viverrini and O. felineus are lance shaped.
|
|
|
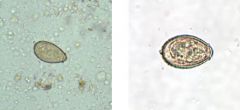
What is the morphology of Clonorchis/Opisthorchis eggs?
|
You can't distinguish between the two (though Oposthorchis are slightly smaller).
Operculate on one end, have prominent opercular "shoulders," have knob on the other end, and are embryonated. |
|
|
What are the clinical manifestations of Clonorchis/Opisthorchis?
|
Acutely: rarely reported. Fever, fatigue, abdominal pain, enlarged liver, eosinophilia, eggs in stool after 3-4 weeks
Chronic: asymptomatic unless heavy load. Fatigue, abdominal pain, dyspepsia, hepatomegaly. Chronic irritation can also lead to bile duct proliferation and squamous metaplasia. This makes it easier to get infected, which can cause recurrent ascending cholangitis/pancreatitis. These infections can cause gram - sepsis. Cholangiocarcinoma is also possible. |
|
|
How do you diagnose Clonorchis/Opisthorchis?
|
Eggs in stool; recover flukes after treatment to differentiate between the two.
Ultrasound shows cytic or "mulberry-like" dilation of intrahepatic bile ducts. |
|
|
How do you treat Clonorchis/Opisthorchis?
|
Praziquantel 75mg in 3 doses x 2 days
Albendazole 10mg/kg/d x 7 days |
|
|
What family of fish serve as a common intermediate host for Clonorchis?
|
Cyprinidae (Carp family)
|
|
|
Where are Clonorchis/Opisthorchis usually found?
|
SE Asia
|
|
|
Describe the Fasciola life cycle.
|
Unembryonated eggs pass in feces into water --> Embryonate in water --> Miracidia hatch and infect snail --> Inside snail mature into Sporocysts --> Rediae --> Cercariae --> Shed free swimming cercariae --> Metacercariae attach on water plant --> Plant ingested by humans --> Migrates via peritoneal cavity and liver parenchyma to get the bile duct --> Adult in hepatic biliary duct give off eggs
|
|
|
What is a common source of Fasciola metacercariae for humans?
|
Watercress
|
|
|
What is the morphology of adult Fasciola?
|
Looks like a leaf.
|
|
|
What two species of Fasciola do we care about?
|
F. hepatica and F. gigantica
|
|
|
What is the definitive host of Fasciola?
|
Humans, domestic animals like cattle or sheep
|
|
|
What is the intermediate host of Fasciola?
|
Snails
|
|
|
What is the morphology of Fasciola eggs?
|
Broadly ellipsoidal, large, operculated on one end.
You cannot distinguish between Fasciola and Fasciolopsis eggs. |
|
|
What are the clinical manifestations of Fasciola?
|
Acute hepatic (invasive): 6-12 weeks post ingestion of metacercariae, lasts 2-4 months. Eosinophilia, abdominal pain, intermittent fever, malaise, weight loss
Chronic Biliary (obstructive): intermittent biliary obstruction, intermittent abdominal pain, ascending cholangitis, jaundice, lithiasis |
|
|
How do you diagnose Fasciola?
|
Eggs in stool (after 3-4 months), Ab detection, CT/ultrasound
|
|
|
What is false fascioliasis?
|
Ingestion of infected bovine or ovine liver with eggs will cause eggs to pass into human feces. This gives a positive test for Fasciola infection, despite it not being present.
Note: also called pseudofascioliasis |
|
|
How do you treat Fasciola?
|
Triclabendazole 10mg/kg once or twice
Bithionol 30-50mg on alternate days x 10-15 doses Nitazoxanide 500mg x 7 days Note: Praziquantel is NOT effective |
|
|
Where is Fasciola found?
|
F. hepatica is found worldwide, even N. America
F. gigantica is mostly in sub-Saharan Africa and India |
|
|
Describe the Paragonimus life cycle.
|
Unembryonated eggs in water --> Embryonate in water --> Miracidia hatches and infects snail --> Inside snail matures to Sporocysts --> Rediae --> Cercariae --> Cercariae infect freshwater crustaceans --> matures into metacercariae --> Humans ingest undercooked/pickled crustaceans --> Migrates via gut wall, peritoneum, diaphragm, pleural cavity, to lung parenchyma --> Adults in cystic cavities in lungs lay eggs which are coughed out in sputum or swallowed
|
|
|
What is the definitive host of Paragonimus?
|
Humans
|
|
|
What is the intermediate host of Paragonimus?
|
Snail, then crustaceans
|
|
|
What is the morphology of Paragonimus?
|
Reddish brown color, coffee bean-shaped
2-3 flukes enclosed in fibrotic cyst Eggs escape through cyst-bronchial fistula |
|
|
What is the morphology of Paragonimus eggs?
|
Yellow-brown, ovoid or elongate, thick shell.
Asymmetrical, one end is flattened and the other end is pointed. Operculum at large end. Abopercular end thickened. |
|
|
What are the clinical manifestations of Paragonimus?
|
Acute: young migrating worms may cause diarrhea, pain, eosinophilia. If entering the lungs they can cause fever, chills, chest pain.
Chronic: Productive cough (rusty flecks due to eggs), hemoptysis, pleural lesions (fluid, thickening), diffuse/segmental/or patchy infiltrates. Xray may resemble TB Extrapulmonary: rare. Can go to cerebral, cutaneous, etc. |
|
|
How do you diagnose Paragonimus?
|
Eggs in sputum or feces (after 2-3 months), biopsy, or Ab detection
|
|
|
How do you treat Paragonimus?
|
Praziquantel 75mg/kg/d in 3 doses x 2 days
Bithionol 30-50mg on alternate days x 10-15 doses |
|
|
Where is Paragonimus found?
|
China, India, and Japan (where crustaceans don't get cooked)
|
|
|
Describe the life cycle of Fasciolopsis buski.
|
Unembryonated eggs in water --> Embryonate in water and Miracidia hatches --> Penetrates snail --> matures inside snail into sporocysts --> rediae --> cercariae, which snail sheds --> gets on water plant and matures into metacercariae --> human or pig eats plant --> matures in small intestine
|
|
|
What is the definite host of Fasciolopsis buski?
|
Humans, pigs
|
|
|
What is the intermediate host of Fasciolopsis buski?
|
Snail
|
|
|
What is the morphology of Fasciolopsis buski?
|
Largest of the flukes (up to 8cm long).
|
|
|
What is the morphology of Fasciolopsis eggs?
|
Exact same appearance as Fasciola eggs.
|
|
|
What are the clinical manifestations of Fasciolopsis buski?
|
Fluke attaches to intestine and causes focal inflammation, ulceration, and abscesses.
Epigastric pain, diarrhea, intermittent obstruction |
|
|
How do you treat Fasciolopsis buski?
|
Praziquantel 75mg/kg/d in 3 doses x 1 day
|
|
|
What is a common source of Fasciolopsis buski metacercariae for humans?
|
Water Chestnut (particularly in China)
|
|
|
Where is Fasciolopsis buski found?
|
SE Asia
|
|

|
Adult Fasciolopsis buski
|
|

|
Adult Fasciolopsis buski
|
|

|
Fasciolopsis buski eggs
Cannot distinguish for Fasciola eggs |
|
|
Clonorchis sinensis (Chinese liver fluke)
|
|
|
Clonorchis eggs
|
|

|
Fasciola adult
|
|

|
Fasciola hepatica
|
|

|
Fasciolopsis buski
|
|
|
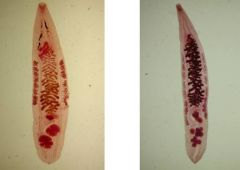
O. felineus left
O. viverrini right |
|

|
Opisthorchis eggs
|
|

|
Opisthorchis viverrini (SE Asian liver fluke)
|
|
|
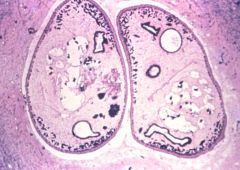
Two Paragonimus inside a fibrotic cyst
|
|

|
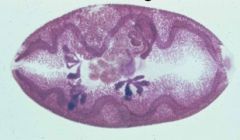
Paragonimus eggs
|
|

|
Paragonimus eggs
|
|
|
Paragonimus westermani
|