![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
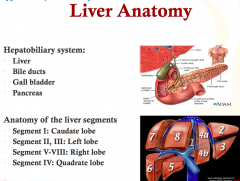
Hepatobiliary system
Anatomy of Liver Segments |
|
|
|
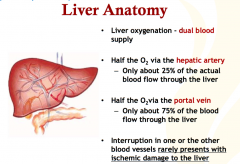
Liver Blood Supply What happens if 1 vessel is interrupted? |
|
|
|
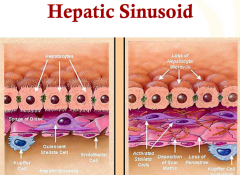
Hepatic Sinusoids (normal and abnormal) |
|
|
|
Liver Function |
|
|
|
Histological Pattern of Liver Injury can Indicate what conditions? |

|
|
|
Purpose of Liver tests, liver function tests, pattern of Liver injury. Do they lead to a diagnosis? |
|
|
|
Liver Chemistry Panel (Liver Tests, Liver Function tests) What indicates |
ALT AST are associated with hepatocellular disease ALT- specific for liver diseases AST- skeletal muscle, brain and heart tissue (less specific) |
|
|
What is bilirubin and how is it excreted? Direct vsIndirect Bilirubin? High levels of water soluble bilirubin can cause what characteristic? |
|
|
|
What are patterns of injury? Be specific? What can labs assess synthetic function of the liver? |
Synthetic function test can be abnormal for many reasons ie nephrotic syndrome, hemolytic amenia |
|
|
What is cholestasis? What are the two types? What does it indicate? |
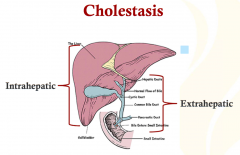
problems within the level, cellular level (intrahepatic) obstruction of ducts (extrahepatic) |
|
|
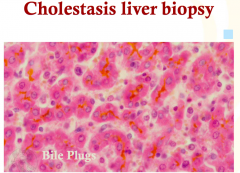
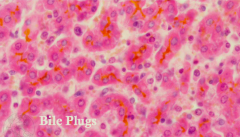
bile plugs, rust colored, cholestic |
|
|
How does AST, ALT, ALP, GGT, Bilirubin, and Protime relate to Hepatocellular an Cholestasis Injury? |
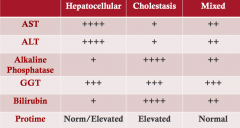
Pro time decreased: absorption preserved by hepatocyte mass is lost (Hepatocellular injury) Pro time Increase: fat soluble dep factors 2, 7, 9, and 10 cannot be absorbed (cant absorb vitamins (cholestasis) |
|
|
What is the Sx and Ddx of Cholestasis? |
Ace Inhibitors |
|
|
What is the Sx and Ddx of Hepatocellular Injury? |
|
|
|
List the Viral Hepatitis Which are DNA and RNA viruses? |
|
|
|
Hepatitis A: Mode of Transmission, Natural History, Cause of Outbreaks When is it Serious? |
|
|
|
Hepatitis A:Mode of Transmission, Natural History, Cause of Outbreaks When is it Serious? |
|
|
|
Hepatitis A:Mode of Transmission, Natural History, Cause of Outbreaks When is it Serious? |
|
|
|
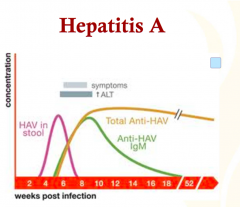
Hepatitis A: Markers of Acute infection and Disease resolution Clinical Scenarios, Treatment , and Prevention |
|
|
|
Hepatitis B: Wha is it? Symptoms? Risk of Transmission? |
|
|
|
Hepatitis B: Acute vs ironic Significance of Vertical Transmission |
|
|
|
Hepatitis B Serologic Profile |
|
|
|
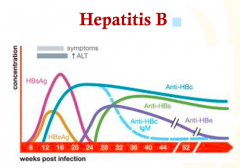
Hepatitis B: Serology Graphical |
|
|
|
Hepatitis B: Hepatitis Surface Antigen |
|
|
|
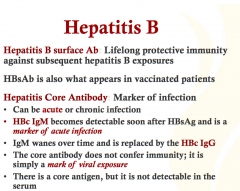
Hepatitis B: Hepatitis B Surface Antibody vs Hepatitis Core Antibody |
|
|
|
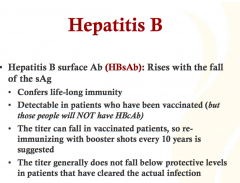
Hepatitis B: Hepatitis B Surface Antibody |
|
|
|
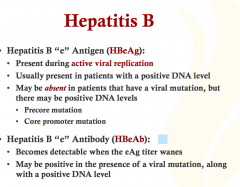
Hepatitis B: Hepatitis B e Antigen |
|
|
|
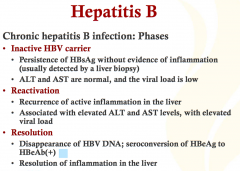
Hepatitis B: Phases of Chronic Hepatitis B |
|
|
|
Hepatitis B: DNA level measured correlates to what? |
|
|
|
Hepatitis B: Chronic Hepatitis B General Treatment, Complicaiotns, Seroconversions, |
|
|
|
Hepatitis B: Specific Treatment for Chronic Hepatitis and Complications |
|
|
|
Hepatitis C (Etiology) |
|
|
|
Hepatitis C: How often to patients get this and can it clear? Acute or Chronic? |
|
|
|
Hepatitis C: Risk of Transmission (main difference) |
|
|
|
Hepatitis C: Genotypes and why are they significant? |

|
|
|
Hepatitis C: Acute Hepatitis ClinicalManifestation and Labs |
|
|
|
Hepatitis C: Goal of Treatment and What is used to Treat is? |
|
|
|
Hepatitis C: What is Combination Therapy? |
|
|
|
Hepatitis D: What is it Risk Factors, Clinical Manifestation |
|
|
|
Hepatitis D: Diagnosis and Serology |
|
|
|
Hepatitis E |
|
|
|
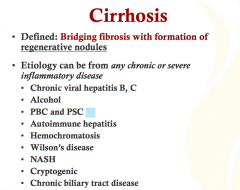
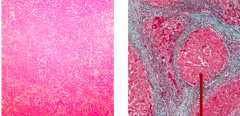
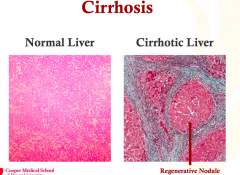
What is Cirrhosis and the etiology? |
|
|
|
|
|
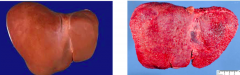
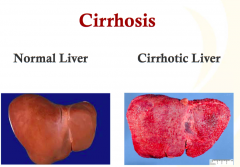
Identify the normal and abnormal liver. |
|
|
|
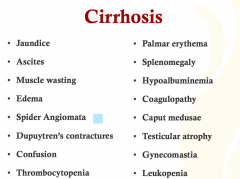
Cirrhosis: Clinical Presentation |
|
|
|
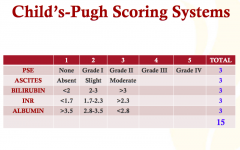
Scoring System for Cirrhosis: Child Pugh |
|
|
|
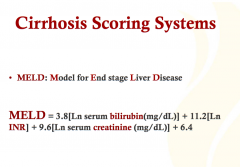
Scoring System for Cirrhosis: MELD |
|
|
|
Compensated vs Decompensated Cirrhosis |
|
|
|
Decompensating Events in Cirrhosis |
|
|
|
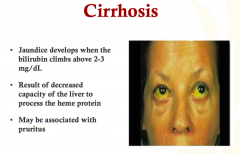
In cirrhosis, what might develop due to high bilirubin levels? Why does this occur? |
|
|
|
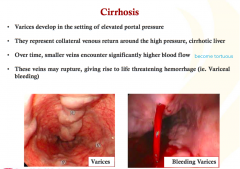
How can cirrhosis affect veins? |
|
|
|
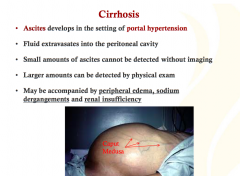
Cirrhosis can lead to what conditions in the setting of portal hypertension ? |
|
|
|
Treatment of Cirrhosis |
|
|
|
What is GGT? |
sensitive but not specific Used when alkaline phsopahtase is highbone, intestinal tract o biliary tree normal GGT suggests it is not coming from the biliary tree (require an alternative diagnosis) elevated GGT suggests it is coming from the biliary tree (cholestatic process) |