Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back
- 3rd side (hint)
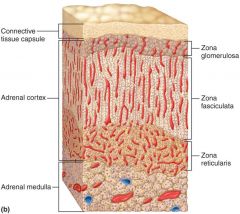
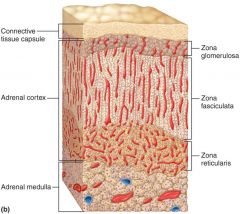
Adrenal Glands: adrenal cortex and medulla
|
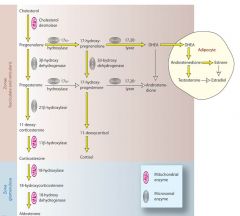
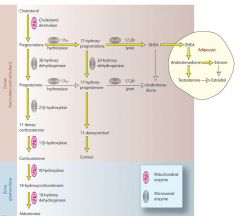
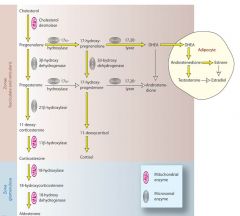
Cortex zones: -- Zona GLOmerulosa – Aldosterone (mineralcorticoids) -- Zone FASciculata – cortisol and corticosterone (glucocorticoids) -- Zona (S)TETicularis – Androgens and Estradiol (sex steroids)
|
|
|
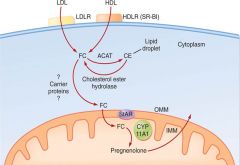
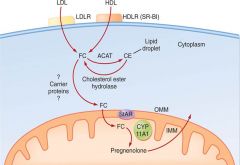
Andrenal Hormone synthesis –
|
use Cholesterol as the precursor --> uptake of cholesterol is the Rate limiting step in synthesis – L/HDLR - FC - StAR (mito) - CYP 11A1 --> Pregnenolone (prohormone) --- ACTH (corticotropin) helps turn on LDLRec
|
|
|
|
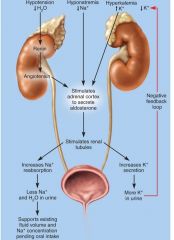
Aldosterone (Mineralocorticoids -Na/K) – Zona GLOmerulosa
|
Aldosterone – helps maintain blood pressure and volume: 1) Hypotension (Renin-Angiotensin) 2) Hyponatrimia 3) Hyperkalemia (Na/K ratio) ->
|
|
|
|
Androgens (testo-DHE) – Zona Reticularis Sex Steroids Male
|
Androgens – control aspects of male development and reproductive physiology, bone growth --1) DHEA and 2) Androstenedione
|
|
|
|
1) DHEA
|
fetal male development --2nd sex chac - drive (little effect) --> Converted to testosterone/estrogen in many tissues – to increase effectiveness
|
|
|
|
Use of Anabolic steroids
|
Synthetic steroids stimulate same mechanism as endogenous --- Block the actions of glucocorticoids --- Long term abuse leads to liver damage, hypertension, testicular shrinkage and breast growth --- Clinical uses: delayed puberty, muscle loss due to disease, hormone deficits in men
|
|
|
|
2) Androstenedione
|
(less and weaker effects) – converted to testosterone
|
|
|
|
Androgens – Zona Reticularis Sex Steroids Female
|
Estradiol – minor compared to reproductive estrogen (follicle), after menopause becomes more important
|
|
|
Congenital andrenal hyperplasia
|
Mutation cause enz deficiencies --- high ACTH (Ant -Pit) no (Aldosterone-Cortisol-Androgen) to neg fb ---> Low Na (Dehydration/ weird HR) -- Puberty early -- large clitoris-penis
|
|
|
|
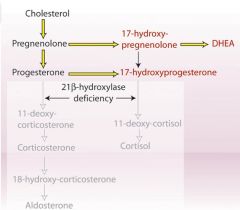
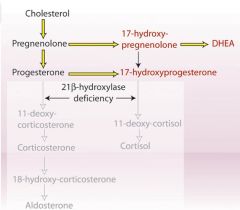
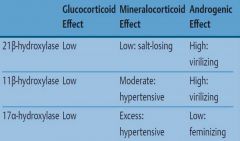
21b-hydroxylase
|
no Aldosterone --> salt losing - dehydration/ HR ----- high DHEA --> virilization (masculinization) female wt male sex organ
|
|
|
|
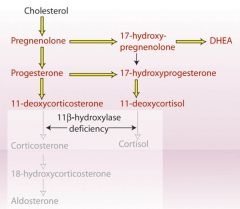
11a-hydroxylase
|
intermediate mimic aldosteron ---> moderate hypertensive --- high DHEA --> virilization (masculinization) female wt male sex organ
|
|
|
|
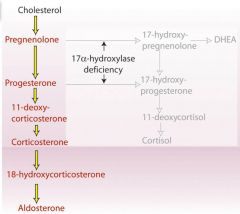
17 b-hydroxylase
|
a lot of Aldosterone ---> EXcessive hypertension ---- no DHEA --> feminizing
|
|
|
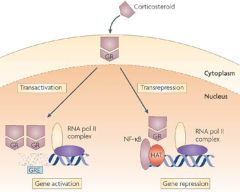
Glucocorticoids -type 1 - lipophilic -
|
Transport: corticosteroid-binding globulin (CBG) - transcortin) -- Long half-life -- Binds to intracellular GC receptors to activation (GRE) or repression (HAT) gene expression ----- Conjugated to glucuronic acid (in liver) –> excreted in bile or via kidneys
|
|
|
|
Corticol synthesis
|
High ACTH (Ant-Pit) --> Pro-opion-melano-cortin (POMC) broken into 3 other hormones --> Melanocyte Sti Horm (MSH-ez to sleep) ---be-lipotropin (break fat to make cortisol - steroid remember) -- be-endorphin (feel good)
|
|
|
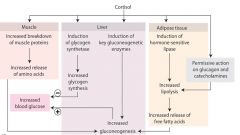
Cortisol Physiological Effects: make sugar (inc glucose plasma)
|
Anti-inflam (im-suppress) -- Inc growth adrenal medulla (Epi-Nor: sympa - gluconeogenesis) -- No sex hormone -- Break down muscle - fat - glycogen - more Glucagon
|
|
|
|
Cortisol level is high in .....
|
day time and stress time (injury-exer-infect-anger-grief-hermorrhage-loose blood)
|
|
|
|
Cortisol response stages ---- should NOT last long: Brain can't use Ketone (after Glc gone) -- fat break down and not used --> move to other areas -- Edema
|
1) Alarm: Epi-Norepi (Glycogen → glucose, inc BP) ----- 2)
Resistance: Glycogen gone --> Cortisol HIGH (break muscle-fat for glc) --- REduce Immu - inflam -- 3) Exhaustion: Fats gone ---> no more glucocorticoids |
|
|
|
Hypersecretion of cortisol: Cushing’s Syndrome
|
Hypotha HIGH - ↑ CRH (F) ---- Adenomas (Ant-Pit cancer) - ↑ ACTH -- Ectopic ACTH (other ACTH cancer: lung) ---- Adenomas (And-Cort) ---- Exogenous use of corticosteroids (over use Prednisone topical)
|
|
|
|
Cushing’s SynpTOMs
|
Buffalo Torso (fats move to chest) --- Moon face, acne, facial hair (Excess steroids) --- Hypertension (excess Aldosterone) --- Osteoporosis -- Muscular weakness (break for Glc) --- Prone to infection (dec lymphoid) ---
Dark skin (MSH - ACTH secreting tumor) --- Androgenital Syndrome (incr androgens-- enlarged genitals and increased masculinization) |
|
|
|
Diagnosing source of Cortisol: Dexa-methasone --- Treatment
|
Use High-dose dexamethosone to suppress ACTH (Ant-Pit) by neg fb ---> if not working --> Adenomas of And Cort (AD cancer) ----- Remove And Cort and HRT (Cortisone- Demamethosone-Prednisone)
|
|
|
|
Hyposecretion of cortisol: Addison’s disease
|
Autoimm Adrenal Cortex -- Tuberculosis destroys gland -- Cancer --- less ACTH (Ant Pit) --- Enzyme mutations (Inborn errors in metabolism)
|
|
|
|
Symptoms of Addison’s disease:
|
Hypo-natremia/kalemia/tension (less Aldosteron) -- Fasting hypoglycemia (less cortisol) --- Muscle weakness (no glc no ATP) -- Intolerance to “any stresses” (no beta endorphin, be-lipotropin, MSH, pos fb Epi-Nor, glucagon), ----- Melanin hyperpigmentation mucous membranes and thin skin areas due to excess ACTH (if disease due to adrenal deficit)
|
|
|
|
Diagnosis of hyposecretion - Primary (adrenal destruction) versus Secondary (hypo/pit):
|
Measure ACTH to determine primary or secondary --- ACTH stimulation test - Addison’s will have no increase in cortisol levels
|
|
|
|
Treatment of hyposecretion:
|
Immediate or death --- Adrenocorticoid administered daily --- Need to really avoid stress – infection, trauma, ect
|
|
|
|
Other uses of Corticosteroid -- Cortisol
|
Asthma (inflammation) ----- Poison Ivy (immsuppress) ----- Arthritis (immsupp)
|
|