Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
79 Cards in this Set
- Front
- Back
|
Referred Back Pain
|
AAA >4cm, Pancreatitis, Gastric/duodenal ulcer, endometriosis, Prostate CA, myeloma (primary CA and mets), kidney infection/pathology/stones, renal calculi
|
|
|
Intrinsic Back Pain
|
Trauma (fx, dislocation),
Pathology (compression fx d/t osteoporosis, spinal stenosis d/t osteoarthritis, ankylosing spondylitis- bone defect developed in adolescence, osteomyelitis), IVD pathology- disc protrusion/nerve root impediment, Postural/Structural Imbalances- overuse, misuse, occupational, recreational habits, scoliosis, spondylolisthesis, etc |
|
|
Back Pain in the Pt Exam
|
identify the causes that would require emergency intervention
observe and indentify pain patterns of potential DDx for back pain observe and identify appropriate clusters of s/s for potential ddx for back pain palpate and identify normal/abnormal structural anatomy observe and identify postural deviations |
|
|
Vertebral Column Structure
|

33 vertebrae
7 Cervical, 12 thoracic, 5 lumbar, 5 fused sacral, 4 fused coccyx |
|
|
Gross movement of Vertebral Column
|
general- F, E, LF, R
each region of the spine emphasizes and limits specific movements |
|
|
Functions of vertebral column
|
protect spinal column, support wt of head/trunk, allow movement of rib cage (costovertebral joints), critical role in posture/locamotion
|
|
|
Normal Curvatures of Vertebral Column
|
primary- T and S (kyphotic)
secondary- L and C (lordotic) function is to absorb shock (10x more than if straight spine) Birth- primary curve only, when infant starts to hold head and sit up cervical curve develops, when infant begins to stand/walk lumbar curve develops |
|
|
Kyphosis
|

excessive kyphosis in T spine (excessive posterior curve)
D/T comp fx, postural habits, Schuerman's disease or osteoporosis |
|
|
Lordosis
|

excessive lordosis in lumbar region (excessive anterior curve), d/t anomalies, postural habits, etc
clinical- important to assess ability to "reverse the lordotic curve" during flexion of the trunk |
|
|
Scoliosis
|
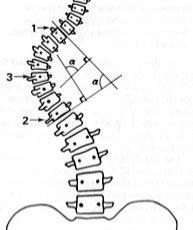
lateral deviation with rotary component (uneven ribs), curve named for convexity
school screenings to ID potential curves, progression and severity are key factors, depending on the above treatment ranges from observation, tx of sxs to bracing or surgical intervention |
|
|
Reversal of Cervical Curve
|
reduction of normal lordosis of C spine, d/t postural habits, MVA or other trauma, etc
|
|
|
Body of typical vertebrae-
T4 and below gradually increase in size to support increasing body weight ephyseal ring- smooth region of vertebrae along the periphery of the body, formed from annular epiphysis (2˚ ossification center during growth) shape of body varies in each region of the spine |
|
|
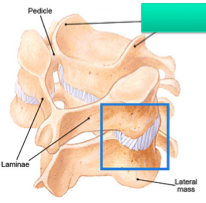
Vertebral (neural) arch= pedicles and lamina
clinically- spina bifida |
|

|
Spina bifida- lamina fail to fuse resulting in defect of arch,
spina bifida occulta- failure of vertebral arch to fuse, bony defect meningocele- meninges protrude through bony defect of vertebral arch meniomyelocele- spinal cord + meninges protrude defect of vertebral arch |
|
|
Transverse Process (2)-
project laterally from junction of pedicles and lamina attachement and lever for spinal mm |
|
|
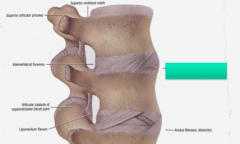
Articular Process (4)- superior and inferior processes
project from junction of pedicle and lamina adjacent articular processes from facet (zypgapophyseal) joints between vertebrae |
|
|
Spinous Process (1)-
project posteriorly from junction of R/L lamina attachment and lever for spinal mm |
|
|
Vertebral Notch- superior and inferior portion of pedicle
|
|

|
Intervertebral foramen
formed between vertebrae via the vertebral notches of two adjacent segments, superior and inferior vertebral notches |
|
|
formed by the body and vertebral arch
|
|
|
Vertebral Canal- vertebral foramina collectively form the canal
|
|
|
Cervical Vertebrae
|
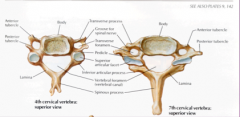
Cervical Vertebrae (typical C3-C7, smallest vetebrae)
Body- small, wider side to side than ant-post Vertebral foramen- LARGE, triangular TPs- have transverse foramen, allow vertebral artery to pass through (C6-1), C7 may have small or absent APs- superior facets face superior and posterior, inferior facets face inferior and anterior SPs- typically bifid C3-5, C7- most prominent, common landmark for palpation |
|
|
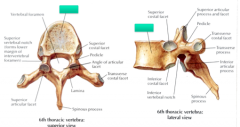
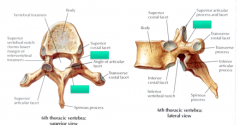
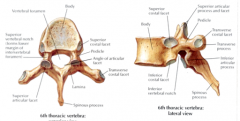
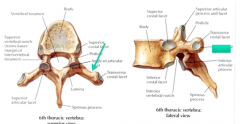
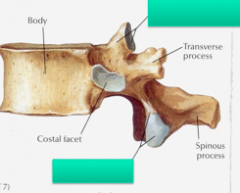
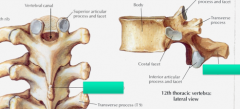
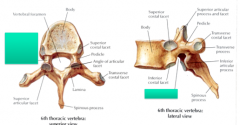
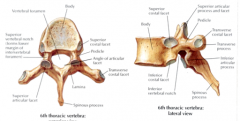
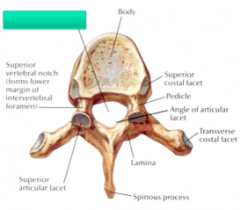
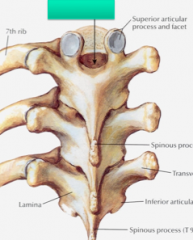
Thoracic Vertebrae
|
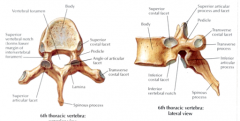
Body- heart shaped, costal facets
Vertebral foramen- circular and smaller than C and L TPs- long, T1-10 have facets for articulation with ribs (transverse costal facets) APs- superior facets face posterior and slightly lateral, inferior facets face anterior and slightly medial SPs- long and extend inferiorly to segment below General- upper Ts transition from C spine, mid Ts thoracic vertebrae characteristics, lower Ts begin to transition to L spine |
|
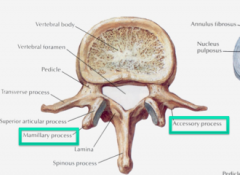
Lumbar Vertebrae
|
Body- kidney shaped
Vertebral Foramen- triangular, larger than T, smaller than C TPs- have accessory process- tubercles located at the base of TPs APs- superior facets face posterior and medial, inferior facets face anterior and lateral, have mamillary process- tubercles located on superior articular pillar SPs- sturdy, "hatchet shape" |
|
|
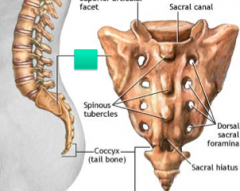
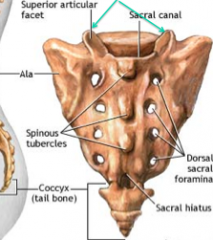
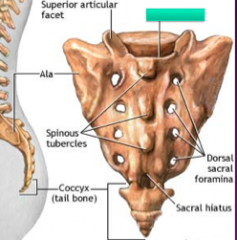
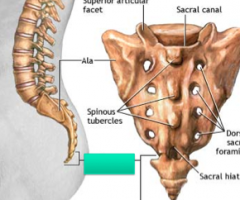
Sacrum
|
large triangular wedged shaped bone composed of 5 fused vertebrae, 4 pairs of foramina- exit for dorsal and ventral nerve roots, provides stability to pelvis
|
|
|
Promontory of Sacral Bone
|
prominent anterior edge of first vertebrae (segment)
|
|
|
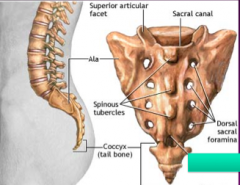
Ala of Sacral Bone
superior/lateral portion of sacrum (wings) |
|
|
Median Sacral Crest
|
midline formed by fused SPs
|
|
|
Sacral hiatus
formed by failure of the lamina of S5 to fuse |
|
|
Sacral cornu (horns) formed by pedicles of S5
|
|
|
Sacral Canal
contain nerve roots of cauda equina |
|
|
Apex of Sacrum
|
inferior end
|
|
|
Base
|
superior portion of S1
|
|
|
Coccyx- wedge shaped bone of 4 fused coccygeal vertebrae (provide attachement for pelvic mm)
|
|
|
Atlas (C1)
|

ring shaped, no spinous process or body
consists of anterior and posterior arches with TPs Anterior/posterior tubercles instead of spinous process Lateral mass- superior facets articulate with occipital condyles (flexion and extension motion), inferior facets articulate with C2 (superior facets for rotation) facet located on anterior arch- articulate with dens (odontoid process) TPs wide- palpate inferior to mastoid process Vertebral artery- forms large "loop" as it ascends to foramen magnum Front is smaller than back (to orient yourself) |
|
|
Axis (C2)
|

characterized by dens (odontoid process)
forms the "pivot" or axis for rotation between C1 and C2 Supported by multiple ligaments Everything else is normal |
|
|
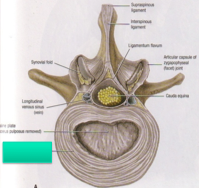
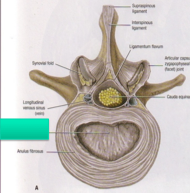
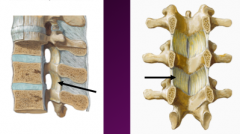
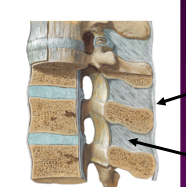
Intervertebral Disc
Annulus fibrosus + nucleus pulposus act as shock absorber, influences motion form the secondary cartilaginous joints between vertebral bodies composition- water, collagen fibers, proteoglycans approximately 1/4 of overal spine length no disc between occiput and C1, C1 and C2 Clinical- fissures develop (discogenic pain), protrusions/herniation (potential to compress nerve roots= radicular pain myatome or dermatome patterns), degenerative charges (loss of disc ht) |
|
|
Annulus Fibrosus- concentric layers composed of collagen fibers,
bundles if collegen fibers are obliquely oriented- provides tensile strength, direction of the fibers alternates for each layer- crosswoven effect, anchor disc to bone or cartilaginous end plate, outside layer will blend ALL and PLL and have innervation (can have pain) |
|
|
Nucleus pulposus
proteoglycans attract water to this portion of the disc gradual transition from annulus- not really a jelly donut as commonly referred to does contain collagen fibers- finer fibers, lose random network arrangement of fibers |
|
|
Uncovertebral (Joints of Luschka)
unique to cervical spine formed by uncinate processes of C3 and C7 considered more of a "pseudo joint" formed between the beveled uncinate processes of each vertebrae the joint looks similar to a synovial joint- cartilage and capsule research continues to debate if synovial jt or not clinically- prone to degenerative changes (bone spur formation) |
|

|
Facet (zygapophyseal) joints
plane synovial joints between superior and inferior facets of articular process surrounded by loose articular capsule permit gliding movement between vertebrae orientation varies in each region- will both enhance and limit movement depending on motion some wt bearing function in C and L regions innervation- dorsal primary rami of individual segment and segment above and below clinical- also prone to degenerative changes (result= limited movement and pain), excessive bone spurs can cause stenosis of invertebral foramen |
|

|
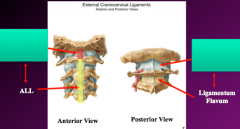
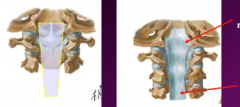
Anterior Longitudinal Ligament (ALL)
runs from occiput to the sacrum along anterior portion of vertebral column width increases as it descends down the vertebral column function- limit extension, support anterior annulus fibrosis of disc |
|

|
Posterior Longitudinal Ligament (PLL)- C2 to sacrum
runs along posterior vertebral column within vertebral canal (thus anterior to spinal column) along vertebral body width decreases as it descends down the vertebral column, narrow and much less substantial as compared to ALL function- limits flexion, supports posterior annulus fibrosis of disc |
|
|
Ligamentum Flavum
connects the lamina between each vertebrae, forms part of the posterior wall of vertebral canal gradually thicken as descend from C to L regions high elastin content function- allow smooth flexion of vetebrae and thus reduce potential for IVD injury, elasticity assists with restoring neutral position after flexion of spine |
|
|
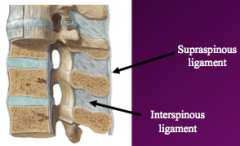
Interspinous ligaments (thin membranous ligament)- connect adjacent spinous processes, attach along inferior and superior position of SP
Supraspinous ligaments (cord like ligament)- connect adjacent spinous processess, attachement of apices of each SP, C7-sacrum, merges superiorly with nuchal ligament |
|
|
Nuchal Ligament (ligamentum nuchae)
EOP to C7, connects the EOP, posterior tubercle of C1 and SPs of C2-7, acts as septum separating muscles of R/L posterior neck |
|
|
Intratransverse Ligaments
|
Connects TPs between adjacent vertebrae
|
|
|
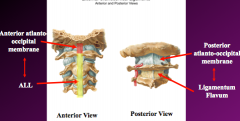
Atlanto-occipital joints (occiput and C1)
synovial joints, orientation provides flexion/extension movement of head and neck additional ligamentous support of atlanto occipital joints- anterior and posterior atlanto-occipital membranes (connect arches of C1 to occiput (edges of foramen magnum), help prevent excessive movement of the joint (stability) |
|
|
Atlantoaxial Joints
|

3 articulations- R/L facets and median atlantoaxial jt)
Median atlantoaxial joint- odontoid (dens) articulates with anterior arch of C1 (pivot type joint provides rotation C1 and occiput as unit on C2) Atlanto axial membrane- attaches to anterior body of C2 and anteiror arch of C1 Facet joints of C1-C2- synovial plane type of joint- provides gliding movement, orientation allows for rotation |
|
|
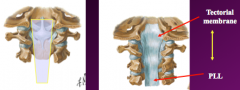
Tectorial membrane- acts as continuation of PLL, C2 to foramen magnum, runs posterior to cruciate ligament
|
|
|
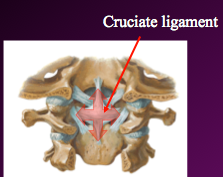
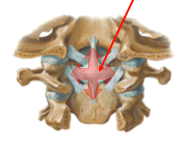
Cruciate Ligament (perviously known as cruciform ligament)
cruciate ligament= transverse ligament + superior/inferior longitudinal bands function- stabilizes dens against anterior arch of C1, acts as posterior wall and forms "socket" for dens |
|
|
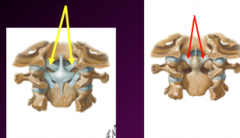
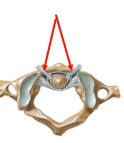
Alar Ligaments- extend from sides of dens to lateral margin of foramen magnum, limit excessive rotation
|
|
|
Apical Ligament- apex of dens to foramen magnum
|
|
|
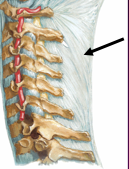
Fascia of posterior trunk- thoracolumbar fascia
invests the deep muscles of the back, attaches to SPs and TPs of T/L regions, provides origin of lats, transverse abdominal and internal oblique mm |
|
|
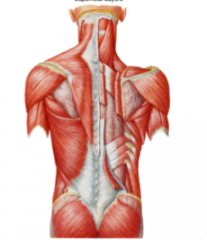
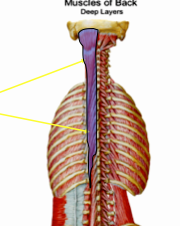
Muscles of the Back Hierarchy
|
Superficial layer (extrinsic, muscles that control the upper limb)- traps, lats, rhomboids and levator scapula
Intermediate layer of the back (extrinsic, assist in respiration control)- serratus posterior superior and inferior Deep layer of the back (intrinsic, act on vertebral column)- superficial= splenius capitus and cervicis, intermediate= errector spinae (iliocostals, longissimus, spinalis), deep= transversospinal group (semispinalis, multifidi, rotatores) |
|
|
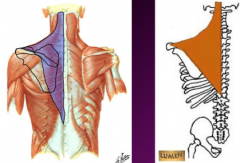
Trapezius (extrinsic, superficial layer)
O: medial third of the superior nuchal line, external occipital protuberance, ligamentum nuchae, spinous processes of vertebrae C7-T12 I: lateral third of the clavicle, medial side of the acromion and the upper crest of the scapular spine, tubercle of the scapular spine N: motor: spinal accessory (XI) A: elevates and depresses the scapula (depending on which part of the muscle contracts); rotates the scapula superiorly; retracts scapula |
|
|
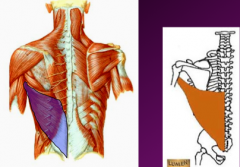
Latissimus dorsi (extrinsic, superficial layer)
O: vertebral spines from T7 to the sacrum, posterior third of the iliac crest, lower 3 or 4 ribs, sometimes from the inferior angle of the scapula I: floor of the intertubercular groove N: thoracodorsal nerve (C7,8) from the posterior cord of the brachial plexus A: extends the arm and rotates the arm medially |
|
|
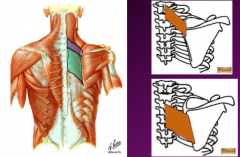
Both are extrinsic superficial
Rhomboid minor O: inferior end of the ligamentum nuchae, spines of vertebrae C7 and T1 I: medial border of the scapula at the root of the spine of the scapula N: dorsal scapular nerve (C5) A: retracts, elevates and rotates the scapula inferiorly Rhomboid major O: spines of vertebrae T2-T5 I: medial border of the scapula inferior to the spine of the scapula N: dorsal scapular nerve (C5) A: retracts, elevates and rotates the scapula inferiorly |
|
|
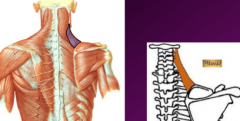
Levator Scapula (extrinsic, superficial)
O: transverse processes of C1-C4 vertebrae I: medial border of the scapula from the superior angle to the spine N: dorsal scapular nerve (C5); the upper part of the muscle receives branches of C3 & C4 A: elevates the scapula |
|
|
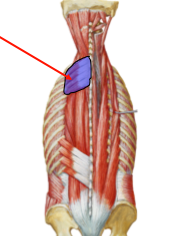
Intermediate Layer of Back Muscles – EXTRINSICS
Serratus posterior superior O: ligamentum nuchae, spines of vertebrae C7 -T3 I: superior borders of ribs 2-4 N: intercostals nerves 2-5 (branches of the ventral primary rami) A: elevates the upper ribs |
|
|
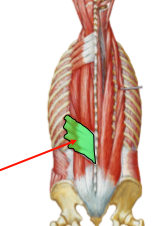
Intermediate Layer of Back Muscles – EXTRINSICS
Serratus posterior inferior O: thoracolumbar fascia, SP’s of vertebrae T11-L2 I: ribs 8-12 (inferior borders near their angles) N: branches of the ventral primary rami of spinal nerves T9-T12 A: pulls down lower ribs |
|

|
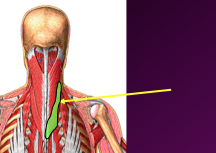
Deep Layer of Back Muscles– INTRINSICS (true back muscles) – innervated by DPR
Superficial layer of the deep back muscles = Splenius muscles – fiber direction is superolateral, cover vertical mm like a bandage (L. splenion) Splenius capitis O: ligamentum nuchae and spines of C7-T4 vertebrae I: mastoid process and lateral end of the superior nuchal line N: dorsal primary rami of spinal nerves C2-C6 A: Bilateral: extends neck/head Unilateral: lateral flex and rotate head/neck to same side |
|
|
Deep Layer of Back Muscles– INTRINSICS (true back muscles) – innervated by DPR
Superficial layer of the deep back muscles = Splenius muscles – fiber direction is superolateral, cover vertical mm like a bandage (L. splenion) Splenius cervicis O: ligamentum nuchae and spines of C7-T4 vertebrae I: posterior tubercles of the transverse processes of C1-C3 or 4 vertebrae N: dorsal primary rami of spinal nerves C2-C6 A: Bilateral: extends neck/head Unilateral: lateral flex and rotate head/neck to same side |
|
|
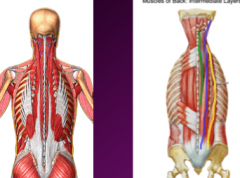
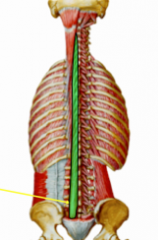
Intermediate layer of the deep back muscles
Collectively known as …Erector Spinae muscles…3 ”columns” of muscle, act as chief EXTENSOR of the vertebral column, each column shares common origin of broad tendon Iliocostalis – lateral column Longissimus – intermediate column Spinalis – medial column |
|
|
Iliocostalis
|
lliocostalis – lumborum, thoracis, and cervicis
O: broad tendon from posterior part iliac crest and sacrum, SP’s of lower L and S, supraspinus ligament I: angles of the ribs and cervical TP’s N: dorsal primary rami of spinal nerves A: Bilaterally: extends the vertebral column, assist with flexion (eccentric contraction) Unilateral: laterally bends the vertebral column |
|
|
Longissimus
|
Longissimus – thoracis, cervics, and capitis
O: broad tendon from posterior part iliac crest and sacrum, SP’s of lower L and S, supraspinus ligament I: ribs, TP’s at superior vertebral levels, mastoid process N: dorsal primary rami of spinal nerves A: Bilaterally: extends the vertebral column, assist with flexion (eccentric contraction) Unilateral: laterally bends the vertebral column |
|
|
Spinalis
|
Spinalis – spinalis thoracis, spinalis cervicis
O: broad tendon from posterior part iliac crest and sacrum, SP’s of lower L and S, supraspinus ligament I: spinous processes at superior vertebral levels and base of the skull N: dorsal primary rami of spinal nerves A: Bilaterally: extends the vertebral column, assist with flexion (eccentric contraction) Unilateral: laterally bends the vertebral column |
|
|
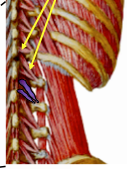
Deep Layer of the deep back muscles
a. Collectively known as Transversospinalis muscle group, all originate from TP’s and insert into SP’s Semispinalis – thoracics, cervicis, and capitis O: TPs of C4-T12 I: capitis: back of skull between nuchal lines; cervicis & thoracis: SP’s 4-6 vertebrae above origin N: dorsal primary rami of spinal nerves A: Bilaterally: extends the head and vertebral column in C and T region, stabilize vertebrae during local or isolated movements of vertebral column, assit with extension of vertebral column Unilateral: rotates the vertebral column to opposite side (contralateral rotation) May have proprioceptive function |
|
|
Deep Layer of the deep back muscles
a. Collectively known as Transversospinalis muscle group, all originate from TP’s and insert into SP’s Multifidus O: sacrum,TPs of T1-L5 and articular pillars (AP’s) of C4-7 I: spinous processes 2-4 vertebral levels superior to their origin N: dorsal primary rami of spinal nerves A: Bilaterally: extends the head and vertebral column in C and T region, stabilize vertebrae during local or isolated movements of vertebral column, assit with extension of vertebral column Unilateral: rotates the vertebral column to opposite side (contralateral rotation) May have proprioceptive function |
|
|
Deep Layer of the deep back muscles
a. Collectively known as Transversospinalis muscle group, all originate from TP’s and insert into SP’s Rotatores O: TPs of vertebral column I: long rotatores: SP’s (lamina) 2 vertebrae above origin short rotatores: SP’s (lamina) 1 vertebrae above origin N: dorsal primary rami of spinal nerves A: Bilaterally: extends the head and vertebral column in C and T region, stabilize vertebrae during local or isolated movements of vertebral column, assit with extension of vertebral column Unilateral: rotates the vertebral column to opposite side (contralateral rotation) May have proprioceptive function |
|
|
Minor deep intrinsics (not sure if need to know)
|
Levatores costarum (sometimes thought as analogous to intertransverse m in C and L regions)
O: Tips of C7 – T11 vertebrae I: pass inferolaterally and insert on rib between it’s tubercle and angle N: dorsal rami of C8-T11 A: elevate ribs, assisting with inspiration, assist with LF of spinal column |
|
|
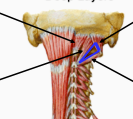
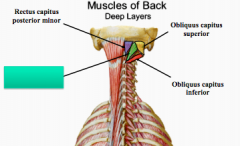
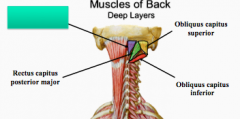
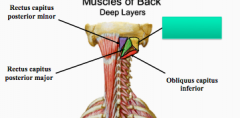
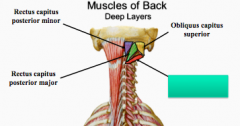
Suboccipital Triangle
1. Boundaries a. medial – rectus capitus posterior major b. lateral – obliquus capitus superior muscle c. inferior – obliquus capitus inferior 2. Floor – posterior arch of the atlas and posterior atlanto-occipital membrane 3. Roof – semispinalis capitis and longissimus capitis 4. Contents of suboccipital triangle– contains vertebral artery, suboccipital nerve (C1) and blood vessels |
|
|
Rectus capitis posterior major
O: SP of C2 (axis) I: inferior nuchal line (lateral portion) N: suboccipital nerve (DPR of C1) A: extends the head, rotate head to same side (ipsilateral rotation) |
|
|
Rectus capitis posterior minor
O: posterior tubercle of C1 (atlas) I: inferior nuchal line (medial portion) N: suboccipital nerve (DPR of C1) A: extends the head, rotate head to same side (ipslateral rotation) |
|
|
Obliquus capitis superior
O: TP of C1 (atlas) I: occipital bone above inferior nuchal line N: suboccipital nerve (DPR of C1) A: extends the head, rotates the head to the same side |
|
|
Obliquus capitis inferior
O: SP of the C2 (axis) I: TP of C1 (atlas) N: suboccipital nerve (DPR of C1) A: rotates the head to the same side (ipslateral rotation) |
|
|
Dura Matter
|
a. Dural sac extends from foramen magnum (continuatiuon of cranial dura)
b. Distal end of dural sac – filum terminale attaches to coccyx bone c. Spinal nerve roots pierce dura sac and form dural sleeves d. Epidural or extradural space = space between vertebral bone and dura, contains - adipose tissue, venous plexus • Epidural block – inject anesthesia direct effect on the spinal nerve roots of the cauda equina after they exit the dural sac |
|
|
Arachnoid ("spider")
|
a. middle layer between dura and pia
b. does not adhere to pia – creates a space known as subarachnoid space c. subarachnoid space is filled with CSF (cerebrospinal fluid) d. enlarged areas of the subarchnoid space = cisterns • lumbar cistern used for lumber puncture – sample CSF, inject contrast for myelogram, measure CSF pressure |
|
|
Pia Matter
|
a. inner most layer
b. in spinal cord – small extensions form dentate ligaments c. dentate ligaments anchor the spinal cord to the dura d. distal end – pia filament extends from conus medullaris to end of dural sac |