Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back

|
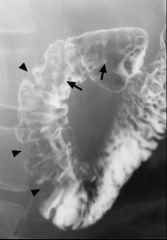
Intramural pseudodiverticula
Case findings: Multiple contrast-filled cavities, only 1 or 2 millimeter in diameter in the esophageal mucosa Dilated excretory ducts of deep mucous glands in esophagus Secondary to esophagitis: pseudodiverticula vanish when the esophagitis is treated (MC Candida) Dilated submucosal glands and ducts, which are similar to Rokitansky-Aschoff sinuses of GB DDX: Moniliasis Glycogen acanthosis |
|

|
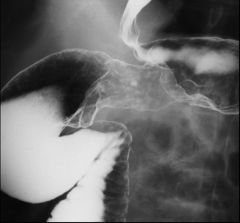
Esophageal varices
Etiology: portal venous hypertension Classification Uphill varices: mid to distal esophagus, portal hypertension Downhill varices: upper or mid esophagus, SVC obstruction DDX: Varicoid carcinoma: superficial spreading carcinoma, with thickened nodular tortuous longitudinal folds Has a rigid, fixed, nodular folds that do NOT change configuration (unlike varices) Esophagitis with thickened esophageal folds Lymphoma Squamous cell carcinoma |
|
|

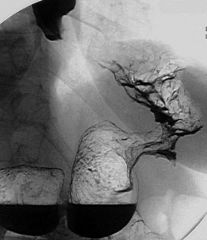
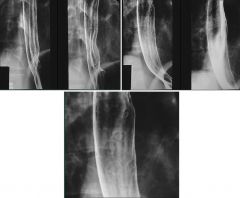
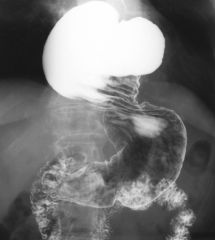
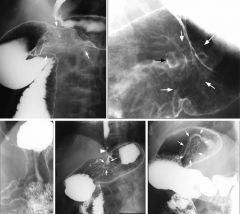
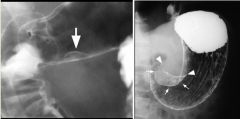
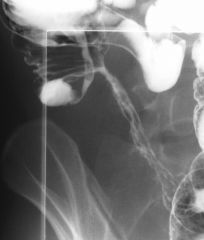
Pharyngeal pouch
Case findings: Contrast-filled cavity at the posterior wall of the esophagus Arises between the superior and the middle pharyngeal constrictors (congenitally weak point of the pharyngeal wall) Esophageal diverticula: Pulsion diverticula: contain no muscle in their wall so they tend to stay filled with barium after the rest of the esophagus empties Traction diverticula: contain muscle in their walls so they tend to empty with the rest of esophagus Esophageal diverticulum Pharyngo-esophageal (Zenker): Herniation of mucosa and submucosa through oblique and transverse muscle bundles of the cricopharyngeal muscle (pseudodiverticulum) Increased intraluminal pressures and tic formation in midline of Killian dehiscence at level of C5-C6 MC posterior Traction diverticulum (interbronchial diverticulum): Response to pull from fibrous adhesions following lymph node infection (MC TB) MC right anterior esophageal wall Distal (epiphrenic diverticulum): Pulsion, associated with hiatal hernia MC right Related to long-standing peptic esophagitis and strictures Killian-Jamieson diverticulum: Lateral to the insertion of the longitudinal tendon of the esophagus on the cricoid cartilage Diverticula are in the mid esophagus can congenital or traction: Traction types develop by traction from contiguous mediastinal inflammation and adenopathy such as from TB or histoplasmosis Other causes of mid and lower diverticula: Iatrogenic Ehlers-Danlos syndrome Motility disorders such as achalasia and esophageal spasm Zenker’s diverticulum Epiphrenic diverticulum Large diverticulum (arrows) arising from the posterior wall of the distal esophagus Traction diverticulum Traction diverticulum identified by black arrow MC located in the mid-esophagus Result from scarring and retraction of the esophageal wall due to granulomatous disease in adjacent subcarinal or hilar lymph nodes Presence of calcification in subcarinal (white arrows), hilar, or paratracheal lymph nodes TB |
|

|

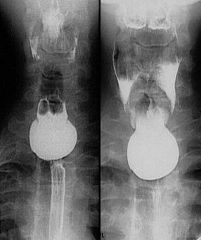
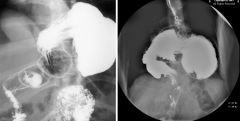
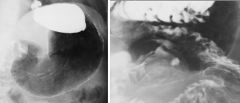
Paraesophageal hernia
Case findings: Gastroesophageal junction in normal position Parts of the stomach slip through the esophageal hiatus Hiatal hernia: Sliding: MC (80%), GEJ slides superior into the chest through the esophageal hiatus Paraesophageal: GEJ remains in its normal position, but parts of the stomach and peritoneum slip through the esophageal hiatus Sliding hiatal hernia |
|
|
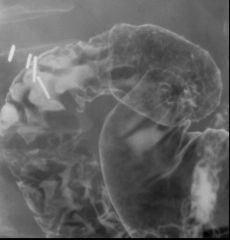
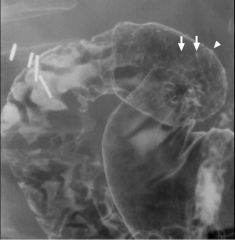
Gastric carcinoma
Case findings: Filling defect in the gastric body Location: MC pylorus > lesser curve, GEJ, greater curvature Types: Polypoid Ulcerating Infiltrating or schirrous: linitis plastica DDX: metastatic breast carcinoma Superficial spreading: confined to mucosa and submucosa Predisposing factors: H. pylori, adenomatous polyps, pernicious anemia, atrophic gastritis DDX gastric mass Malignant: Carcinoma, lymphoma, leiomyosarcoma, metastases Benign: Leiomyoma, lipoma, neurofibroma Polyps: Hyperplastic Adenomatous Hamartomatous Others: Bezoar, Nissen fundoplication, ectopic pancreas Gastric polyps Hyperplastic (MC) Adenomatous: increased risk of malignancy Familial adenomatous polyposis (FAP) Gardner’s syndrome Turcot syndrome: associated with CNS tumors (e.g., gliomas) Hamartomatous: Peutz-Jeghers syndrome Cowden syndrome Inflammatory: Cronkhite-Canada syndrome |
|

|

Duodenal diverticulum
Case findings: Large duodenal diverticulum with some small diverticula at the top MC located near the ampulla Intraluminal duodenal diverticulum (2 cases) |
|

|

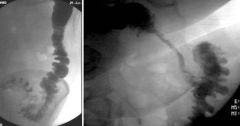
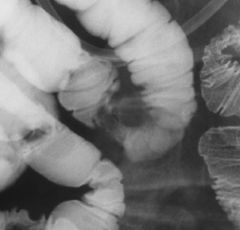
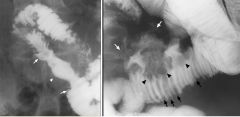
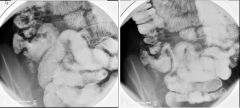
Celiac disease (sprue)
Case findings: Proximal small bowel dilatation Smudging and dilution of barium in LUQ Moulage sign: produced by barium reaching such diluted, fluid-filled, hypotonic segments Normal sized, but widely spaced, sparser folds in jejunum Associated with transient intussusception Risk of intestinal lymphoma Features: Small bowel dilatation Moulage pattern: barium pooling Flocculation: excessive mucus prevents an adequate coating of the mucosa by the barium (barium flocculates in the presence of mucus) Jejunization of the ileum: increased number of folds in the ileum, with reversal of the normal jejuno-ileal fold pattern Jejunization of the ileum Lymphoma arising in celiac disease as thick, slightly undulating folds (arrows) and smooth nodules (arrowheads) |
|

|

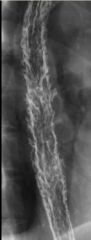
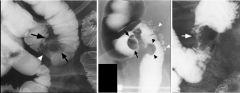
Crohn’s
Case findings: Deep and superficial linear ulcerations and small bowel wall thickening near the terminal ileum Fistula track Features: Deep and superficial linear ulcerations Cobblestoning Bowel wall thickening, strictures, skip lesions Pseudopolyposis, fistula DDX: Yersinia colitis: fold thickening (early finding), aphthoid ulcers, coarsened mucosal surface and inflammatory nodules (indistinguishable from early Crohn’s) Deeper ulceration and marked luminal narrowing is unlikely Heals to a lymphoid hyperplasia pattern, resolves completely Ileitis: due to Shigella, Salmonella, Campylobacter Self-limited and will not reach a stenotic stage Tuberculosis: identical to Crohn’s Cobblestoning: deep and superficial linear ulcerations in descending colon Numerous barium-filled linear clefts are seen as straight, longitudinal and transaxial lines (arrows) Cobblestones: between the fissures are residual islands of less inflamed mucosa Confined to the mucosa and submucosa with thickened and curved folds Long mesenteric border ulcer is seen as a thin barium-filled line (arrows) Area of ulceration merging with marked narrowing (arrowhead) of the terminal ileum Small ulcers are also seen in the ascending colon (arrow) |
|

|
Ulcerative colitis
Case findings: Loss of haustra and mucosal distortion |
|

|
Diverticulitis
Case findings: Irregular bowel wall thickening, with narrowing of the sigmoid lumen Mucosal pattern preserved (implies a benign process) |
|

|
Moniliasis
Case findings: Diffuse nodular and plaque like mucosal defects Plaque like defects are longitudinally oriented Sharply defined plaques DDX: Glycogen acanthosis Reflux esophagitis: ill-defined plaques With progression, esophagus may have a grossly irregular or shaggy contour (shaggy esophagus) Shaggy contour due to multiple plaques, pseudomembranes, and ulcers |
|

|
Herpes esophagitis
Multiple small discrete superficial ulcerations: appears as a small barium collection with a surrounding halo of lucency due to edema No fold thickening, normal esophageal contour Ulcers may be clustered, MC in mid-esophagus (relative sparing of distal esophagus) Discrete ulcers surrounded by radiolucent halos of edematous mucosa Normal intervening mucosa |
|

|
Glycogen acanthosis
Degenerative condition, MC seen in elderly Asymptomatic No risk of malignant degeneration Features: multiple small, rounded nodules or plaques in the mid or distal esophagus DDX: Candida esophagitis (moniliasis): well-defined plaques Reflux esophagitis: nodular mucosa (ill-defined plaques) |
|

|

Barrett’s esophagus
Case findings: Reticular pattern is distal esophagus, adjacent to a stricture in the mid esophagus Adenocarcinoma arising in Barrett’s esophagus may appear as a flat slightly elevated nodular lesion or as a sessile polyp Plaque-like tumor: area of nodular mucosa in distal esophagus (arrows) above a hiatal hernia Edge of plaque-like lesion is seen en face as a white line (arrowhead) |
|

|
CMV esophagitis
Case findings: Giant flat ulcer (> 3 cm) on the posterior wall of the distal esophagus with a thin, radiolucent rim of edema May also present with multiple small ulcers indistinguishable from Herpes esophagitis DDX giant flat ulcer: HIV esophagitis CMV esophagitis |
|

|
Esophageal leiomyoma
Case findings: Upper and lower borders of the lesion form slightly obtuse angles (in profile) with the adjacent esophageal wall (submucosal lesion) DDX submucosal lesion: MC leiomyoma LC fibroma, neurofibroma, lipoma, hemangioma, granular cell tumor, squamous papilloma DDX multiple submucosal lesion: Granular cell tumor Neurofibromatosis Lymphoma |
|

|

Esophageal carcinoma
Case findings: Iinfiltrating esophageal cancers cause irregular narrowing and obstruction of the lumen with nodularity and/or ulceration of the mucosa MC squamous cell Types: Infiltrating Polypoid Ulcerative Varicoid: superficial spreading Polypoid: lobulated or fungating intraluminal masses, often containing areas of ulceration Polypoid edge of the tumor is etched in white by barium Central ulcer protrudes from the expected luminal contour Advanced infiltrating carcinoma of the mid-esophagus Varicoid esophageal carcinoma Focal nodularity in the mid-esophagus due to tiny, coalescent nodules and plaques DDX: Moniliasis: localized plaque formation, the plaques tend to have discrete, well-defined borders with normal intervening mucosa |
|

|

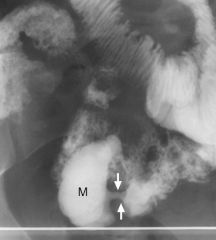
Achalasia
Case findings: Dilated, aperistaltic esophagus that tapers abruptly to a narrowed, fixed lumen Tapering is concentric and the lumen contour is absolutely smooth Primary achalasia: Result of degeneration of the myenteric plexus innervating the lower esophageal sphincter Failure of relaxation and lack of coordinating peristalsis (aperistalsis) Secondary achalasia (pseudoachalasia): Most carcinomas that cause achalasia are adenocarcinoma arising either in the stomach or in distal esophagus in a Barrett's esophagus Chagas' disease (trypanosomiasis) Achalasia (secondary) Secondary achalasia due to metastasis to GEJ from adenocarcinoma of the mid esophagus Smooth, tapered narrowing (black arrow) of the distal esophagus just above GEJ Ulcerated mass (white arrows) in mid esophagus |
|

|
Annular pancreas
Case findings: Circumferential narrowing of the 2nd portion of duodenum Mucosal pattern is preserved |
|

|

Erosive gastritis
Case findings: Multiple erosions present in the antrum of the stomach, seen as small barium-filled ulcer craters with a radiolucent halo (edema) around them Incomplete linear and serpiginous erosions in the distal stomach (erosive gastritis) Etiology: NSAID, H. Pylori, alcohol, Crohn’s Associated with gastric atrophy Atony is common in elderly Stomach has a tubular appearance Lack of normal gastric mucosal folds Areae gastricae may be smaller and irregular in the gastric fundus and body Case findings: Smooth, non-distensible antrum No peristalsis seen on fluoroscopy |
|
|
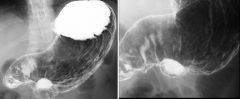
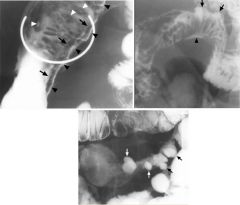
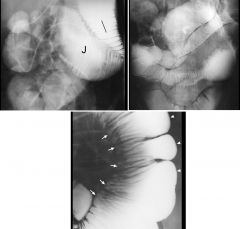
Benign gastric ulcer
Large ulcer crater (arrowhead) on greater curvature Multiple folds (arrows) radiating to the edge of ulcer crater Folds taper gradually to the edge of the crater Crater itself extends beyond the outlines of the gastric lumen Supine position: fundus posterior and contains barium Large ring shadow (arrow) etched-in-white appearance in the gastric antrum (anterior non-dependent wall) Prone position Large collection of barium (arrow) in the same area of the gastric antrum (anterior dependent portion) Ulcer crater protrudes beyond the contour of the stomach Ulcer is central in the mound (of inflammation and edema) that is smooth and symmetrical Hampton's line: mucosa is more resistant to ulceration than the fat in the lamina propria and submucosa Ulcer often spreads laterally in the soft submucosal fat, undermining the mucosa Undermined mucosa is seen when a gastric ulcer is demonstrated in profile (seen as a thin Hampton's line crossing the ulcer crater) Folds radiating towards the ulcer crater are smooth and taper towards the crater's edge No masses associated with the ulcer Mucosa surrounding the ulcer is not nodular |
|

|
Ectopic gastric mucosa
Case findings: Multiple 1-3 mm, polygonally-shaped radiolucent filling defects in the duodenal cap |
|
|
Crohn’s of the duodenum
Large polygonal nodules covering the mucosal surface of the duodenal cap 2nd part of the duodenum shows mucosal irregularity Focal eccentric narrowing of the lumen (arrowheads) Two aphthoid ulcers (arrows) in the proximal 2nd part of the duodenum |
|
|
Gastric volvulus
Mesenteroaxial (this case): Stomach has rotated about the gastrohepatic ligament (lesser omentum) Organoaxial: Stomach flips superiorly parallel to the longitudinal axis of the organ Greater curvature lies superior to the lesser curvature Oganoaxial gastric volvulus Gastric volvulus Organoaxial volvulus of the stomach |
|
|
Erosive duodenitis
Multiple aphthoid-like small ulcers in the duodenal cap tiny barium collections surrounded by radiolucent halos of edema Erosions are seen both en face (arrows) and in profile (arrowhead) |
|

|
Duodenal hematoma
Diffuse thickening of the duodenal folds DDX: Lymphoma |
|

|
Gastric bezoar
Complication of subtotal gastrectomy and vagotomy Poorly chewed fibrous foods, lack of gastric peristalsis, absence of hydrochloric acid |
|
|
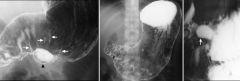
Gastric carcinoma
Sharply circumscribed constricting lesion (arrows) in proximal body Mucosa is irregular and there are shoulders at the lesion's margins Segment involved by the tumor is rigid and non-distensible Gastric (ulcerative) carcinoma Ulcerated lesion in the body of the stomach with irregularly thickened folds around it Ulcer crater (black) is rectangular in shape Surface pattern of the adjacent mucosa (white) is nodular Nodules are of different sizes and more irregular than the usual areae gastricae pattern Gastric carcinoma Diagnosis: gastric carcinoma, linitus plastica Body and antrum of the stomach are narrowed, rigid No peristalsis was seen Diagnosis: ulcerating carcinoma of cardia, with extension into lower esophagus Irregular shaped ulcer crater (arrows) in gastric cardia Folds radiating towards the ulcer crater are of uneven thickness, and most do not reach the crater edge Distal esophagus is narrowed, secondary to proximal extension of the tumor (arrowhead) Mass in the cardia with thickened folds (arrows) Normal cardiac rosette is obliterated Mucosa is coarsely nodular in some areas |
|
|
Gastrointestinal stromal tumor
Case findings: Well- circumscribed, smooth-surfaced 3 cm mass in gastric antrum Barium-filled ulcer crater is centrally located Ectopic pancreatic rest Single, smooth-surfaced, relatively flat, polypoid lesion (arrow) on the greater curvature of the distal gastric antrum Gastrointestinal stromal tumor Large smooth broad-based polypoid lesion (arrows) along distal lesser curvature Lesion has abrupt margins (arrowheads) with the luminal contour submucosal mass Large, solitary submucosal masses of the stomach MC GIST and lymphoma (about 50% are ulcerated) DDX: lymphoma |
|

|

Gastric lymphoma
Loss of the normal gastric rugal pattern, with multiple, large ulcers (large arrows) Stomach is diffusely narrowed, which is the result of diffuse infiltration by lymphomatous tissue Well demarcated line (small arrows) in fundus, suggesting that the barium is being displaced by a mass effect exerted by the tumor MC NHL of B-cell origin, arising in the mucosa-associated lymphoid tissue of the stomach (MALT) Associated H pylori gastritis Features: MC appearance an infiltrating lesion May be focal or diffuse, nodular or smooth thickening of the rugal folds Gastric wall may either be rigid mimicking scirrhous carcinoma or be pliable due to the soft nature of the lymphomatous infiltrate Multiple ulcers are often present Ulcerated submucosal mass Ulcerating mass with a nodular surface |
|
|
Carcinoid
Smooth-surfaced, broad-based, sessile polypoid lesion (arrows) in the ileum Wall opposite the tumor is mildly in-bowed (arrowhead) DDX sessile polypoid lesion in ileum: Carcinoid Gastrointestinal stromal tumor (GIST) Lipoma: soft and change size or shape DDX ileal submucosal lesion: Metastasis Disseminated lymphoma Kaposi's sarcoma Carcinoid tumor Polypoid lesion in the terminal ileum (black arrowhead), carcinoid lesion Ileal diverticula (white arrowheads) and the smooth-surfaced submucosal mass (black arrows) at the entrance of the appendix into the cecum (mucinous cystadenoma of the appendix) Carcinoid (annular) Mucosal folds are shown to be preserved (arrow) |
|

|
Crohn’s
Ulcer (black arrowheads) on the mesenteric border of the distal ileum Radiolucent collar of edema (arrows) parallels the barium-filled groove Aphthoid ulcers (white arrowheads) More extensive along the mesenteric side of the small intestine, and extends along vessels and lymphatics entering the small bowel mesentery Linear mesenteric border ulcer: Associated with fibrosis and shortening of mesenteric side Whenever flattening of a mesenteric border is seen in a Crohn's, suspect mesenteric border ulceration Look on antimesenteric side for sacculations Mesenteric border ulcer (arrowhead) folds radiate toward the ulcer Opposite wall (antimesenteric border) is mildly sacculated (arrows), which is the result of the folds radiating toward the ulcer, and is associated shortening of the mesenteric border With progressive luminal narrowing and fibrosis of the wall, some of the antimesenteric sacculations survive as diverticula-like outpouchings (arrows) |
|
|

Crohn’s
DDX of small bowel stricture: Ischemia: MC solitary, smooth surfaced narrowing, with gradually tapering margins Radiation: smooth, thick folds perpendicular to the longitudinal axis If very long-standing, radiation strictures may be smooth circumferential tubular narrowing Neoplasm: annular constricting tumors (primary or metastatic) are sharply demarcated with shoulder formation Ulcerative colitis: rare, chronic stage of UC with short annular constrictions separating dilated segments are present Stricture of the terminal ileum (string sign) |
|

|
Crohn’s
Ileosigmoid fistula due to terminal ileal Crohn's disease BE: shows reflux of barium into the TI, and a strictured TI |
|

|

Small bowel ischemia
Intramural hemorrhage: identical on SBFT submucosal edema or blood causes thumbprinting, with thickened but straight folds Barium trapped between the thick folds produces interspace spikes CT target sign = barium thumbprinting Etiology of intramural hemorrhage/ischemia: Low flow states Emboli or atherosclerosis Vasculitis: SLE, RA, Behçet's, HSP Bleeding from hemophilia, ITP, anticoagulation, or intrinsic coagulopathies Radiation enteropathy |
|

|
Primary small bowel lymphoma
Grow first by submucosal infiltration longitudinally resulting in thickened valvulae conniventes Then extends through the thickness of the wall with effacement of valvulae conniventes Lumen can be mildly narrowed by submucosal lymphoma, but obstruction is uncommon If the smooth muscle of the wall is destroyed, the lumen can expand (aneurysmal dilatation) Features: MC type is infiltrative 2nd MC type is cavitary (ulcerating) DDX: Malignant GIST Metastatic melanoma Rarely primary adenocarcinoma May infiltrate short segment of small bowel Segment of annular narrowing (arrowhead) of the distal jejunum Borders are abrupt (arrows), but not shelf-like Normal folds are absent NOTE: lack of obstruction and relative mild luminal narrowing favor primary lymphoma a over primary adenocarcinoma Large cavity (white arrows) extends into the small bowel mesentery Surface of cavity is nodular Folds of the SB are thick (black arrows) Large tumor nodules (arrowheads) are seen on the mesenteric border |
|

|
Meckel’s diverticulum
Case findings: Smooth-contoured saccular outpouching from the antimesenteric wall of a RLQ ileal loop No folds are seen in the outpouching Occurs at obliterated omphalomesenteric duct Contains all layers of the bowel wall Ectopic gastric mucosa may be present (hemorrhage) Pertechnetate scan Junction of the diverticulum with the antimesenteric border of the distal ileum is a narrow neck (arrows) |
|

|
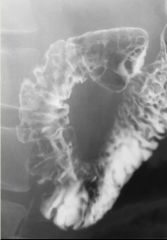
Scleroderma
Dilated duodenum and jejunum Despite the massive dilatation, there are 7-8 folds per inch in the first jejunal loop Dilated duodenum and jejunum Despite the massive dilatation, there are 7-8 folds per inch in the first jejunal loop Although the number of folds/inch remains is normal (5-6/inch), there are too many folds for the massive luminal dilatation Lumen is dilated Folds radiate toward the mesenteric border (arrows) due to asymmetric scarring Antimesenteric border shows broad-based sacculations (arrowheads) Classic appearance: Luminal dilatation Tethered, crowded folds Broad based sacculations opposite these folds |
|

|
Familial adenomatous polyposis
Hamartomatous polyps: Cowden (multiple hamartoma syndrome): associated with breast and thyroid cancer Peutz-Jeghers Multiple hamartomas MC stomach Mucocutaneous hyperpigmentation Adenomatous polyps: Familial polyposis coli Turcot: associated with brain tumors (GBM, medulloblastoma) Gardner’s syndrome: colonic polyps, osteomas (frontal sinus, mandible), ST tumors (desmoid tumors, epidermoid inclusion cysts, fibroma, lipoma, leiomyoma) Juvenile polyps: Juvenile polyposis coli Cronkite-Canada: inflammatory juvenile polyps |
|

|

Ulcerative colitis
Early ulcerative colitis: Colonic mucosa replaced by a diffusely granular appearance Corresponds to edema and hyperemia, and may precede actual ulceration Rectum shows diffuse narrowing Widened presacral space |
|
|
Crohn’s
Case findings: Distal ileum fold thickening and cobble-stoning Mild transient spasm of this portion of bowel indicating acute inflammation at this site No skip lesions, obstructions, leaks, or masses DDX terminal ileum fold thickening: Crohn's disease Yersinia infection Mycobacterium tuberculosis ileitis Adjacent appendiceal abscess |
|
|
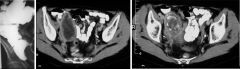
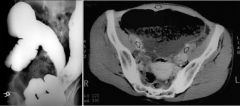
Mucinous cystadenoma of appendix
Case findings: BE: Smooth, sharply outlined, broad based extramucosal mass impressing the apex of the cecum CT: Sharply defined round mass in RLQ Central part has low attenuation Wall of the lesion is thickened Peripheral calcification |
|
|
Crohn’s
Case findings (SBFT): 20cm segment of the terminal ileum is narrowed and non-distensible Within the right mid abdomen, there is a shorter, approximately 10cm segment of similar narrowing Early findings: Aphthoid ulcer: shallow pinpoint mucosal erosions surrounded by an edematous mound Late findings: Cobblestone pattern: ulcerations grow and fuse together, forming linear confluent deep ulcerations separated by edematous mucosa Thickened and distorted folds String sign: progressive narrowing of the lumen (MC in terminal ileum)a Rigid, featureless bowel, strictures and obstruction, and foreshortening of bowel Asymmetric involvement of bowel wall both longitudinally and circumferentially lesions MC on mesenteric side of intestine Sinus tract and fistula formation, originating in deep ulcers or fissures Creeping fat: inflamed mesenteric fat (stranding) accumulate on serosal surfaces |
|
|
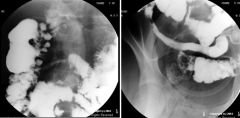
Cecal bascule
Case findings: BE: Contrast flowed to the level of what initially appeared to represent the cecum However, the hugely distended loop of bowel located in the pelvis and extending into the mid-abdomen did not fill with contrast No “birds beak” sign was demonstrated CT: Markedly distended bowel loop in the pelvis DDX: cecal volvulus Form of volvulus in which the cecum folds anteromedially in front of the ascending colon, producing a flap-valve occlusion at the site of flexion Torsion in the transverse plane Cecum usually falls into the pelvis, resting centrally Birds beak sign: not present with bascule because there is no true twist Axial torsion: classic cecal volvulus Rotation occurs in the longitudinal plane Cecum turns upward and usually lies in an ectopic location (MC LUQ) Classic “kidney-bean” appearance Bascules represent up to 1/3rd of cecal volvuli Two forms of cecal volvuli have similar presentations and treatments |