![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
266 Cards in this Set
- Front
- Back
|
Iliac crest |
site for contusion - hip pointer - common site for autologous bone graft harvest |
|
|
Anterior superior iliac spine |
- origin of sartorious muscle - avulsion fx can happen here - Lateral femoral cutaneous nerve courses here and can be entrapped - Landmark used for measuring Q angle of knee |
|
|
Symphysis pubis |
Site of osteitis pubis - uncommon cause of anterior pelvic pain |
|
|
Inguinal ligament |
- External iliac artery become femoral artery here - femoral pulses can be palpated just inferior to the ligament in femoral triangle |
|
|
Greater trochanter |
- tenderness can indicate trochanteric bursitis |
|
|
Erector spinae muscles |
overuse and spasm are common causes of lower back pain |
|
|
Posterior superior iliac spine |
Site of bone graft harvest in posterior spinal procedures |
|
|
Sacroiliac joint |
Degeneration of joint can cause lower back pain |
|
|
Ischial tuberosity |
Avulsion fracture (hamstring muscle) or bursitis can occur here |
|
|
Pelvis Osteology |
- Combination of 3 bones (two innominate bones and sacrum) and 3 joints (2 sacroiliac joints and symphysis pubis) - Pelvis has no inherent stability. Requires ligament support for stability - Two portions of pelvis divided by pelvic brim/iliopectineal line |
|
|
False (greater) pelvis |
- above the brim, bordered by sacral ala and iliac wings |
|
|
True (lesser) pelvis |
- below the brim, bordered by ischium and pubis |
|
|
Sacrum characteristics |
- 5 vertebrae are fused - 4 pairs of foramina - Ala (wing) expands to laterally - Sacral canal opens to hiatus distally - kyphotic (approx 25 degrees) the apex is at S3 |
|
|
Primary Sacral ossification |
- Body ossifies at 8 weeks fetal and fuses at 2-8 years - Arches and costal elements fuse at 2-8 years |
|
|
Secondary sacral ossification |
Ossifies at 11-14 years and fuses at 20 years |
|
|
Sacrum comments |
- Transmits weight from spine to pelvis - Nerves exit through sacral foramina - Ala is common site for sacral fractures - Sacral canal narrows distally before opening to sacral hiatus - segments fuse to each other at puberty |
|
|
Coccyx characteristics |
- 4 vertebrae are fused - Lack features of typical vertebrae |
|
|
Primary coccyx ossification |
- Primary arch ossifies at 7-8 weeks fetal and fuses at 1-2 years - Body ossifies at 7-8 weeks fetal and fuses at 7-10 years |
|
|
Coccyx comments |
- is attached to gluteus maximus and coccygeal muscle - common site for tailbone fracture |
|
|
Inominate bone characteristics |
- 3 bones (ilium, iscium, and pubis) fuse to become one bone at triradiate cartilage in acetabulum - Ilium: body and ala (wing) - Pubis: inferior and superior rami - Ischium: body and tuberosity - Acetabulum: socket of hip joint, has 2 walls (A&P) and notch/condyloid fossa inferiorly. Articular cartilage is horseshoe shaped |
|
|
Primary inominate bone ossification |
- One in each body: ossifies at 2-6 mos and fuses to acetabulum at 15 years |
|
|
Secondary inominate ossification |
Iliac crest, Triradiate, ischial tuberosity, AIIS, and Pubis - ossify at 15 years - All fuse at 20 years |
|
|
Inominate bone comments |
- Iliac crest is common site for both tricortical and cancellous bone graft harvest - Contusion to iliac crest known as hip pointer - Iliac crest ossification used to determine skeletal maturity (Risser stage) - Multiple iliac spines serve as anatomical landmarks and muscle insertion sites (ASIS, AIIS, PSIS, PIIS) - Acetabulum 45 degrees oblique orientation, 15 degrees anteverted |
|
|
Skeletal maturity scale |
Risser stage |
|
|
Anterior superior iliac spine attachments |
- Sartorius - Inguinal ligament - Transverse and internal oblique abdominal muscles |
|
|
ASIS comments |
- LCFN crosses the ASIS and can be compressed here - Sartorius can avulse from ASIS - Landmark to measure Q angle |
|
|
Anterior inferior iliac spine attachments |
- Rectus femoris - tensor fasciae latae - Iliofemoral ligament (hip capsule) |
|
|
AIIS comments |
- Rectus femoris can avulse from here |
|
|
Posterior superior iliac spine attachments |
- Posterior sacroiliac ligaments - marked by skin dimple - Excellent bone graft site |
|
|
Arcuate line attachments |
- Pectinues - AKA pectineal line - Strong weight bearing region |
|
|
Gluteal lines |
- 3 lines: anterior, posterior, inferior - Separate origins of gluteal muscles |
|
|
Lesser trochanter attachments |
- iliacus/psoas muscle - Tendon can snap over trochanter (snapping hip) |
|
|
Ischial tuberosity attachments |
- Sacrotuberous ligaments - hamstrings can avulse (avulsion fx) |
|
|
Excess friction over ischial tuberosity |
bursitis = weaver's bottom |
|
|
Ischial spine attachments |
- coccygus and levator ani - sacrospinous ligaments |
|
|
Lesser sciatic foramen attachments |
- Short external rotators exit - obturator externus/internus |
|
|
Lesser sciatic foramen comments |
- obturator internus is landmark to posterior column - obturator externus not seen in posterior approach |
|
|
Greater sciatic foramen structures |
- superior gluteal nerve/artery - Piriformis muscle - pudendal nerve - inferior pudendal artery - interior pudendal artery - nerve to obturator internus - posterior cutaneous nerve of thigh - sciatic nerve - inferior gluteal nerve - inferior gluteal artery - Nerve to quadratus femoris |
|
|
Greater sciatic foramen comments |
- Piriformis muscle is reference point - superior gluteal nerve and artery exit superior to piriformis - POP'S IQ is mnemonic for nerves that exit inferior to the piriformis (med to lat) - Sciatic nerve (especially peroneal division) may exit pelvis above or through the piriformis as an anatomic variation |
|
|
Anterior (iliopubic) acetabular column |
- Superior pubic ramus - Anterior acetabular wall - Anterior iliac wing - Pelvic brim |
|
|
Posterior (ilioischial) acetabular column |
- ischial tuberosity - posterior acetabular wall - greater and lesser sciatic notches |
|
|
Acetabular zones |
zones defined by 2 lines - ASIS to center of acetabulum - perpendicular to line 1 Structures can be injured when screws are placed in these zones (acetabular cups) |
|
|
Anterior superior acetabular zone |
- External iliac artery and vein - do not put screws in this zone |
|
|
Anterior inferior acetabular zone |
- obturator nerve, artery, and vein - do not put screws in this zone |
|
|
Posterior superior acetabular zone |
- Sciatic nerve, Superior gluteal N/A/V - SAFE zone |
|
|
Posterior inferior acetabular zone |
- Sciatic nerve, Inferior gluteal N/A/V, Inferior pudendal N/A/V - This is a secondary safe zone. Safe screw placement can be achieved with care if necessary |
|
|
AP pelvic radiograph technique |
- AP - Internally rotate feet 15 degrees - Beam directed at midpelvis |
|
|
AP pelvic radiograph findings |
6 radiograph lines - iliopectineal (anterior column) - Ilioischial (post column) - radiographic teardrop - Acetabular roof (dome) - Anterior acetabulum rim/wall - posterior acetabulum rim/wall |
|
|
AP Pelvic radiograph clinical application |
- screen for fractures - use ATLS protocol - dysplasia - DJD/arthritis |
|
|
Pelvic inlet view technique |
- AP - beam 45 degrees caudal |
|
|
Pelvic inlet view radiograph findings |
- SI joint - pelvic brim/pubic rami - sacrum |
|
|
Pelvic inlet view XR clinical application |
- pelvic ring fractures - shows posterior displacement or symphysis widening |
|
|
Pelvic outlet view XR technique |
- AP - beam 45 degrees cephalad |
|
|
Pelvic outlet view XR findings |
- iliac crest - symphysis pubis - sacral foraminal |
|
|
Pelvic outlet view XR clinical application |
- pelvic ring fractures shows superior displacement of of hemi-pelvis |
|
|
Oblique/Judet views (obturator oblique) XR radiograph |
- Beam at affected hip - elevate affected hip 45 degrees |
|
|
Obturator oblique XR findings |
obturator foramen |
|
|
Obturator oblique XR clinical applications |
- Acetabulum fx: anterior column, posterior wall |
|
|
Iliac oblique XR technique |
- Elevated unaffected hip 45 degrees |
|
|
Iliac oblique XR findings |
- Iliac crest - sciatic notches |
|
|
Iliac oblique XR clinical applications |
- Acetabulum fx: posterior column, anterior wall |
|
|
Sacral fracture description |
- Mechanism: elderly (fall), young (high energy) - Isolated injuries rare, usually associated w/ pelvis/spine fx - Nerve root injury very common - Plain XR identifies < 50% of fx - Easily missed and difficult to treat, can lead to chronic pain |
|
|
Sacral fx H&P |
- Hx: Trauma, pain +/- neuro symptoms - PE: palpate spine and sacrum. Complete neuro exam including rectal exam |
|
|
Sacral fracture workup |
- XR: AP pelvis, lateral sacrum - CT: necessary for diagnosis and pre-op planning |
|
|
Sacral fracture classification |
By direction of fracture - I: Vertical - II: Transverse - III: Oblique - Complex: U or H shaped |
|
|
Vertical Sacral fx: Denis classification |
- Zone 1: lateral to formina - Zones 2: through foramina - Zone 3: medial to formina |
|
|
Sacral fx Tx |
- Minimally displaced/stable: non operative - Displaced/unstable: 1) Closed reduction and percutaneous fixation 2) ORIF - Nerve injury: decompression |
|
|
Sacral fx complications |
- nerve root and injury - cauda equina syndrome (esp zone 3 fractures), nonunion/malunion, chronic pain |
|
|
Pelvic ring fx |
- mechanism: high energy blunt trauma - Multiple associated injuries: GI/GU, extremity fxs, neurologic, vascular head - very high morbidity due to uncontrolled hemorrhage (venous > arterial bleeding) especially w/ APC3 fractures (open bood) - Open fx has higher morbidity - Stability of x based on ligament disruption - Avulsion of iliolumbar ligament/L5 transverse process suggests unstable fx - Lateral compression most common: LC1 posterior directed force, LC2: anterior directed force |
|
|
Pelvic ring rx H&P |
Hx: High energy trauma, pain +/- neuro sxs PE: inspect perineum for open injury. LE may be malrotated. Pelvic "rock". - Rectal and vaginal exam for associated injuries - Complete neuro exam including rectal bone and bulbocavernous reflexes |
|
|
Pelvic ring fx workup |
- XR: AP pelvis, inlet and outlet views are essential - CT: essentially useful to define sacral/SIJ injury - Angiogram: if hemodynamicaly unstable after pelvic stabilization, consider embolization of artery |
|
|
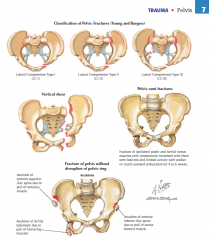
Pelvic ring fx Classification: Young & Burgess (AP compression) |
- I : < 2.5 cm pubis diastasis + 1 or 2 pubic rami fxs - II : > 2.5 cm diastasis + anterior SI injury, but vertically stable - III: Complete anterior (symphysis) and posterior (SIJ) disruption. Unstable |
|
|
Pelvic ring fx Classification: Young & Burgess (Lateral compression) |
- I : Sacral compression + ipsilateral rami fracture - II : LC1 (post directed force) + iliac wing fx or posterior SIJ injury. Vertically stable - III : LC2 (ant directed force) w/ contralateral APC3 windswept pelvis) |
|
|
Pelvic ring fx classification: Young & Burgess (Vertical Shear) |
- SIJ and ST/SS ligament disruption, + rami fxs - Vertically unstable |
|
|
Pelvic ring fx tx |
- ATLS protocol. Tx life threatening injuries - Pelvic hemorrhage: pelvis compression (sheet) or external fixation to reduce pelvic volume - Diverting colostomy for open injury or any communication w/ open bowel - Non-operative tx: WBAT for LC1, APC1, ramus rx |
|
|
Operative tx for pelvic ring fx |
- Operative for LC2/3, APC 2/3 and vertical stress - Anterior: ORIF of symphysis - Posterior 1: ORIF of iliac wing and sacral fractures - Posterior 2: screws for dislocated SIJ |
|
|
Pelvic ring fx compliations |
- hemorrhage (Venous > arterial), internal pudendal artery > superior gluteal artery - neuro injuries (L5 risk w/ SI screws) - malunion/non union - chronic pain - functional disability - infection - thromboembolism |
|
|
pelvic ring fx |
|
|
|
Pelvic fracture (other) |
- mechanism: low energy, trauma - Stable isolated fx, pelvic ring not disrupted - can occur in osteopenic bone |
|
|
Pelvic fracture evaluation |
- Hx: pain, especially w/ WB - PE: TTP at bony site - XR: AP, inlet/outlet views - CT: often not needed, can determine displacement |
|
|
Pelvic fracture classification |
- Isolated fx: inferior or superior pubic rami, iliac wing/crest - Avulsions: ASIS (sartorius), AIIS (rectus femoris), Ischial tuberosity (hamstrings) |
|
|
Pelvic fracture tx |
- Isolated fx: treat w/ limited rest, WBAT - Avulsion fx: most treated non-operatively. Reattach if widely displaced |
|
|
Pelvic fracture complications |
- Malunion/non-union - chronic pain - pain/disability - thromboembolism |
|
|
Pelvic acetabular fx |
|
|
|
Acetabular fx description |
- Mechanism: high energy blunt trauma, femoral head into acetabulum - fracture pattern determined by force vector and position of femoral head at impact - Multiple associated injuries: GI/GU, extremity fx |
|
|
Acetabular fx surgical approaches |
- Kocher-Langenbeck: posterior fxs (PW, PC, transverse, T type) - Ilioinguinal: anterior fxs (AW, AC/HT, both columns |
|
|
Acetabular fx H&P |
- Hx: high energy trauma, pain, inability to WB - PE: LE may be malrotated. Inspect skin for Morel-Lavalle lesion. Neuro exam |
|
|
Acetabular fx workup |
- XR: AP pelvis, obturator and iliac obliques (Judet views) are essential. - Roof arc angle: center of head to fx (< 45 degrees is WB) - CT: essential to accurately define fx (size, impaction, articular involvement, LB) and do pre-op planning |
|
|
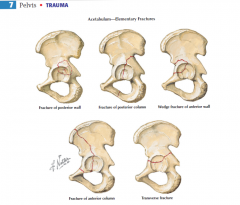
Acetabular fracture classification |
Letournel and Judet |
|
|
Acetabular fracture (Letournel and Judet): Elementary fx's |
- Posterior wall - Posterior column - Anterior wall - Anterior column - Transverse |
|
|
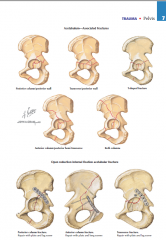
Acetabular fracture: Associated fx's |
- Posterior column and posterior wall - Transverse & posterior wall - T type - Anterior column and posterior hemitransverse - Both columns |
|
|
Non-operative tx for acetabular fracture |
- Reduce hip if dislocated (traction if necessary to maintain reduction) Non-operative: NWB for 12 weeks - < 2mm articular displacement - Roof arc angle > 45 degrees - Posterior wall fx < 20-30% |
|
|
Operative tx of Acetabular fx |
ORIF, NWB 12 weeks - 2 mm articular displacement - posterior wall > 40% - irreducible fx/dx - marginal impaction - loose bodies in hip joint - XRT for HO prophylaxis |
|
|
Acetabular fx complications |
- Post-traumatic arthritis - nerve injury (sciatic nerve) - post surgical (heterotropic ossification) - sciatic nerve injury, bleeding - malunion/non union - infection (associated w/ Morel-Lavalle lesion) - thromboembolism |
|
|
Acetabular fx |
|
|
|
Pelvic ligaments |
|
|
|
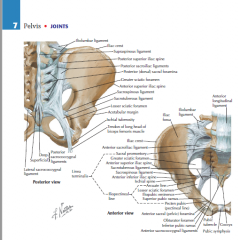
Sacroiliac joint/ligaments |
- Gliding joint, has minimal rotation motion during gait. Should be no vertical motion in normal joint - Vertical stability is essential; the body weight is transmitted through this joint - Articular surface (located inferiorly in articulation) covered w/ sacrum (articular cartilage), ilium (fibrocartilage) |
|
|
Posterior sacroiliac ligament |
- Posterolateral scarum to posteromedial ilium - Strongest in pelvis, key to vertical stability |
|
|
Short sacroiliac ligament |
- Oblique orientation: sacrum to PSIS and PIIS - Resists rotational forces |
|
|
Long sacroiliac ligament |
- vertical orientation: sacrum to PSIS - Resists vertical forces, blends with sacrotuberous ligament |
|
|
Anterior sacroiliac ligament |
- anterior sacrum to anterior ilium - Weaker than posterior, resists rotations forces |
|
|
Interosseous ligament |
- sacrum to ilium - Adds supports to anterior and posterior ligaments |
|
|
Pelvic rotational stability |
- Transverse/horizontal orientation - Short posterior SI, anterior SI, sacrospinous, iliolumnar ligaments |
|
|
Pelvic rotational stability |
- longitudinal/vertical orientation - long posterior SI, sacrotuberous, lumbosacral ligaments |
|
|
Pubic symphysis |
- Anterior articulation of two hemipelves. Articulating surfaces are covered w/ hyaline cartilage - Fibrocartilage disc between two pubic bones in the joint |
|
|
Superior pubic ligament |
- Both pubic bones superiorly and anteriorly - Strongest supporting ligament |
|
|
Arcuate pubic ligament |
- both pubic bones inferiorly - muscle attachments also support inferiorly |
|
|
Sacrospinous ligament |
- Anterolateral sacrum to spinous process - Resists rotation, divides sciatic notches |
|
|
Sacrotuberous ligament |
- posterolateral sacrum to ischial tuberosity - resists vertical forces, provides vertical stability |
|
|
Iliolumbar ligament |
- L4/5 transverse process to psoterior iliac crest - Avulsion fracture sign of unstable pelvic ring injury |
|
|
Lumbosacral ligament |
- L5 transverse process to sacral ala - Anterior support, assists in providing vertical stability |
|
|
Hip pain: young age |
- ankylosis spondylitis |
|
|
Hip pain: middle aged to elderly |
- saroilitis - decreased mobility |
|
|
Acute hip pain |
- Trauma: fx, dislocation, contusion |
|
|
Chronic hip pain |
- systemic inflammatory - degenerative disorder |
|
|
Deep, non specific hip pain |
- sacroiliac etiology - infection - tumor |
|
|
Radiating hip pain |
- to thigh or buttock - SI joint - L spine |
|
|
Pain in/out of bed, or on stairs |
SI etiology |
|
|
Pain adducting legs |
Symphysis pubis etiology |
|
|
Hip pain in pregnancy |
Laxity of ligament in SI joint causes pain |
|
|
Fall on buttock/twist injury |
sacroiliac joint injury |
|
|
High velocity pelvic trauma |
- fracture - pelvic ring disruption |
|
|
Pain while twisting, standing on one leg |
SI etiology |
|
|
Hip pain, numbness, tingling |
Spine or SI etiology |
|
|
Hx of Arthritides |
- SI involvement of RA, Reiter's, ankylosing spondylitis |
|
|
Anteroposterior compression pelvic fracture |
- open book fx - Forceful frontal impact causes anteroposterior compression of pelvis |
|
|
Lateral compression injury |
- caused by forceful blow to side of pelvis |
|
|
Ischial bursitis |
deep pain and tenderness over ischial tuberosity |
|
|
Hip pointer |
palpate iliac crest for tenderness |
|
|
Sacroilitis |
deep pain and tenderness over SI joint |
|
|
Skin inspection of pelvis |
- Discoloration, wounds - recent trauma indication |
|
|
Inspection of ASIS/Iliac crest |
- Both level (same plane) - if on different plane: leg length discrepancy, sacral torsion |
|
|
Lumbar curvature inspection |
- Increased lordosis - flexion contracture - Decreased lordosis - paraspinal muscle spasm |
|
|
Standing palpation of ASIS, pubic/iliac tubercles, PSIS |
- Unequal side to side = pelvic obliquity, leg length discrepancy |
|
|
Lying palpation of iliac crest, ischial tuberosity |
- Hip point/contusion, fx - Ischial bursitis (weaver's bottom) - avulsion fx |
|
|
Palpation of SI joint |
Sacroilitis |
|
|
Palpation of inguinal ligament |
- protruding mass: hernia |
|
|
Palpation of femoral pulse and nodes |
Diminished pulse: vascular injury - palpable nodes : infection |
|
|
Palpation of muscle groups |
Each group should be symmetrical b/l |
|
|
Hip ROM: forward flexion |
- Standing: bend forward - PSIS should elevate slightly |
|
|
Hip ROM: Extension |
- Standing: lean backward - PSIS should depress equally |
|
|
Hip flexion |
- Standing: knee to chest - PSIS should drop but will elevate in hypomobile SI joint - Ischial tuberosity should move laterally, will elevate in hypomobile SI joint |
|
|
Trendelenberg Test |
When weight is on affected side, normal hip drops, indicating weakness of weight baring gluteus medius - trunk shift to weak side as patient attempts to maintain balance |
|
|
Iliohypogastric nerve (L1) sensory |
- suprapubic - lateral butt/thigh |
|
|
Ilioinguinal nerve (L1) sensory |
Inguinal region |
|
|
Genitofemoral nerve sensory |
Scrotum or mons |
|
|
Lateral femoral cutaneous nerve L2-3 Sensory |
Lateral hip/thigh - meralgia paresthetica |
|
|
Pudendal nerve S2-4 sensory |
Perineum |
|
|
Femoral L2-4 Motor |
Hip flexion - iliopsoas weakness |
|
|
Inferior gluteal nerve - motor |
- External rotation - glut maximus weakness |
|
|
Nerve to quadratus femoris - motor |
External rotation - short rotator weakness |
|
|
Superior gluteal nerve - motor |
- Abduction - gluteus medius/minimis weakness |
|
|
Bulbocavernous reflex |
- Finger in rectum - squeeze or pull penis (Foley/clitoris, anal sphincter should contract) |
|
|
Femoral pulses |
Diminished pulses abnormal |
|
|
Pelvic rock |
- push both iliac crests - instability/motion indicates pelvic ring injury |
|
|
SI stress test |
- Press ASIS and iliac crests - Pain in SI could be SI ligament injury |
|
|
Trendelenburg sign |
- Standing: lift one leg (flex hip) - Flexed side: pelvis should elevate, if pelvis falls, abductor or gluteus medius (superior gluteal nerve) dysfunction |
|
|
Patrick (FABER) test |
- Flex, Abduct, ER hip then abduct more - Positive if pain or LE will not continue to abduct below other leg; SI joint pathology |
|
|
Meralgia |
- Pressure to medial ASIS - Reproduction to pain, burning, numbness = LCFN entrapment |
|
|
Rectal and Vaginal exam |
- Especially after trauma - Gross blood indicates trauma communicating with other organs |
|
|
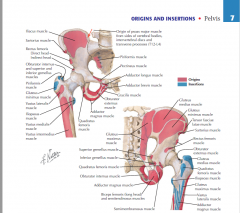
Pelvic muscle origin and insertions |
|
|
|
Pubic Rami Muscle Origins |
- Pectinues - Adductor longus - Adductor brevis - Adductor magnus - Gracilis - Obturator internus - Obturator externus |
|
|
Ischial tuberosity muscle origins |
- Semimembranosus - Semitendinosus - Biceps femoris (LH) - Adductor magnus - Ischium Bone: Quadratus femorus/inferior gemellus |
|
|
Linea Aspera muscle origins |
- Vastus lateralis - Vastus intermedius - Vastus medialis - Biceps femoris (SH) |
|
|
Greater trochanter muscle insertions |
- Gluteus medius (posterior) - Gluteus minimus (anterior) - Quadratus femoris (inferior) - Obturator externus (fossa) - Short external rotators: Piriformis, Superior gemellus, obturator internus, inferior gemellus |
|
|
Linea aspera muscle insertions |
- gluteus maximus - adductor magnus - adductor longus - pectineus |
|
|
Psoas major |
- Origin: T12-L5 - Insertion: Lesser trochanter - Femoral nerve - Flex hip - Covers lumbar plexus |
|
|
Psoas minor |
- Origin: T12-L1 vertebrae - Iliopubic eminence insertion - L1 - ventral ramus - Assists in hip flexion - Weak - present in 50% people |
|
|
Iliacus muscle |
- origin: iliac fossa/sacral ala - insertion: lesser trochanter - femoral nerve - flex hip - Covers anterior ilium |
|
|
Tensor fascia latae |
- origin: iliac crest, ASIS - insertion: Iliotibial band/proximal tibia - Superior gluteal nerve - Abducts, flex, IR thigh - A plane in anterior approach to hip |
|
|
Gluteus medius |
- origin: ilium between anterior and posterior gluteal lines - Greater trochanter (posterior) - Superior gluteal nerve - Abducts, IR thigh - Trendelenberg gait if muscle is out |
|
|
Gluteus minimus |
- origin: ilium between anterior and inferior gluteal lines - insertion: greater trochanter - Superior gluteal nerve - Abducts, IR thigh - Works in conjuction w/ medius |
|
|
Gluteus maximus |
- origin: Ilium, dorsal sacrum - insertion: ischial tuberosity, gluteal tuberosity (Femur) - inferior gluteal nerve - Extend, ER thigh - Must be split in posterior apporach to hip |
|
|
Obturator externus |
- origin: ilium, dorsal sacrum - insertion: trochanteric fossa - Obturator nerve - ER thigh - Inserts at start point for IM nail |
|
|
Piriformis |
- origin: anterior sacrum - insertion: superior greater trochanter - Nerve to piriformis - ER thigh - used as landmark for sciatic nerve |
|
|
Superior gemellus |
- origin: anterior sacrum - insertion: medial greater trochanter - Nerve to obturator internus - ER thigh - Detached in posterior approach to hip |
|
|
Obturator internus |
- Origin: Isciopubic rami, obturator membrane - Insertion: medial greater trochanter - Nerve to obturator internus - ER, abduct thigh - Exits through lesser sciatic foramen |
|
|
Inferior gemellus |
- origin: ischial tuberosity - insertion: medial greater trochanter - N to quadratus femoris - ER thigh - Detached in posterior approach to hip |
|
|
Quadratus femoris |
- origin: ischial tuberosity - insertion: intertrochanteric crest - nerve to quadratus femoris - ER thigh - Ascending branch of medial circumflex artery under muscle |
|
|
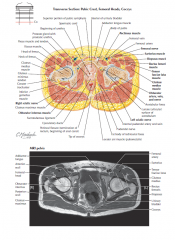
Transverse section of pelvis |
|
|
|
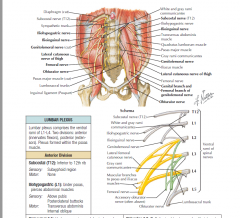
Lumbar plexus |
-comprises the ventral rami of L1-4 - two divisionsL anterior (flexors) and posterior (extensors) - plexus formed within psoas muscle |
|
|
Anterior Lumbar plexus |
- Subcostal T12 - Iliohypogastric L1 - Ilioinguinal L1 - Genitofemoral L1-2 - Obturator L2-4 - Accessory obturator L2-4 |
|
|
Subcostal nerve (T12) |
- Sensory: subxyphoid region - No motor |
|
|
Iliohypogastric nerve (L1) |
- under psoas, pierces abdominal muscles - Sensory: Above pubis, posterolateral buttocks - Motor: Transverse adbominis, internal oblique |
|
|
Ilioinguinal nerve L1 |
- under psoas, pierces abdominal muscles - Sensory: inguinal region, anterosuperior thigh - motor: none |
|
|
Genitofemoral nerve L1-2 |
- pierces psoas lies on anterior surface of psoas muscle - Sensory: scrotum or labia majora - Motor: cremaster |
|
|
Obturator L2-4 |
- exits via obturator canal, splits into ant/post division (can be injured by retractors placed behind transverse acetabular ligament) - Sensory: inferomedial thigh via cutaneous branch of obturator nerve - motor: external oblique, obturator externus |
|
|
Accessory obturator nerve L2--4 |
- inconsistent - sensory: none - motor: psaos |
|
|
Posterior division of lumbar plexus |
- Lateral femoral cutaneous nerve (L2-3) - Femoral nerve L2-4 |
|
|
Lateral femoral cutaneous (FFCN) L2-3 |
- runs on iliacus, crosses inferior to ASIS (can be compressed, meralgia paresthetica) - No motor or sensory in pelvis |
|
|
Femoral nerve L2-4 |
- lies between psoas major and iliacus - Sensory: none in pelvis - Motor: psoas, iliacus, pectinues |
|
|
Lumber plexus anterior |
|
|
|
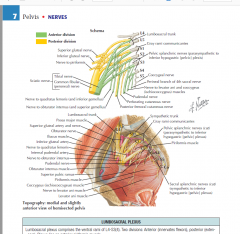
Lumbosacral plexus lateral |
|
|
|
Lumbosacral plexus |
- ventral rami of L4-S4 - Anterior and posterior divisions - plexus lies on anterior piriformis muscle |
|
|
Anterior division of Lumbosacral plexus |
- nerve to quadratus femoris L4-S1 - nerve to obturator internus L5-S2 - Pudendal S2-4 - Nerve to coccygeus S3-4 |
|
|
Nerve to quadratus femoris L4-S1 |
- Exits greater sciatic foramen - sensory: none - motor: quadratus femoria, inferior gemelli |
|
|
Nerve to obturator internus (L5-S2) |
- exits greater sciatic foramen - obturator internus, superior gemelli |
|
|
Pudendal nerve S2-4 |
- exits greater then re enters pelvis through lesser sciatic foramen |
|
|
Pudendal nerve sensory |
- perineum via perineal nerve (scrotal/labial) - perineum via inferior rectal nerve - perinuem via dorsal nerve to penis/clitoris |
|
|
Pudendal nerve motor |
- Bulbospongiosus: perineal nerve - Ischiocavernous: perineal nerve - Urethral spinchter: perineal nerve - Urogenital diaphragm: perineal nerve - Sphincter ani externus: inferior rectal nerve |
|
|
Nerve to coccygeus S3-4 |
- directly innervates muscles - sensory: none - motor: coccygeus and levator ani |
|
|
Lumbosacral plexus - posterior division |
- Superior gluteal nerve L4-S1 - Inferior gluteal nerve L5-S2 - Nerve to piriformis S2 |
|
|
Superior gluteal nerve L4-S1 |
- exits greater sciatic foramen above piriformis - Sensory: none - Motor: gluteus medius/minimus, TFL |
|
|
Inferior gluteal nerve L5-S2 |
- Exits greater sciatic foramen - Sensory: none - motor: gluteus maximus |
|
|
Nerve to piriformis S2 |
- directly innervates muscles - sensory: none - motor: piriformis |
|
|
Lumbosacral plexus - Both divisions |
- Posterior femoral cutaneous nerve S1-3 - Sciatic L4-S3 |
|
|
Posterior femoral cutaneous S1-3 |
- exits via greater sciatic foramen, under piriformis, medial to sciatic nerve - motor: none |
|
|
Posterior femoral cutaneous sensory |
- Inferior buttocks via inferior cluneal nerves - Posterior perineum via perineal branches - Posterior thigh |
|
|
Sciatic nerve L4-S3 |
- Largest nerve in body - Two components: tibial (anterior) and peroneal (post division) - Exits greater sciatic foramen under piriformis - Anatomic variation include exiting through or above piriformis - Reflecting short ER's will protect sciatic in posterior approach to hip |
|
|
Superior cluneal nerve L1-3 |
- branches of dorsal rami - Sensory: superior 2/3 of buttocks |
|
|
Medial cluneal S1-3 |
- branches of dorsal rami - Sacral and medial buttocks |
|
|
Piriformis muscle is the landmark in |
gluteal region - most nerves exit inferior to it |
|
|
POPS IQ |
- Pudendal - N to Obturator internus - Posterior cutaneous - Sciatic - Inferior gluteal - N to Quadratus femoris |
|
|
Common Iliacs |
- Branch at L4, run along anterior spine - Blood supply to pelvis and lower extremity - Branches off aorta |
|
|
Medial sacral artery |
- Descends along anterior spine and sacrum - Anastamoses w/ lateral sacral arteries |
|
|
Branches of common iliac artery |
- internal/external iliac |
|
|
Internal iliac artery |
- under ureter toward sacrum, then divides - Supplies most of pelvis/pelvic organs - divides into anterior/posterior divisions |
|
|
External iliac artery |
- On anterior surface of psoas to inguinal ligament - Does not supply much of pelvis |
|
|
Internal iliac artery: anterior division |
- Obturator artery - Inferior gluteal artery - Umbilical - uterine/vaginal - inferior vesicle (males) - middle rectal - internal pudendal |
|
|
Obturator artery |
- through obturator foramen w/ obturaotr nerve - fovea artery (ligamentum teres) branches - off of internal iliac |
|
|
Inferior gluteal artery |
- off of internal iliac - exits greater sciatic foramen under piriformis - supplies gluteus maximus muscle |
|
|
Umbilical artery |
- off of internal iliac - supplies bladder (via superior vesical arteries) |
|
|
Uterine/vaginal artery (female) |
- supplies uterus and vagina - off of internal iliac |
|
|
Inferior vesicle artery (males |
- off of internal iliac artery - supplies bladder, prostate, ductus deferens |
|
|
Middle rectal artery |
- anastamoses w/ superior/inferior rectal arteries |
|
|
Internal pudendal nerve |
- runs with pudendal nerve - inferior rectal artery branches from inferior pudendal |
|
|
Posterior division of Internal iliac |
- Superior gluteal - iliolumbar - lateral sacral |
|
|
Superior gluteal artery |
- exits greater sciatic foramen above piriformis - in sciatic notch, can be injured in posterior column fractures or pelvic ring fractures |
|
|
Iliolumbar artery |
- runs superiorly toward iliac fossa - supplies ilium, ilacus, psoas muscles |
|
|
Lateral sacral artery |
- runs along sacrum, anterior to sacral rods - supplies sacrum/sacral muscles/nerves - anastamoses w/ median sacral artery off of aorta |
|
|
External Iliac Artery Branches |
- Deep circumflex iliac - inferior epigastric - femoral artery |
|
|
Deep circumflex artery |
- runs laterally under internal oblique to iliac crest - supplies anterolateral abdominal wall muscles |
|
|
Inferior epigastric artery |
- runs superiorly in transversalis fascia - supplies anterior abodminal wall muscles |
|
|
Femoral artery |
- combination of external iliac artery under inguinal ligament - terminal branch of external iliac artery |
|
|
Femoral artery branches
|
- superficial circumflex iliac - superficial epigastric - superficial and deep external pudendal - Profunda femoris - medial circumflex femoral - lateral circumflex femoral |
|
|
superficial circumflex iliac artery |
- in subcutaneous tissues toward ASIS - supplies superficial abdominal tissues |
|
|
Superficial epigastric artery |
- in subcutaneous tissues towards umbilicus - supplies superficial abdominal tissues |
|
|
Superficial and deep external pudendal artery |
- medially over the adductors and spermatic cord to inguinal and genital regions - Supplies subQ tissues in the pubic region and the scrotal/labia majus |
|
|
Profunda femoris (deep artery of thigh) |
- Between adductor longus and pectinues/addcutor brevis - gives off circumflex (2) and perforating branches |
|
|
Medial circumflex femoral artery |
- between pectineus and psoas, then posterior to femoral neck under quadratus femoris - runs under quadratus femoris, can be injured in posterior approach to hip |
|
|
Lateral circumflex femoral artery |
- runs laterally deep to sartorius and rectus - at risk in anterolateral approach |
|
|
Osteitis pubis description |
- inflammation or degeneration of pubic symphysis - etiology: repetitive micro trauma (sports) or fx |
|
|
Osteitis pubis H&P |
- Hx: Anterior pelvic pain, sports or trauma - PE: symphisis pubis is tender to palpation |
|
|
Osteitis pubis workup |
- XR: AP pelvis, +/- inlet and outlet views - CT/MR: not usually needed |
|
|
Osteitis pubis tx |
- activity mod - rest, NSAIDs - Fusion if symptoms are refractory to conservative tx |
|
|
Sacroilitis |
- inflammatory or degeneration of SI joint - infection can occur - associated w/ Reiter's syndrome |
|
|
Sacroilitis H&P |
- Hx: low back pain - PE: SIJ tender to palpation, + FABER test, injection can help diagnosis |
|
|
Sacroilitis workup |
- XR/CT: SI joint, +/- DJD - Bone scan: r/o infection - LABS: CBC, ESR, CRP if infection is suspected |
|
|
Sacroilitis tx |
- Rest, NSAIDs - injection can be diagnostic and therapeutic - fusion rarely indicated |
|
|
Ischial bursitis |
- inflammation of bursa ischial tuberosity - often from prolonged sitting - aka weaver's bottom - mimics hamstring injury |
|
|
Ischial bursitis |
- Hx: buttocks pain, sitting - PE: Ischial tuberosity tender to palpation, active hamstring not painful |
|
|
Ischial bursitis workup |
- XR: pelvis, r/o tuberosity avulsion - MR: can evaluate or r/o hamstring insertion injury |
|
|
Ischial bursitis tx |
- rest - NSAIDs - Activity mod - decrease sitting or increase cushion |
|
|
Iliac crest contusion (hip pointer) |
- direct trauma to iliac crest - common in contact sports |
|
|
Iliac crest contusion H&P |
- Hx: trauma, hip pain - PE: iliac crest tender to palpation |
|
|
Hip Pointer workup |
- Xr: pelvis, r/o fx - MR/CT: usually not necessary for diagnosis |
|
|
Hip pointer tx |
- rest, NSAIDs - padding to iliac crest - corticosteroid injection |
|
|
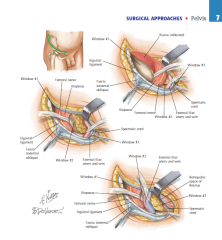
Ilioinguinal surgical approach uses |
- ORIF of acetabular fracture involving anterior column of acetabulum |
|
|
Ilioinguinal surgical approach internervous plane |
3 windows - interval access -Lateral to iliopsoas and femoral nerve (anterior SIJ, iliac fossa, pelvic brim) - Between iliopsoas/femoral nerve and external iliac artery (pelvic brim, lateral superior pubic ramus) - Medial to external iliac artery and spermatic cord (quadrilateral plate and retropubic space) |
|
|
Ilioinguinal surgical approach dangers |
- External iliac vessels - Corona mortis (vessel from obturator artery) - femoral nerve - lateral femoral cutaneous nerve - inferior epigastric artery - spermatic cord - bladder |
|
|
Ilioinguinal surgical approach comments |
- good knowledge of abdominal and pelvic anatomy essential to this approach - must detach pelvic insertion of abdominal muscles and iliacus muscle for exposure - use rubber drains around iliopsoas/femoral nerves and external iliac vessels to access windows |
|
|
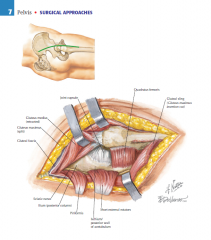
Kocher-Langenbeck surgical approach |
- ORIF of acetabular fracture involving posterior column of acetabulum |
|
|
Kocher- Langenbeck surgical approach internervous plane |
No internervous plane - gluteus maximus (inferior gluteal nerve) fascia is split in line with its fibers (inferior gluteal nerve is limit to the split) - TFL also split in line with its fibers |
|
|
Kocher-Langenbeck surgical approach comments |
- Hetertropic ossification is common, prophylaxis (XRT) is often needed - do not take down quadrtaus femoris due to vascular risk |
|
|
Kocher-Langenbeck surgical approach pic |
|
|
|
Ilioinguinal surgical approach pic |
|