Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
90 Cards in this Set
- Front
- Back
|
Gastroesophageal reflux: 3 mechanisms involving the LES (lower esophageal sphincter)
|
1) Weak basal LES pressure
2) Inadequate LES response to increased abdominal pressure 3) Transient relaxation of the LES without peristalsis |
|
|
Antireflux barrier: Anatomy
|
-lower esophageal sphincter
-crural diaphragm -phrenoesophageal ligament |
|
|
Reflux esophagitis
|
esophageal injury that is due to reflux of acidic gastric contents into the esophagus
|
|
|
Pill-induced esophagitis
|
Caustic injury from lingering in the esophagus
Examples -KCl -FeSO4 -quinidine -NSAIDS -tetracycline |
|
|
Infectious esophagitis (causes, host factors)
|
Causes
-Candida -HSV -CMV Host factor: Immunocompromised |
|
|
Barrett's Esophagus
|
-patch or patches of metaplastic columnar epithelium (specialized intestinal metaplasia) in the lower esophagus, often due to severe reflux esophagitis
-increased prevalence of adenocarcinoma |
|
|
GERD: External factors
|
-Diet (eg high fat foods)
-Smoking -Medication |
|
|
GERD: Mucosal pathophysiology
|
Impaired esophageal mucosal resistance
|
|
|
GERD: Reasons for diminished esophageal clearance
|
-Peristalsis
-Body position -Saliva |
|
|
GERD: Gastric factors
|
-Acid
-Bile acids -Gastric emptying -Gastric distention |
|
|
Heartburn: Indications of severe disease
|
-Age > 40
-Symptoms > 3 years -Alarming symptoms --Dysphagia --Weight loss --Anemia |
|
|
Heartburn: differential diagnosis
|
-Esophagitis
-Stricture -Barrett's esophagus |
|
|
Approach to patient with dysphagia
|
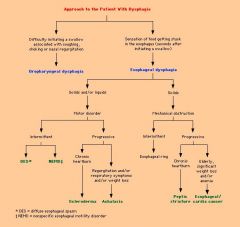
Algorithm image
|
|
|
Spastic esophageal motility disorders: Syndromes
|
-DES (Diffuse esophageal spasm)
-Nutcracker esophagus -Hypertensive LES (lower esophageal sphincter_ -Nonspecific |
|
|
Spastic esophageal motility disorders: Symptoms
|
-Chest pain
-Dysphagia |
|
|
Spastic esophageal motility disorders: Manometric features
|
-Some normal peristalsis
-Contractions (simultaneous/spontaneous/repetitive/high-amplitude) -High LES pressure |
|
|
Achalasia manometry
|
-Incomplete relaxation
-Aperistalsis -Lower esophageal sphincter hypertension |
|
|
Scleroderma manometry
|
-Weak contractions
-LES hypotension |
|
|
Parietal cell function
|
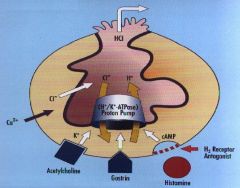
In: Ca, ACh, Gastrin.
Out: HCl |
|
|
Evidence for H. Pylori's role in gastric ulcer
|
1. Colonization precedes ulcer
2. Eradication of H. Pylori ends cycle of recurrent ulcers |
|
|
How are peptic ulcers named?
|
By location:
-Gastric -Duodenal -Esophageal |
|
|
Percentage of ulcers caused by H. Pylori
|
Duodenal: 70% (if not used NSAIDs to excess)
Gastric: 65-95% (45% if NSAID related) |
|
|
Testing for H. Pylori
|
Noninvasive
-serology (rare) -Urease breath test Invasive (biopsy) -rapid urease test –special stains |
|
|
Difference between ulcers in NSAID related disease and H. Pylori related disease
|
NSAIDS: less surrounding inflammation
|
|
|
NSAID related injury: Preventive factors in normals
|
i. mucus
ii. superoxide scavengers in mucosa (e.g. glutathione) iii. bicarbonate iv. high blood supply of stomach (promoting repair and cellular metabolic functions) |
|
|
Risk factors for NSAID-induced damage
|
-history of ulcer disease, dyspepsia, gastritis
-age (lower gastric perfusion) -high/prolonged NSAID dose -corticosteroids -anticoagulants |
|
|
Typical location of gastrinoma
|
Pancreas
|
|
|
Causes of diarrhea
|
-Osmotic-lactose intolerance (High fecal osmotic gap: > 125)
-Malabsorption/fatty -Inflammatory -Secretory (Low fecal osmotic gap: <50) -Altered motility |
|
|
Fecal osmotic gap: calculation
|
290 - 2(Na + K)
|
|
|
Causes of diarrhea by location
|
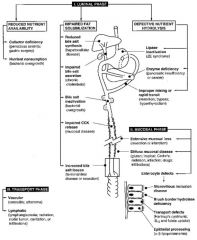
Picture
|
|
|
Celiac Sprue: antibodies
|
-Tissue transglutaminase
-Anti-gliadin -Anti-endomysial |
|
|
Celiac Sprue: MHC
|
HLA-DQ2 associated
|
|
|
Celiac Sprue: Triggers and manifestations
|
Trigger: gluten
Manifestations: -Abdominal symptoms -Malnutrition -Low nutrients (Iron, Vit. D, Vit. K) |
|
|
Ulcerative Colitis: Major features
|
Symptoms: Bloody diarrhea
Inflammation -continuous (no skip lesions) -Rectum involved |
|
|
Crohns Disease: Major features
|
Symptoms:
-Diarrhea (not necessarily bloody) -RLQ pain -Fever -Weight loss Inflammation: -Transmural -Large ulcers -Skip lesions Fistulae and Strictures |
|
|
IBD: Medical Treatment
|
Induce and maintain remission
Drugs: 1) 5-amino-salicylates (inhibit COX and 5-Lipox --> anti-inflammatory) 2) Corticosteroids 3) Antibiotics 4) Immune modulators (6-MP, azathoprine) |
|
|
IBD: Surgical therapy
|
Ulcerative colitis: Total colectomy: curative
Crohn's Disease: Usually recurs after surgery |
|
|
Ulcerative Colitis: Complications
|
Massive hemorrhage
Fulminant colitis Colonic stricture (rare) Colon cancer |
|
|
Crohn's Disease: Complications
|
Bile acid malabsorption
-Secretory diarrhea: bile acids on colon -Gallstones: bile more lithogenic -Steatorrhea: vitamins ADEK malabsorption -Nephrolithiasis: steatorrhea causes more oxalate absorption leading to calcium oxalate stones --- NOT uric acid stones Malignancy: -colon cancer -small bowel cancer (lymphoma or adenocarcinoma – very rare) |
|
|
Benign colon disorders: Differential
|
-Constipation
-Diverticula -Hemorrhoids -Anorectal fistula -Anal fissure |
|
|
Gallstones: Epidemiology
|
-women
-people over age 60 -Native Americans -Mexican Americans -overweight men and women -people who fast or lose a lot of weight quickly -hormonal women |
|
|
Gallstones: Types
|
-Cholesterol stones (90% of US gallstones)
-Pigment stones |
|
|
Gallstones: Cholesterol stone causes
|
-Hypersecretion of cholesterol into bile (Obesity, OCPs, estrogen, rapid weight loss)
-Hyposecretion of bile acids (Impaired synthesis, intestinal loss (t.i.resection), progesterone) -Gallbladder stasis (Progesterone, pregnancy, total parenteral nutrition) |
|
|
Gallstones: Pigment stones
|
Black pigment
–cirrhosis -hemolytic anemia --hemoglobinopathy --red cell disorders Brown pigment -Asian patients (infection) |
|
|
Gallstones: Diagnosis
|
ultrasound
|
|
|
Gallstones: Treatment
|
Laparoscopic cholecystectomy
|
|
|
Gallstones: Symptoms/Manifestations
|
-Asymptomatic (in gallbladder) (75%)
-Intermittent biliary colic (floating in and out of cystic duct) (20%) -Acute pain/cholecystitis (impacted in cystic duct) (10%) -Jaundice/biliary colic (impacted in distal common bile duct) (5%) |
|
|
Pancreatitis: Most common etiologies
|

Image
|
|
|
Pancreatitis: Local effects of enzymes
|
-Inflammation
-Third space losses -Fat necrosis -Pancreatic/peripancreatic necrosis |
|
|
Pancreatitis: Signs and Symptoms
|
-Abdominal pain/tenderness
-Nausea/vomiting -Fever -Tachycardia |
|
|
Pancreatitis: Lab tests
|
-Increased WBC
-Increased serum amylase -Increased serum lipase |
|
|
Pancreatitis: Differential diagnosis
|
-Choledocholithiasis (gallstone in common bile duct)
-Perforated ulcer -Mesenteric ischemia -Intestinal obstruction -Salpingitis -Ectopic pregnancy |
|
|
Chronic Pancreatitis: Most common etiologies
|
Alcohol: 70%
Idiopathic: 12.5% |
|
|
ALT levels: Vary with?
|
-BMI
-Elevated lipids -Glucose |
|
|
High AST/ALT ratio
|
Alcoholic liver disease
|
|
|
Level for AST for 95% chance of hepatocellular liver disease
|
>300 IU
|
|
|
Elevated alkaline phosphatase indicates:
|
1. Liver disease – overproduction of alkaline phosphatase by liver and regurgitation into blood. Highest values in bile duct obstruction and some drug toxicities.
2. Bone disease – overproduction by bone |
|
|
Difference between direct and indirect bilirubin
|
Direct: conjugated with glucouronides. water soluble. excreted in urine
Indirect: unconjugated bilirubin, insoluble in water and not excreted in urine |
|
|
Direct bilirubin: normal
Indirect bilirubin: elevated Bilirubinuria: none |
Increased production: Hemolysis, PA, Thal
Decreased conjugation: Gilbert's syndrome, Crigler-Najjar Syndrome |
|
|
Direct bilirubin: elevated
Indirect bilirubin: elevated Bilirubinuria: positive |
Decreased excretion: All types of liver disease
|
|
|
Normal albumin levels + liver symptoms = ?
|
Possibly acute liver disease
|
|
|
Low albumin levels + liver symptoms = ?
|
Possibly chronic liver diseasse
|
|
|
Prolonged PT (prothrombin time)
|
Vitamin K deficiency: Administer vitamin K and recheck --> if PT normalizes, it's Vit K deficiency
|
|
|
Which coagulation factor is not made in the liver?
|
Factor VIII – made vascular endothelium and R-E cells
|
|
|
Hep A IgM antibody
|
acute infection
|
|
|
Hep A IgG antibody
|
prior infection
|
|
|
Hep B surface Ag: +
Hep B surface Ab: - Hep B core IgM Ab: + Hep B core IgG Ab: - Hep B e Ag: + Hep B e Ab: - HBV-DNA: + |
Acute
(only time Hep B core IgM Ab is positive) |
|
|
Hep B surface Ag: -
Hep B surface Ab: + Hep B core IgM Ab: - Hep B core IgG Ab: + Hep B e Ag: - Hep B e Ab: + HBV-DNA: - |
Resolved acute infection
(Hep B core IgM is negative --> Hep B surface Ab is positive --> Hep B e Ab is positive --> Resolved Acute infection) |
|
|
Hep B surface Ag: -
Hep B surface Ab: + Hep B core IgM Ab: - Hep B core IgG Ab: - Hep B e Ag: - Hep B e Ab: - HBV-DNA: - |
Vaccinated
(Hep B core IgM is negative --> Hep B surface Ab is positive --> Hep B e Ab is negative OR nothing else is positive --> Vaccinated) |
|
|
Hep B surface Ag: +
Hep B surface Ab: - Hep B core IgM Ab: - Hep B core IgG Ab: +/- Hep B e Ag: - Hep B e Ab: + HBV-DNA: - |
Chronic carrier state
(Hep B core IgM is negative --> Hep B surface Ab is negative --> Hep B e Ab is positive --> HBV DNA is negative --> Chronic carrier state) |
|
|
Hep B surface Ag: +
Hep B surface Ab: - Hep B core IgM Ab: - Hep B core IgG Ab: +/- Hep B e Ag: + Hep B e Ab: - HBV-DNA: + |
Chronic active hepatitis
(Hep B core IgM is negative --> Hep B surface Ab is negative --> Hep B e Ab is negative --> Chronic active hepatitis) |
|
|
Hep B surface Ag: +
Hep B surface Ab: - Hep B core IgM Ab: - Hep B core IgG Ab: +/- Hep B e Ag: - Hep B e Ab: + HBV-DNA: - |
Chronic active hepatitis pre-core mutant
(Hep B core IgM is negative --> Hep B surface Ab is negative --> Hep B e Ab is positive --> HBV DNA is positive --> Chronic active hepatitis pre-core mutant) |
|
|
HVPG < 12
|
Normal
|
|
|
HVPG > 12
|
Portal hypertension - Intrahepatic. Due to sinusoidal arteries (due to cirrhosis)
|
|
|
Portal hypertension, Pre-hepatic
|
Portal or splenic vein thrombosis
AV fistulas in the splanchnic bed or spleen |
|
|
Portal hypertension, Intrahepatic, normal HVPG
|
Pre-sinusoidal --> Normal HVPG
Sarcoid, Schistosomiasis Post-sinusoidal --> Budd Chiari – can’t get into hepatic veins (clot in veins) |
|
|
Portal hypertension, Post hepatic
|
Webs in IVC
Cardiac disease --> constrictive pericarditis, right heart failure |
|
|
Complications of cirrhosis
|
Varices
Ascites Hepatic encephalopathy Hepatorenal syndrome |
|
|
Prokinetic Agents - Subbclasses
|
-Cholinergic agents
-Serotonin receptor modulators -Dopamine receptor blockers -Motilin-like agents |
|
|
Drugs for constipation - subclasses
|
-Bulk forming agents
-Softeners/surfactants -Osmotic agents -Stimulants -Miscellaneous |
|
|
Prokinetic agents - Cholinergic agents
|
Bethanechol
|
|
|
Prokinetic agents - Serotonin receptor modulators
|
-Metoclopramide
-Cisapride -Tegaserod |
|
|
Prokinetic agents - Dopamine receptor blockers
|
-Domperidone
-Metoclopramide |
|
|
Constipation drugs - Bulk-forming agents - Toxicities and examples
|
Toxicity
-Bloating Natural -Psyllium (Metamucil) Semi-synthetic -Methylcellulose -Polycarbophil |
|
|
Constipation drugs - Softeners/Surfactants - Mechanism, toxicities and examples
|
Mechanism: Lowers surface tension of stool
Toxicities: -Impaired absorption of fat soluble agents -Oil leakage -Lipid pneumonitis Examples -Docusate -Mineral oil |
|
|
Constipation drugs - Osmotic agents - Mechanism, toxicities and examples
|
Mechanism
-Osmotically-mediated water retention stimulates peristalsis Toxicities -Abdominal distention, flatulence -Saline: caution if renal/cardiovascular disease or electrolyte disorder. Monitor electrolytes. Examples -Saline-based -Sugar/alcohol-alcohol based -Other (PEG solutions) |
|
|
Constipation drugs - Stimulant Laxatives - Mechanism, toxicities and examples
|
Mechanism: Migrating colonic contractions
Concern: Overuse Examples: -Diphenylmethanes -Anthraquinones -Castor oil |
|
|
Constipation drugs - Lubiprostone - Mechanism, toxicities
|
Mechanism: Activates Cl channels within GI tract --> increasing intestinal fluid secretion
Toxicities: Nausea Abdominal distention and pain Diarrhea and flatulence Headache Avoid in pregnancy |
|
|
Anti-diarrheals - Bulk-forming & binding agents - Examples
|
Natural
-Psyllium Semi-synthetic -Methylcellulose -Polycarbophil Other agents -Cholestyramine -Bismuth subsalicylate |
|
|
Anti-diarrheals - classes
|
-Bulk-forming/binding agents
-Antimotility agents -Antisecretory agents -Miscellaneous |