Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
75 Cards in this Set
- Front
- Back
|
Sulfonamides: how do they work
|
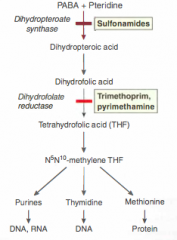
They competitively inhibit DHPsynthase by acting like PABA and binding to the active site. This will cause a drop in DHP which is needed to work with DHFR to make tetrahydrofolate which is needed to make nucleic acids
|
|
|
What is SMX/TMP and how do the active ingredients work
|
Sulfamethoxazole/Trimehtoprim cocktail
Sulfa works by inhibiting DHPsynthase and trimeth works by inhibiting DHFR (DHFR is conserved evo) TMP is more effective at a lower dose and both are bacteriostatic alone...combined they're bactericidal |
|
|
Which bacteria will sulfonamides work on?
|
Gram neg/pos bacteria requiring denovo synth of folic acid. USED MOSTLY FOR GRAM NEGATIVE RODS
UTI: e coli, proteus mirabilis (cystitis, prostatitis) GI: salmonella typhi, shigella spp (diarrhea) RTI: Some Hemophilus influenza (sinusitis), |
|
|
What is Pyrimethamine and what is it used for?
|
Used for Plasmodium and malaria treatment in conjunction with a sulfonamide
This drug itself is not a sulfonamide |
|
|
Mechanism of Resistance Mechanism for SULFA AND TMP
|
SMX: mutation of DHPsynthase or enhanced PABA getting into cell
TMP: mutation of DHFR or overexpression of DHFR |
|
|
Which bacteria are resistant to SMX/TMP
|
CAMPYLOBACTER, p aeruginosa, TB, Bacteroides fragilis and most anerobes, PENICILLIN resistant pneumon, RICKETTSIAE, ENTEROCOCCUS
FOLIC ACID AUXOTROPHS |
|
|
What are main therapeutic usage of SMX/TMP
|
UTI, Treatment/prevention of pneumocystis carinii penumonia (PCP) (Fungal cause of pneumon: pneumocystis jirovecii) for HIV pts
TOXOPLASMOSIS in immunocompromised |
|
|
Adverse Effects of Sulfonamides
|
Kernicterus, hemolytic anemia (especially in pts with inherited G6PD deficiency) due to ox stress causing hemoglobin denaturation and acute hemolysis and red cell loss, stevens johnson syndrome (hypersensitivity), kernicterus (excess bilirubin in brain because you can't get glucuronidation to displace it due to a lack of UGT1A1 in infants)
|
|
|
Trimethoprim Birth Defects
|
Causes birth defects because it will inhibit folate activity and this is required during baby making time. though we get our folate through food, we have some folate synthesis biochemical activity. Cause cardiovascular and oral cleft defects.
|
|
|
Fluoroquinolone mechanisms of action
|
Enter through porins.
Inhibit dna gyrase (topoisomerasae II) (more for gram negative) and topoisomerase IV (more for gram positive) TOPO II for unwinding DNA, TOPO 4 for untying replicated DNA |
|
|
Mechanism of Fluoroquinolone Resistance
|
DNA gyrase mutation/topoisomerase mutation
Cellular membrane efflux mechanism Multidrugresistance and decreased number of porins: channel loss, channel mutation, decreased porin gene expression |
|
|
Usage, names, and bacteria that 1st and 2nd generation fluoroquinolones treat
|
1st gen-Nalidixic Acid-limited spectrum of Activity
2nd gen-Ciprofloxacin (MAIN ONE), (norfloxacin and ofloxacin as secondaries) Cipro used for GRAM NEGATIVE: Mycoplasma, Chlamydia, Mycobacteria, Legionella Cipro used for GRAM + : Bacillus anthracis Cipro for UTI and skin infection and sometime RI SPECIFICALLY for anthrax, osteomyelitis, febrile neutropenia, typhoid fever, and abdominal infections. |
|
|
3rd Generation Fluoroquinolones: what are they, what are they used for, Indications, ETC
|
Levofloxacin (l isomer of ofloxacin)
More active against Mycoplasma, Chlamydia, and Legionella Some activity against Gram Positive Cocci: Strepto pneumoniae USED ESPECIALLY FOR SEPTIC AND PNEUMONIC PLAGUE, PYELONEPHRITIS |
|
|
4th gen Fluoroquinolones: what are they, what are they used for, indications: ETC
|
main one is MOXIFLOXACIN (gemifloxacin is secondary)
Used for Gram Positive Cocci and Bacilli and ANAEROBES USED ALMOST EXCLUSIVELY for respiratory infections Uniquely used for anaerobic intra abdominal infection NO ACTIVITY AGAINST P. aeruginosa |
|
|
Common usages and bacteria affected by 2-4 gen fluoros
|
Enterobacteria, Pseudomonas sp, hemophilius influenza, moraxella catarrhalis
Treatment of osteomyelitis due to gram neg High bone penetration effective against sev organisms causing atypical pneumonia (non gram staining ones) |
|
|
Absorption/administration of fluoros
|
Do not take with antacids, magnesium, aluminum, calcium, vitamin, mineral supplements w/iron or zinc because it will make make it harder to absorb
Cipro comes in oral, IV, topical, and eye/ear drops Levo and Moxi are oral, IV or eye drops Gemi is only oral |
|
|
Clearance of Fluoros
|
Moxi is primarily hepatic clearance
Cipro is primary renal clearance (50) Levo is renal -reason why used for GU |
|
|
Complications with fluoros
|
Connective tissue issues: cartilage erosion and arthropathy in children EXCEPT with EYE and EAR DROPS
Tendon rupture in old pts and in pts with tendonitis PHOTOTOX Prolonged QT interval-blocking of incoming K thru K channels slowing repolarization (from high to low risk: moxi, gemi, levo) Peripheral Neuropathy risk with oral, not eye/ear |
|
|
Aminoglycosides: what's a VERY general description of how they work and some VERY general properties and some VERY general uses
|
Protein Synthesis inhibitors of 30S ribosome
Strong base, positive charge, water soluble Used mostly for empirical therapy (occuring less and less nowadays) and mostly used for specific bacterial infections, zoonotic infections |
|
|
Specific Aminoglycosides: GNATS K
|
gentamicin, neomycin, amikacin, tobramycin, streptomycin, kanamycin
|
|
|
Gentamicin uses and half life: what bacteria and which medical conditions
|
Treatment of ENDOCARDITIS, PERITONITIS, INTRA-ABDOMINAL AND PELVIC FUNCTIONS, SEPTIC STATES
Gram negative aerobes treatment of Tularemia, Brucellosis (with doxycycline combo), Klebsiella (with pipericillin or ticracillin) Use for serious gram negative bacillary infections First AG to be used due to low costs, reliability and long experience of use HALF LIFE OF 2 HOURS |
|
|
Tobramycin: uses and properties
|
Almost used exclusively for P. aeruginosa in combincation with Pipericillin or ticarcilliln
|
|
|
Amikacin: uses and properties
|
Used when you have a resistance to gentamicin
NOT AFFECTED BY INACTIVING ENZYMES use for serious nosocomial gram neg infections withere tobramycin and gentamycin are resisted. EFFECTIVE for TB and atypical mycobacteria in AIDS pts |
|
|
Kanamycin: uses and properties
|
BAD NEPHROTOX AND OTOTOX and therefore used only with TB and topical forms
|
|
|
Neomycin: uses and properties
|
Used for bowel sterilization can also be used topically
Oral-intestinal antiseptic prioer to colonic surg suppressing intestinal folora Used with antibiotics like bacitracin and polymyxin b to treat topical skin or eye infection (combo helps wide spectrum treatment) Cream-used alone or combo therapy with other antibio or corticosteroids for burns, wounds, ulcers |
|
|
Streptomycin: uses and properties
|
USED FOR TB in hospital
Used for plague treatment (combo with doxycycline) (plague is called yersinia pestis) |
|
|
Spectrum of coverage of AMGs
|
aerobic Gram neg bacilli
WHEN USED WITH A COMPLEMENTARY AGENT (SUCH AS A CELL WALL INHIBITOR), CAN EXTEND TO GRAM POSITIVE COCCI |
|
|
Clinical Indications of AMG: empirical and direct
|
Empirical usages with rapid bactericidal activity with dose limited to 48 hr and with combo of cell wall inhibitor (b lactam or vancomycin)
AG have low levels of resistance (hospital gram neg pathogens) Direct therapy: antibiotic for gram negative infection resistant to safer antimicrobials (what does this mean?) Combo therapy used for p. aeruginosa, brucellosis, tulaermia, and the plague Synergistic treatment with cell wall inhibitor (blacatam) for strepto and enterococcal endocarditis. Oral neomycin for bowel sterilization before bowel surg or colonoscopy (works because AMG are highly polar and poorly absorbed) (usually oral to reduce hepatic tox) |
|
|
Mechanism of Action for AMG
|

1. Passive diffusion through porins
2. O2 dependent active transport to cytosol via O2 dependent active transporter on inner membrane 3. Binding to 30S subunit (binds irreversibly and distorts rRNA/mRNA interaction to the poitn where you don't get a proper anticodon set. This causes wrong AA to insert making the bacteria dyslexic and creating bactericidal and post antibiotic effect) 4. Disrupt Protein Synthesis (reading errors) Irreversible binding and residual bactericidal activity present even after drug is cleared Will produce aberrant proteins caused by misreading and premature termination of mRNA at ribosome which favor bacteria cell death |
|
|
Mechanism of Drug Resistance for AMGs
|
1. Depletion or deficit of porin
2. O2 Deficit/Anerobic Organism (like facultative bacteria in an anaerobic environment) (Gram+clostridia Gram-Bacteroides/fusobacteria) 3. Enzyme alteration of AMG impairing AMG binding to 30s or ability to enter cell (acetylation-less h20 soluble, phosporylation-distort ribosomebinding/porinentry, adenylation-make less water soluble) 4. Mutation of 30s ribosome |
|
|
Dosing of AMG
|

Daily dose usually admin as a single injection (IM injection) with less toxicity and equal efficacy as multi dose
YOU'D RATHER HAVE A HIGH CONCENTRATION THAN LOWER MORE FREQUENT DOSES |
|
|
Absorption and elimination of AMG
|
Rapid with peak plasma in 60-90 min
does not cross BBBarrier Doesn't penetrate eye Elimination via glomerular filtration with half life of 2-3 hrs Accumulation in Renal cortex and inner ear perilymph |
|
|
Toxicity of AMG and Risk factors and how to manage neuromuscular risk
|
Nephrotoxicity and Ototoxicity/Vestibular TOX (8th cran nerve effects and accumulation occurs due to pH diff)
Ototox/vestitox will damage hair cells, can cause hearing loss, and physical instability and damage to vestibular nerve Risk factors for nephrotox-low bp, loop diuretics like furosemide, old age, use of other nephrotox agens like cyclosporin in transplate pts or amphotericin in severe fungal infections Fetal exposure-AMG accumulating in fetal plasma/amniotic fluid. (strepto and tobramycin can cause deafness in children during preg and gentamycin cause renal damage Neuromuscular blockade with highest risk during intrapleural/intraperitoneal admin, large dose, rapid iv infusion (can cause resp arrest, aggravate/reveal MG or cause transient myasthenia syndrome----managed with neostigmine or ventilator |
|
|
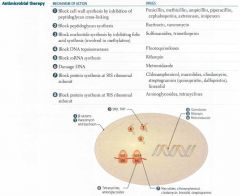
GENERAL PNEUMONICS AND SMALL CHART FOR MECH/CLINCIAL USE/TOX/RESISTANCE
|

see picture
|
|
|
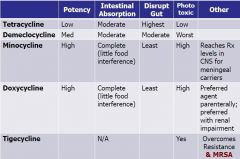
Tetracyclines: Mechanism of Actions
|
Protein synthesis inhibitor on 30s rRNA
1. Passive diffusion into Bacterial Cytosol 2. Bind to 30S rUnit 3. Block Binding of Aminoacyl tRNA 4. Inhibit prot synth 5. Exert Bacteriostatic effect which is reversible unlike AMG |
|
|
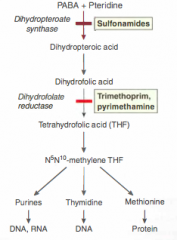
CHART OF TETRACYCLINES with potency, absorption, disruption of gut, phototox, others
PNEUMONIC OF TETRA: it's a palindrome from lowestpot/highest disruption to highestpot/lowestdisruption |
TDMDT
tetracycline, demeclocycline, minocycline, doxycycline, tigecyline |
|
|
tetracyline (specific drug) properties
|
low potency but disrupts the gut more than any other organ
|
|
|
Demeclocycline properties
|
medium potency and most phototoxic
|
|
|
minocycline properties
|
high potency and can reach therapeutic levels CNS for meningeal carriers and HIGH phototox
|
|
|
doxycycline properties
|
high potency and perferred parenteral agent especially during renal impairment with high levels of phototox
|
|
|
tigecycline
|
ONLY USED WHEN ABSOLUTELY NECESSARY TO PREVENT RESISTANCE TO THIS NEWER DRUG
Highest potency, least gut disruption Considered a Glycylcycline overcomes resistance and MRSA Structural modification to minocycline which improves spectrum of activity No drug interactions Use biliary excretion so is safe in pt with renal impariment Decreased susceptibility to TetA efflux pump and ribosomal protection Works on gram positive aerobes including MRSA and VRE (vancomycin resistant enterococci) and gram negative bacteria and anaerobes including c perfringens and bacteriodes sp. |
|
|
Spectrum of Activity for Tetracyclines
|
Broad Spec: gram negative bacteria, atypical organisms, intracellular organisms, gram positive and negative myccoplasma and ricketsia
|
|
|
Treatment Indications for Tetracyclines (mostly doxycycline)
|
Rickettsia (intracellular)-tick bornw infection causing rocky mountain fever, q fever, and typhus
Borrelia Burgdorferi-tick born infection causing lymeD Chlamydia trachomatis-STD causing urethritis, PID, lymphogranuloma venereum Chlamydia psittaci- causes psittacosis pneumonia Mycoplasma-causing pneumonia in Young adults and ppl living in close quarters vibrio cholera-cholera (single dose of doxy to treat) Brucellosis, tularemia, and plauge-combo cocktail with gentamicin for brucellosis and tularemia or cocktail with strepto for plague |
|
|
tetracylines mechanism of action in a picture form
|
|
|
|
Resistance Mech for TETRACYCLINES
|
1. TetA efflux pump-pumps tetracyclines out of cell allowing ribo to stay intact
2. Ribosomal protection - via methylation of ribosome- can be mediated by a chromosome or plasmid encoding for a protecting prot |
|
|
Absorption of Tetracyclines
|
Good entry to most fluids and compartments
TET can enter placenta and CNS (usually CNS levels don't get high enough for tox or probs) Minocycline can reach therapeutic levels in CNS Any antacids, magnesium, calcium, dairies will chelate tet and not cause proper absorption |
|
|
Metabolism and excretion of Tetracyclines
|
Phase 2 conjugation produces glucuronide metabolites....metabolism occurs in the liver and excretion occurs via biliary mechanism
it can also be cleared somewhat renaly with the exception of Doxycycline which is the only TET safe to use in renal impaired people (almost entirely biliary cleared) |
|
|
Adverse Effects of Tetracyclines on GI
|
GI DISTURBANCE-irritiate mucosa and case epigastric distress
Super infection by disrupting commensal flora of gut and causing pathogenic organisms to thrive causing a SUPER infection: C difficile thrives causing psuedomembranous colitis which can be life threat----treated by metronidazole first, vancomycin second, or fidaxomicin when c difficile is ICU acquired. metronidazole-damages DNA via reductive metabolism |
|
|
Other Adverse Effects of Tetracyclines
|
Disulfiram like reaction: severe symptoms like with intake of alcohol and medication: abdominal distress vomiting flushing headache alcohol withdrawal symptoms: Accumulate acid aldehyde instead of acetic acid and will make you sick as a dog
Accumulation in teeth and bone causing discoloration due to calcium chelation. FATAL HEPATOTOXICITY- TETs concentrate in liver and can also disrupt mitochrondrial processes leading to excess lipid production. Fatty liver deposition in pregnancy leading to fatal hepatitis SHOULD NOT BE USED WITH PREG and BREAST FEEDING Phototox Vestibular issues Diabetes Insipidus by demeclocyline |
|
|
IMAGE OF A COMPREHENSIVE ANTIMICROBIAL THERAPY REVIEW
|
|
|
|
How do macrolides and Ketolides work?
|
Binding to bacterial 50S ribosomes
|
|
|
Names of Macrolides
|
Erythromycin, Clarithryomycin, Azithromycin
|
|
|
Erythromycin: description/properties
|
Acid Labile, poor oral absorption (esters of it are absorbed well), used in patients with penicillin allergy
Acts mainly on gram positive cocci and TREPONEMA PALLIDUM (SYPHILLIS) |
|
|
Clarithromycin: description/properties
|
Intestinally absorbed and has an active metabolite allowing for a longer effect (HALF LIFE OF 3-4 HRS)
Acts on same bacteria as erythromycin: gram positive cocci...also acts on gram negative COCCI bacteria and Chlamydia, legionella, pneumophila, moraxella |
|
|
Azithromycin: description and properties
|
Intestinally absorbed which highly active metabolites (HALF LIFE OF 40 HOURS)
Extended activity over clarithro and erythro to include more gram negative cocci: DRUG OF CHOICE FOR LEGIONNAIRES DISEASE least number of drug drug interactions USED ONCE DAILY FOR 5 days being as effective as a 10 day regimen of other macs: MORE COMPLICANCE |
|
|
Which drugs make up Ketolides and is this drugs general properties/description?
|
Telithromycin: intestinally absorbed, active metabolite for longer effect (half life of 10 hours)
Used for multidrug resistant S. Pneumonia |
|
|
Clinical indications of Macs and Ketos
|
Active against many Gram Postive organisms including S Aureus but not MRSA
Active against Group ABCG streptococcus Used heavily for upper resp tract inf (particularly CAP) because they will distribute/concentrate in lung tissue and phagocytic cells, lung tissue. (serum concentrations that is lower than concentration in epithelial lining, alveolar macrophages) SPECIFIC PATHOGENS: S pneumonia, H influenza, Moraxella, Legionella, Chlamydophila, mycoplasma |
|
|
Mechanism of Action for Ketolides and Macrolides
|
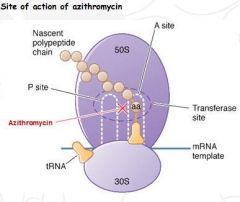
1. Binds IRREVERSIBLE to 50S subunit and inhibit translocation step of prot synth (bacteriostatic manner)
2. Stops the ribosome from getting RATCHET 3. Growing peptide cannot be moved along ribosome for the next rTNA to roll thru |
|
|
Mechanisms of Resistance for Macrolides and Ketolides
|
Cross resistance for Macs are high b/c of drug similarities
1. Methylation of ribosomes- methylases encoded via ERM A/B/C genes alter macrolides (erm-erythromycin ribosome methylase) VERY COMMON METHOD OF RESISTANCE 2. Macrolide efflux pumps, just like TetA pumps but prefer macs...encoded by Macrolife Efflux Genes (mef E). Enterobacteriaceae, Pseudomonas, Acinetobacter are intrinsically resistant due to decreased perm of outer envelope |
|
|
Adverse effects of Macs/Ketos (see another note card for drug drug interactions)
|
Reversible Hearing loss
Nausea, vomitting, diarrhea (time spent in GI tract determines this) Hepatotox-rare, but serious: 1.Cholestatic jaundice caused by hypersensitivity to Erythromycin Estolate 2. Fatal hepatotoxicity caused by Telithroymycin Cardiac tox: can cause PROLONGED QT interval (esp complicated in pts with long qt syndrome) because macs and ketos can block inward rectifying K channel ORDER of worse to least side effects: Erythro, Clarithro, Azithro |
|
|
Drug Drug Interactions with Macs and Ketos and pregnancy usage
|
Macs and Ketos interact with CYP3A
Erythro and Clarithro have interactions related to inhibition of hepatic CYP3A enzymes: NOT AZITHRO Pts who are on drugs that inhibit CYP3A enzymes are at a five fold increase risk of SUDDEN CARDIAC death Erythro and Azithro are CLASS B: safe for preggos in contrary to Tetracyclines |
|
|
Great chart for Macrolides including a PNEUMONIC!
|

|
|
|
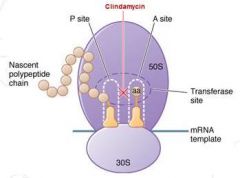
Clindamycin: what type of drug is it considered and general properties
|
IS A LINCOSAMIDE
similar to erythromycin in terms of mech of action, mech of resistance, and efficacy against nonenteric gram positive cocci |
|
|
Anti Microbial Spectrum of Clindamycin
|
UNLIKE EYRTHRO: used primarily in clinical settings for ANAEROBES, mostly for those associated with abdominal anaerobic infections from trauma like bacteroides fragilis
|
|
|
Adverse Effects of Clindamycin
|
Increased risk for pseudomembranous colitis because of activity in gut (overgrowth of c difficile) (can be treated via metronidazole, vancomycin, or (fidaxomycin-ICU acquired PC))
|
|
|
Mech of Action of Clindamycin
|
|
|
|
Small Chart for Clindamycin
|

|
|
|
Chloramphenicol: general properties
|
Considered a broad spec antibiotic with limited clinical use...wide range of gram positive and negative organism
RESTRICTED USE for life threatening infections with no alternatives such as meningitis infection because of ability to cross BBB |
|
|
Adverse effects of Chloramphenicol
|
Lethal side effects
Aplastic anemia:rare/idiosyncratic-individuals with G6PD def have tendency to put stress on RBC causing hemolytic anemia Gray baby syndrome: b/c chloramp penetrates human cells and disrupts mitochondrial prot synth: abdominal distension, diarrhea, vomitting, dusky gray color which can lead to circulatory collapse and death . Syndrome is drug concentration dependent and caused by IMPAIRED GLUCURONIDATION AND RENAL CLEARANCE IN INFANTS (30 DAYS FOR RENAL CLR TO DEV AND 60 DAYS FOR GLUCURON TO DEV) |
|
|
Mechanism of Action and resistance of Chloramphenicol (checccck out the pic here)
|

Binds to 50s subunit inhibiting peptidyl transferase step of prot synthesis in a bacteriostatic fashion. Also has ability to enter host cell impairing mitochondiral prot synthesis enabling toxicity
Resistance: enzymatic modif of Acetyltransferase (CAT) acetylates two hydroxyl groups causing drug to be less active and reduce binding to 50s |
|
|
Chloro Chart
|

|
|
|
Linezolid: what kind of drug is it considered and general properties
|
Considered a OXAZOLIDINONE and used in instances of bacterial resistance
In penicillin resistant S. aureus, use Isoxazole Penicillins, in methicillin resistant S. aureus, use Vancomycin, in vancomycin resistant S. aureus/enterococci (VRSA/VRE) use Linezolid |
|
|
Mech of Action for Linezolid
|
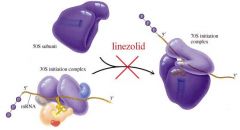
Bacteriostatic protein synthesis inhibitor
binds to 50s ribosome and interferes with its binding to initiation complex |
|
|
Linezolid Clearance and Toxicity
|
Does not induce CYP450, inhibit, or act as substrate for CYP450
Cleared renally With long term use: increased ALT (alanine aminotransferase) decreased platelet count, interaction with MAO (monoamine oxidase) which can lead to peripheral neuropathy |
|
|
GREAT REVIEW SLIDE OF PROTEIN SYNTH INHIBITOR
ALSO GREAT PNEUMONIC |

|