![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
422 Cards in this Set
- Front
- Back
|
Highlights section |
contains most important prescribing information |
|
|
table of contents section |
reference area for the location of detailed or specific prescribing information |
|
|
indications and usage section |
lists disease states/conditions the medication is approved to treat |
|
|
dosage and administration section |
contains recommended doses, dosing schedules, and administration requirements |
|
|
contraindications section |
lists situations when the medication should not be used
|
|
|
warning and precautions section |
lists situations that require caution while taking the medication |
|
|
adverse reactions section |
lists reported side effects |
|
|
drug interactions section |
lists the most significant drug-drug interactions involving the medication |
|
|
use in specific populations section |
lists safety concerns when using the drug during pregnancy, labor and delivery, while breastfeeding, in children, and in the elderly |
|
|
drug abuse and dependence section |
lists the medications controlled substance classification, and the abuse and tolerance potential of the drug if aplicable |
|
|
overdosage section |
lists the signs/symptoms and treatment options during an overdose situation |
|
|
product description section |
lists the chemical name of the medication, a structural diagram of the medication, active ingredients, and inactive ingredients |
|
|
clinical pharmacology section |
contains information on how the medication works, and how the medication is absorbed, metabolized, and eliminated from the body |
|
|
nonclinical toxicology section |
lists any cancer and fertility risks from using the medication |
|
|
clinical studies section |
provides information from the clinical studies showing how well the drug works for its approved indications |
|
|
how supplied sections |
lists the medication's dosage forms, description by color, shape, and markings, and any special storage and handling instructions |
|
|
patient counseling information section |
highlights the most important counseling points about the medication for the pharmacists or prescriber |
|
|
Approved Products with Therapeutic Equivalence Evaluations |
aka orange book, created by fda; maintained electronically, used by many states to guide substitution with generic medications, contains ratings that show whether brand and generic drugs are therapeutically equivalent (e.g. AB-rated) |
|
|
Drug Facts and Comparisons |
contains dispensing and prescribing information; available in print and electronic forms |
|
|
Physicians' Desk Reference (PDR) |
contains a compilation of package inserts; drug manufacturers pay to have package insert in publication; available in print and electronic forms |
|
|
United States Pharmacopeia-National Formulary (USP-NF) |
defines the standards for medications; good reference for compounding medications |
|
|
Trissel's Handbook on Injectable Drugs |
contains information about the administration, preparation, stability, and compatibility of parenteral (injectable) medications |
|
|
Natural Medicines Comprehensive Database |
contains comprehensive, up-to-date information on dietary supplements, vitamins, minerals, and natural remedies; available in print and electronic forms |
|
|
Ident-A-Drug |
contains information to identify medications by imprint codes, NDC numbers, descriptions (color, dosage form, etc); available in print and electronic forms
|
|
|
National Pharmacy Technician Organizations |
Provides resources for advancing the role of pharmacy technicians; promote safe medication use processes. Includes National Pharmacy Technician Association (NPTA) and American Association of Pharmacy Technicians (AAPT) |
|
|
National Pharmacy Organizations |
Provide resources for pharmacy technicians and pharmacists; improve the pharmacy profession and patient care/safety. Includes American Society of Health-System Pharmacists (ASHP) and American Pharmacists Association (APhA) |
|
|
Other Pharmacy Organizations |
Practice-related organizations include National Community Pharmacists Association (NCPA) and National Association of Chain Drug Stores (NACDS). State organizations provide resources to help pharmacists and pharmacy technicians become better healthcare professionals |
|
|
Food and Drug Administration (FDA) |
Governing body over medications sold in US. Branch of US Department of Health and Human Services. Responsible for approval of prescription and over-the-counter medications, drug labeling, and standards for drug manufacturing. |
|
|
Centers for Disease Control and Prevention (CDC) |
Provides regulation for infection control. Publishes annual vaccination and immunization requirements for children, adolescents, and adults. |
|
|
Drug Enforcement Agency (DEA) |
Enforce the laws and regulations surrounding controlled substances and illegal substances. Sets requirements for dispensing controlled substances, refills allowed, and product classifications. |
|
|
The Pure Food and Drug Act of 1906 (Federal) |
First law to regulate medications. Prohibits falsely labeling pharmaceutical products (misbranding). Prohibits sale of contaminated products or those with unknown contents (adulteration). |
|
|
Food, Drug, and Cosmetic Act of 1938 (Federal) |
Created amendments to Pure Food and Drug Act of 1906. Expanded role of FDA (e.g. authority to approve or deny new drugs coming on the market). Addresses safety concerns (e.g. pharmaceutical manufacturers must prove a drug's purity, strength, and safety BEFORE it can be sold). |
|
|
Durham-Humphrey Amendment of 1951 (Federal) |
Created 2 classes of medications: prescription (legend) and non-prescription (OTC) |
|
|
The Poison Prevention Packaging Act of 1970 (Federal) |
Authorizes the Consumer Product Safety Commission to create standards for packaging to protect children from taking harmful meds. Child-resistant containers. Exceptions include sublingual nitroglycerin, oral contraceptives, hormone treatments, inhalers, and drugs dispensed in an inpatient/nursing home setting. Patients must fill out an authorization form to receive non-child resistant packaging for all meds (not including exceptions). |
|
|
Patient Package Insert Legislation (Federal) |
Abbreviated, easy-to-read packet that contains information on benefits and risks of using medication. Required for oral contraceptives and any estrogen-containing products. Outpatient prescriptions: must be dispensed with each new and refill order. Inpatient orders: must be dispensed before the first dose of medication is administered, and then every 30 days. |
|
|
NDC number |
National drug code, 10 digit codes divided into 3 segments. First section identifies the manufacturer/distributor, middle section identifies the name/strength/dosage form of product, last section identifies size/type of packaging. Numbers in each segment can vary. NDCs with 11-digits contain a placeholder (leading) zero or asterisk. |
|
|
Drug Listing Act of 1972 (Federal) |
Requires each new drug to have a national drug code (NDC). NDCs are 10-digit codes divided into 3 segments. Numbers in each segment can vary. NDCs with 11-digits contain a placeholder (leading) zero or asterisk. |
|
|
Drug Price Competition and Patent Term Restoration Act of 1984 (Hatch-Waxman Act) (Federal) |
Allows manufacturers to submit abbreviated new drug applications (ANDA) for generic medications. Must prove generic product is safe and effective, and performs like the brand-name product. Generic drugs can reach the market faster. |
|
|
Omnibus Reconciliation Act of 1990 (OBRA '90) (Federal) |
Requires the pharmacist to discuss information about new and refill prescriptions with patients. State laws vary regarding pharmacist counseling requirements and offering patients pharmacist counseling. |
|
|
Dietary Supplement Health and Education Act of 1994 (DSHEA) (Federal) |
Requires dietary supplements to be treated more like drugs than foods. Dietary supplements include vitamins, minerals, and herbals. Dietary supplements must be safe for people to use. Dietary supplement labels can only say the intended effect on the body. |
|
|
Imprint Code Legislation (Federal) |
Solid, oral dosage forms must have a marking or imprint code on the face of the product. Help identify individual meds, misfilled orders, and counterfeit drugs. |
|
|
Health Insurance Portability and Accountability Act of 1996 (HIPAA) (Federal) |
Protect the privacy of patient information. PHI (protected health information). Use and disclose the minimum necessary amount of protected information. Establish the rights of patients to approve who has access and use of their medication information. HIPAA Security Rule sets standards for ensuring patient information is protected and safe and unauthorized individuals don't have access. |
|
|
Medication Guide Legislation (Federal) |
FDA-approved patient education handouts that inform patients about significant risks of using a medication. MedGuides are different from patient package inserts and written patient information. |
|
|
MedGuide is required if one or more of the following exists: |
Patient labeling could help prevent serious adverse effects. The drug product has serious risks of which the patients should be made aware because information concerning the risks could affect the patient's decision to use, or to continue to use the product. The drug product is important to health and patient adherence to directions for use is crucial to the drug's effectiveness. |
|
|
MedGuide standards: |
Contain specific, comprehensive, scientifically accurate information based off of package insert. Be written in non-technical English. Identify that is is a "Medication Guide" with the name and phonetic spelling of the drug. Contain certain headings and clear explanations. |
|
|
MedGuide must be dispensed: |
When a pt or pt's caregiver asks for a MedGuide, in both outpt and inpt settings. With all outpt presciptions, including new and refill orders (includes retail pharms, outpt clinics, dialysis cneters, and infusion centers). When the first dose of a medication is dispensed in an outpt setting that is to be administered by another health care provider. When the MedGuide is part of a Risk Evaluation and Mitigation Strategies or REMs, program. |
|
|
Board of Pharmacy (BOP) |
Functions to protect the health, safety, and welfare of patients. |
|
|
State Law and Regulations |
Pertain to practice of pharmacy. State law may be more restrictive than federal law. Always follow the stricter law. |
|
|
Drug Approval Process |
Identifying drug compound, preclinical testing, investigational drugs, phase I clinical trials, phase II clinical trials, phase III clinical trials, new drug, phase IV testing |
|
|
Preclinical testing |
testing in animals. determine if drug is safe for human use and potential pharmacologic use. |
|
|
Investigational Drugs |
after preclinical testing, pharmaceutical company must file an investigational drug application (IND) with FDA. When IND is approved, compound becomes an investigation drug and can be tested in humans. Meds require special recordkeeping and dispensing procedures. |
|
|
Phase I Clinical Trials |
after investigational drugs. involves small number of healthy volunteers (20-80 people). volunteers are given small doses of drug compound to determine safety. help investigators determine the drug's therapeutic dose. |
|
|
Phase II Clinical Trials |
after Phase I. involves patients who have the disease the drug is intended to treat (100-300 people). the goal is to determine the drug's efficacy, dose, dosing interval, and method of drug delivery. |
|
|
Phase III Clinical Trials |
after Phase II. involves large number of patients who have the disease the drug is intended to treat (1000-5000 people). the goal is to determine safety and efficacy, including the drug's benefit vs. ratio risk, side effects, drug interactions, and use in special populations. |
|
|
New Drug |
after Phase III. after clinical testing, pharmaceutical company must file a new drug application (NDA) with FDA. When NDA is approved, compound can come to market (process can take months to years for approval). |
|
|
Phase IV Testing |
after new drug. Post-marketing testing period. goals is to monitor drug's safety. pharmaceutical companies required to report any serious or unexpected adverse reactions to FDA. |
|
|
Drug Recalls and Withdrawals |
If a drug product is causing, or has the potential to cause, adverse events, it may be withdrawn from the market. recall can be temporary or permanent. most recalls are voluntary, but FDA can request or require drug removal. may involve specific lot or entire batch of drug. |
|
|
Class I Recall |
Involve products that are likely to cause serious or adverse events or death in people that take the drug.
often involves dietary supplements. |
|
|
Class II Recall |
involve products that could cause temporary but reversible side effects. there is little chance of serious adverse event in people who take the drug. most common type of drug recall. |
|
|
Class III Recall |
involve products or specific batches or lots that are unlikely to cause adverse events in people who take the drug. packaging issues or labeling mix-ups. |
|
|
Market Withdrawal |
drug may be removed if found to be harmful or unapproved. |
|
|
Brand Medications |
new drugs come to market under a protected (patented) brand name. gives innovator exclusive rights for about 20 years. when patent expires, generic versions of med can come to market. |
|
|
Generic Medications |
manufacturers must submit abbreviated new drug application (ANDA) to FDA. When ANDA is approved, generic version of brand-name products can come to market. |
|
|
Pharmaceutical Equivalents |
generic medication must be identical in active ingredients, strength, and dosage form to brand-name drug. |
|
|
Therapeutic Equivalents |
generic is pharmaceutically equivalent and bioequivalent (absorbs and releases the same in the body) to the brand-name drug. same clinical effect and safety profile. |
|
|
Approved Drug Products with Therapeutic Equivalence Evaluations |
aka orange book.
therapeutic equivalence (TE) codes to guide substitution. first letter tells you if product is therapeutic equivalent. second letter tells you additional information about product. number after TE code tells you that meds with the same active ingredient are therapeutically equivalent to different brand name drugs. |
|
|
First letter in TE codes |
The first letter tells you if a product is a therapeutic equivalent. If first letter is an A, products are therapeutic equivalents. If first letter is a B, products are NOT therapeutic equivalents. |
|
|
Second letter in TE codes |
The second letter tells you additional information about product. |
|
|
TE code AB |
means products meet necessary equivalency requirements. |
|
|
TE code AA |
means oral dosage forms are therapeutically equivalent. |
|
|
TE code AN |
means solutions or powers for aerosolization are therapeutically equivalent. |
|
|
TE code AP |
means injectable aqueous solutions are therapeutically equivalent. |
|
|
TE code AT |
means topical meds are therapeutically equivalent. |
|
|
TE code BX |
means products don't meet therapeutically equivalency requirements. |
|
|
TE code BC |
means no therapeutic equivalent extended-release dosage forms |
|
|
TE code BN |
means no therapeutic equivalent solutions or power for aerosolization |
|
|
TE code BP |
means no therapeutic equivalent parenteral (injectable) products |
|
|
TE code BT |
means no therapeutic equivalent topical products |
|
|
Number after TE code |
tells you that medications with the same active ingredient are therapeutically equivalent to different brand name drugs. e.g. AB1, AB2, AB3, AB4 |
|
|
Inactive ingredients |
color, flavor, fillers, etc. can be different from brand name product as long as drug activity, efficacy, and safety do not change. helps lessen confusion and mix-ups between brand and generic medications |
|
|
authorized generics |
brand name product is relabeled and marketed under generic product name |
|
|
Pharmacologic alternatives |
same active ingredient different dosage form or strength |
|
|
therapeutic alternatives |
different active ingredient similar to prescribed product (same drug class, similar drug class, etc) |
|
|
substituting with alternatives |
hospital setting, doesn't usually require prescriber approval; pharmacy follows formulary in most cases. retail setting, usually requires prescriber approval; exception if state laws allows pharmacist to determine product substitution or is pharmacist and presciber have set up a collaborative agreement. |
|
|
DAW codes |
nationally recognized code set that is transmitted with pharmacy claim to insurer/third-party payor. explains if a special circumstance exists that affects product selection. |
|
|
DAW 0 |
no product selection preferred. can substitute with a generic equivalent. |
|
|
DAW 1 |
substitution not allowed by the prescriber. state law may require specific wording be on the face of the prescription (e.g. brand medically necessary, dispense as written, brand only, etc) |
|
|
DAW 2 |
substitution not allowed by the patient |
|
|
DAW 3 |
substitution not allowed by the pharmacist. happens when product is available from multiple sources. |
|
|
DAW 4 |
substitution not allowed because the generic drug is not in stock. based on the pharmacy's buying habits and inventory. |
|
|
DAW 5 |
brand name is dispensed as the generic. happens when there are multiple brands for a generic medication |
|
|
DAW 6 |
override is required. rarely used. |
|
|
DAW 7 |
substitution is not allowed by the state. if brand name drug is written on the prescription, the generic equivalent cannot be dispensed, the brand name product must be dispensed |
|
|
DAW 8 |
substitution not allowed because the generic drug is not available in the marketplace. happens when drug isn't manufactured/distributed or is temporarily unavailable. |
|
|
DAW 9 |
other. reserved and currently not in use. |
|
|
Controlled Substance Act (CSA) |
purpose of CSA: dictates specifics for manufacturing, prescribing, and dispensing controlled substances. prevent diversion and abuse of controlled substances. |
|
|
Drug Enforcement Administration (DEA) |
federal agency governing the enforcement of CSA and other regulations surrounding controlled substances |
|
|
Controlled substance scheduling |
5 schedules: I, II, II, IV, V. depends on the drug's abuse potential, any history of abuse and current pattern of abuse from using med, significance of abuse of the med, whether the substance is a precursor of another substance that is already scheduled, and a substance's potential for physical or psychological addiction. affects prescribing, dispensing, storage, and ordering. product labeling will include scheduling. |
|
|
Schedule I Controlled Substances |
are not usually in pharmacies. high potential for abuse, lack of data for safe use in humans, not current acceptable medical use. illegal substances including marijuana, LSD, PCP, GHB, and ecstasy. |
|
|
Schedule II Controlled Substances |
Highest potential for abuse and physiological dependence or addiction. most stringent requirements in pharmacy. examples of opioids include single ingredient codeine products, fentanyl, hydromorphone, meperidine, hydrocodone combinations, morphine sulfate, methadone, and oxycodone. examples of stimulants include amphetamine/dextroamphetamine combos, dextroamphetamine, methylphenidatem dexmethylphenidate, and lisdexamfetamine. |
|
|
Schedule III Controlled Substances |
less abuse and addiction potential than schedule II medications. examples include buprenorphine, buprenorphine/naloxone, acetaminophen with codeine, butalbital with aspirin, and testosterone. |
|
|
Schedule IV Controlled Substances |
less abuse and addiction potential than schedule II and III medications. examples include phentermine, alprazolam, clonazepam, lorazepam, diazepam, temazepam, triazolam, carisoprodol, modafinil, zolpidem, zaleplon, eszopiclone, tramadol, and phenobarbital. |
|
|
Schedule V Controlled Substances |
lowest abuse potential of all controlled substances. examples include codeine combination products with no more than 200 mg codeine/100 mL, diphenoxylate and not less than 25 mg atropine per dosage unit, pregabalin, ezogabine, and lacosamine. |
|
|
Who can prescribe controlled substances |
prescribers must register with DEA. most states allow: physicians (MD, DO), dentists (DDS, DD), podiatrists (DPM), veterinarians (DVM). some states allow: physician assistants (PA), nurse practitioners (NP, ARNP, CRNP), optometrists (OD) |
|
|
DEA number |
9 characters; 2 letters followed by 7 computer generated numbers. first letter: A, B, F, M, or X A, B, F = physician, dentist, pharmacy, etc. M = midlevel prescriber (physician's assistant etc) X = prescribers who meet requirements to prescribe suboxone for opioid dependence. second letter: first letter of person's last name or company name |
|
|
DEA number verification |
sum 1 = 1st digit + 3rd digit + 5th digit sum 2 = 2nd digit + 4th digit + 6th digit sum 1 + sum 2 = verification number the last digit on the right of the verification number must match the last digit of the DEA number. |
|
|
When can controlled substances be prescribed |
written for a legitimate medical purpose. must be written by a prescriber acting in usual course of practice. |
|
|
Required information on a controlled substance prescription |
Rxs must include: date of issue, patient's full name and address; prescriber's full name, address, and DEA registration number; drug name; drug strength; dosage form; quantity prescribed; directions for use; number of refills authorized if any; and prescriber's signature |
|
|
prescription format |
schedule II prescriptions can be written or electronic; verbal allowed in emergency situations only (only amount for emergency period; pharmacy must receive written hand-signed RX within 7 days); faxed allowed to expedite filling process if pharmacist has original before dispensing med; faxes allowed in long-term care facilities and for certain hospice pts. schedule III, IV, V prescriptions can be faxed, verbal, electronic, or written. |
|
|
Prescription refills |
schedule II prescriptions canNOT be refilled. schedule III and IV prescriptions can have up to 5 refills. schedule V prescriptions can be refilled as authorized by the presciber. |
|
|
Prescription expiration |
schedule II prescriptions have no time limit; up to the pharmacist's discretion. schedule III and IV prescriptions are good up to 6 months after date of issue. schedule V prescriptions have no time limit; up to prescriber's discretion |
|
|
preparing and counting controlled substances |
varies among pharmacies; depends on medication, supervising pharmacist, and employer. |
|
|
partial fills on controlled substances |
schedule II prescriptions can be partially filled; initial quantity dispensed on front of RX; remaining portion filled with 72 hours. schedule III, IV, and V prescriptions can be partial filled; no time restrictions as long as prescription is not expired. |
|
|
prescription labels for controlled substances |
label must include: pharmacy's name and address; prescription number; patient's name; prescriber's name; directions for use; date of filling; and warning statement - "caution: federal law prohibits the transfer of this drug to any person other than the patient for whom it was prescribed" for schedule II, III, and IV medications |
|
|
ordering schedule II medications |
DEA form 222 triplicate paper form electronic controlled substance ordering system CSOS date and amount received must be documented records must be kept for 2 years |
|
|
ordering schedule III, IV, V medications |
no special forms required |
|
|
storing controlled substances in the pharmacy |
store in securely locked cabinet or dispersed throughout pharmacy shelves with other non-controlled medications |
|
|
storing controlled substances in patient care units |
all controlled substances must be secure, locked place never leave medications unattended on a cart when delivering meds |
|
|
inventory requirements for schedule II medications |
exact count some pharmacies use perpetual (ongoing) inventory |
|
|
inventory requirements for schedule III, IV, V medications |
estimated count fr containers that hold less than 1000 dosage units exact count for containers that hold 1000 dosage units or more |
|
|
inventory frequency |
every 2 years |
|
|
inventory recordkeeping |
2 years from inventory completion |
|
|
recordkeeping requirements for schedule II medications |
all prescription, inventory, and order forms must be kept separate from all other pharmacy records all records must be stored for at least 2 years |
|
|
recordkeeping requirements for schedule III, IV, V medications |
all prescription, inventory, and order forms must be kept separate from other pharmacy records or in a readily retrievable fashion all records must be stored for at least 2 years |
|
|
transferring controlled substance medications |
a pharmacy can distribute controlled substance medications to another pharmacy or DEA registered practitioner invoice system required DEA form 222 (or electronic equivalent) required for schedule II medications pharmacy can NOT distribute more than 5% of all controlled substances dispensed per year |
|
|
transferring controlled substance prescriptions |
a pharmacy can transfer a schedule III, IV, or V controlled substance prescription to another pharmacy one time only; exception if pharmacies share an electronic real time online database |
|
|
reverse distributor disposal of controlled sub meds |
pharmacies can send defective or expired controlled substances to DEA registered reverse distributor if schedule II meds, DEA form 222 (or electronic equivalent) is required |
|
|
pharmacy level disposal of controlled sub meds |
hospital - blanket approval by DEA for regular, periodic destruction (e.g. wasting of incomplete doses); DEA for 41 required community - approval by DEA BEFORE destruction; DEA form 41 required |
|
|
robbery or diversion of controlled sub meds |
pharmacist must contact local police, DEA, and board of pharmacy (if required by state law) complete DEA form 106 |
|
|
reasons for special dispensing/prescribing requirements |
keep patients using the medication safe. usually in place for medications with serious side effects. |
|
|
types of special dispensing/prescribing requirements |
mandated by federal law (e.g. age limitations on morning after pill and nicotine products). Risk Evaluation Mitigation Strategy (REMS) program (e.g. ER/LA opioid analgesic REMS program). Special training by prescribers (e.g. buprenorphine and buprenorphine/naloxone for opioid dependence) enrollment in special programs (e.g. STEPS for thalidomide) Registires (e.g. Clozaril National Registry and North American Antiepileptic Drug Pregnancy Registry.) |
|
|
REMS program |
Risk Evaluation Mitigation Strategy program |
|
|
Combat Methamphetamine Epidemic Act of 2005 |
restrict sales of pseudoephedrine and reduce the production of methamphetamine. retail limits of OTC sales: 3.6 grams/day or 9 grams/30 days. mail order limits: 7.5 grams/30 days pseudoephedrine must be kept behind the counter or in locked cabinet pt's ID verified with each transaction with state or federal government issued photo ID. pharmacy must maintain log of sales which must include name/address/signature of purchaser and name/amount of product sold. records must be kept for at least 2 years |
|
|
iPLEDGE program |
for isotretinoin (accutane, etc) - acne med reduce chance of birth defects prescribers must register with i PLEDGE before obtaining an isotretinoin precription; female pts of child bearing age must have monthly pregnancy tests and confirm the use of two separate forms of birth control. pharmacies must register with iPLEDGE before ordering and dispensing isotretinoin; a risk management authorization (RMA) number is required on prescription; isotretinoin prescriptions cannot have refills or be fore more than 30 days supply; MedGuide required; a "do not dispense after" date provided (7 days after pregnancy test for females of child bearing age; 30 days after office visit for all other pts) |
|
|
APPRISE - REMS program |
assisting providers and cancer patients with risk information for sale use of erythropoiesis stimulating agents (e.g. erythropoietins: aranesp, epogen, procrit, etc) ensures pts are informed about the risk of blood clots, heart problems, and death from erythropoietins. program is specific for cancer pts. prescribers must be certified before dispensing erythropoietins to cancer pts. cancer pts and prescriber must sign risk acknowledgement form. all pts in and out must receive MedGuide. |
|
|
TIRF - REMS program |
mitigates the misuse, abuse, addiction, and overdose of transmucosal immediate release fentanyl products. prescribers must enroll in TIRF program before writing prescriptions for outpts. outpts must sign pt-prescriber agreement. pharmacies in and outpt must enroll in TIRF program before dispensing; outpt pharmacy will verify pt enrollment at first fill through electronic verification system; dispense MedGuide with outpt prescriptions |
|
|
PPL |
Prescribing Program for Lotronex - IBS ensures prescribers and pts are informed about serious GI effects from alosetron. prescribers must enroll in PL program before writing alosetron prescriptions; review MedGuide with pt. Pts must sign pt acknowledgement form. pharmacies must verfify alosetron prescriptions contain PPL sticker; ensure alosetron prescription is handwritten (faxed, telephone, electronic orders are not allowed) |
|
|
CNR, CPAS, Teva Clozapine Patient Registry |
Clozaril National Registry/Clozapine Prescription Access System - blood cells track and help prevent cases of agranulocytosis prescribers must register with registry before writing prescriptions; must register pts; must order WBC and ANC lab work. pharmacies must register with registry before dispensing; verify pts are registered and lab work is completed within 7 days of dispensing drug. |
|
|
andro |
male |
|
|
cardi, cardio |
heart |
|
|
derm |
skin |
|
|
emia |
blood |
|
|
gastro, gast |
stomach, abdomen |
|
|
gyn, gene, gynec, gyno |
woman |
|
|
hem, hema, hemat, hemato |
blood |
|
|
hepat, hepato |
liver |
|
|
nephr, nephro |
kidney |
|
|
ocul, oculo, ophthalm, ophthalmo |
eye |
|
|
ost, osteo |
bone |
|
|
oti |
ear |
|
|
psych, psyche, psycho |
mind |
|
|
thromb, thrombo |
blood clot |
|
|
thyr, thyro |
thyroid gland |
|
|
vas, vaso, vasculo |
blood vessel |
|
|
anti |
against |
|
|
chemo |
chemical |
|
|
contra |
against, oppose |
|
|
ferri, ferro |
iron |
|
|
hypno |
sleep |
|
|
intra |
within |
|
|
mimetic |
mimicking, simulating |
|
|
pyro, pyret |
heat, fever |
|
|
a, an |
without |
|
|
auto |
self |
|
|
carcin, carcino |
cancer |
|
|
hyper |
excessive; above normal |
|
|
hypo |
beneath; less than normal |
|
|
itis |
inflammation |
|
|
ology |
study of |
|
|
photo, phot |
light |
|
|
pre |
before |
|
|
rrhagia, rrhage, rrhea |
discharge, flowing |
|
|
semi |
one half, partly |
|
|
therm, thermo |
heat |
|
|
Rx |
prescription; Latin for "recipe" |
|
|
sig |
latin for "you write" |
|
|
disp |
dispense |
|
|
qty |
quantity |
|
|
DAW |
dispense as written |
|
|
cap |
capsule |
|
|
tab |
tablet |
|
|
cr |
cream |
|
|
lot |
lotion |
|
|
sol |
solution |
|
|
supp |
suppository |
|
|
susp |
suspension |
|
|
syr |
syrup |
|
|
ung, oin |
ointment |
|
|
a |
before think a comes before everything else |
|
|
p |
after think of p as post or comes after a in the alphabet |
|
|
c |
with |
|
|
cm |
with meals |
|
|
ac |
before meals |
|
|
pc |
after meals |
|
|
am |
in the morning |
|
|
pm |
in the evening |
|
|
hs |
at bedtime |
|
|
stat |
right away, immediately |
|
|
d |
day |
|
|
hr, h |
hour |
|
|
aa |
affected area |
|
|
po |
by mouth |
|
|
ien |
in each nostril |
|
|
sl |
sublingual |
|
|
pr |
per rectum |
|
|
iv |
intravenous |
|
|
ivpb |
intravenous piggy back |
|
|
im |
intramuscular
|
|
|
sub-q, sc, sq |
subcutaneously |
|
|
au |
both ears think of auditory for a |
|
|
ad |
right ear think of dominant for d because right is dominant |
|
|
as |
left ear think of sinister for s because left is bad side |
|
|
ou |
both eyes think of ophthalmic for o |
|
|
od |
right eye think of dominant for d |
|
|
os |
left eye think of sinister for s |
|
|
q |
every |
|
|
qd |
every day |
|
|
qam |
every morning |
|
|
qpm |
every evening |
|
|
qhs |
every night at bedtime |
|
|
q4h |
every 4 hours |
|
|
qod |
every other day |
|
|
bid |
twice daily |
|
|
tid |
three times daily |
|
|
qid |
four times daily |
|
|
nr |
no refills |
|
|
prn |
as needed |
|
|
ad, uad, ud, ut dict |
as directed, use as directed |
|
|
w, wk |
week |
|
|
dtd
|
dispense such doses
|
|
|
qs |
quantity sufficient |
|
|
ss |
one half, sliding scale |
|
|
u |
unit |
|
|
iu |
international unit |
|
|
g |
grams |
|
|
mcg |
micrograms |
|
|
mg |
miligrams |
|
|
kg |
kilograms |
|
|
oz |
ounces |
|
|
gtts |
drops |
|
|
l |
liters |
|
|
mL |
mililiters |
|
|
cc |
cubic centimeter |
|
|
tbsp |
tablespoon |
|
|
tsp |
teaspoon |
|
|
apap |
acetaminophen |
|
|
asa |
aspirin |
|
|
fe |
iron |
|
|
k |
potassium |
|
|
na |
sodium |
|
|
hci |
hydrochloride |
|
|
mso4 |
morphine sulfate |
|
|
MgSO4 |
magnesium sulfate |
|
|
ZnSO4 |
zinc sulfate |
|
|
PCN, PEN |
penicillin |
|
|
SMX/TMP |
sulfamethoxazole/trimethoprim |
|
|
tcn |
tertracycline |
|
|
norflox |
norfloxacin |
|
|
iv vanc |
intravenous vancomycin |
|
|
hctz |
hydrochlorothiazide |
|
|
hct |
hydrocortisone |
|
|
ntg |
nitroglycerin |
|
|
d5w |
dextrose 5% in water |
|
|
lr |
lactated ringer's |
|
|
bp |
blood pressure |
|
|
hbp |
high blood pressure |
|
|
n/v |
nausea/vomiting |
|
|
p, pa |
pain |
|
|
nka, nkda |
no known allergies, no known drug allergies |
|
|
/ |
per |
|
|
1/2 |
ss |
|
|
1 |
I |
|
|
5 |
V |
|
|
10 |
X |
|
|
50 |
L |
|
|
100 |
C |
|
|
500 |
D |
|
|
1000 |
M |
|
|
L, C, D, M |
Lucky -50 Cows - 100 Drink - 500 Milk - 1000 |
|
|
roman numeral rule 1 |
letters are repeated to form various numbers. when a letter is repeated its value is repeated
|
|
|
roman numeral rule 2 |
letters are never repeated more than three times. once a numeral repeats three times, you must subtract |
|
|
roman numeral rule 3 |
when a smaller number is placed in front of a larger number it is subtracted |
|
|
roman numeral rule 4 |
v, l, d can never be repeated and are never subtracted from larger numbers |
|
|
roman numeral rule 5 |
you can never subtract more than one numeral |
|
|
roman numeral rule 6 |
when an equal or smaller number is placed after the larger number, it is added. so if the larger number is on the left, and the smaller number is on the right add the values |
|
|
roman numeral rule 7 |
when there are three or more numerals and a smaller valued numeral comes between two larger valued numerals subtract the smaller valued numeral from the larger valued number that follows it |
|
|
1 grain |
65 milligrams |
|
|
16 ounces |
7000 grains |
|
|
1 pound |
16 ounces |
|
|
8 ounces |
1 cup |
|
|
2 cups |
1 pint |
|
|
2 pints |
1 quart |
|
|
4 quarts |
1 gallon |
|
|
1 kilogram |
1000 grams |
|
|
1 gram |
1000 milligrams |
|
|
1 milligram |
1000 micrograms |
|
|
1 milligram |
0.001 gram |
|
|
60 grains (gr) |
1 dram (dr) |
|
|
1 microgram |
0.001 milligram |
|
|
1 liter |
1000 milliliters or cc |
|
|
1 deciliter |
100 milliliters or cc |
|
|
1 deciliter |
0.1 liter |
|
|
1 tablespoon |
3 teaspoons |
|
|
1 pint |
16 fluid ounces |
|
|
2 tablespoons |
1 ounce |
|
|
1 cup |
8 ounces |
|
|
1 pint |
2 cups |
|
|
1 quart |
4 cups = 2 pints |
|
|
8 drams (dr) |
1 ounce |
|
|
Celsius and Fahrenheit conversion |
9 x •C = (5 x •F) - 160 |
|
|
20 drops |
1 mL |
|
|
1 oz |
30 mL |
|
|
1 tbsp |
15 mL |
|
|
1 tsp |
5 mL or cc |
|
|
1 pt |
480 mL |
|
|
1 qt |
960 mL |
|
|
1 gal |
3840 mL = 3.84 L |
|
|
5 grain |
325 mg |
|
|
12 ounces |
1 pound |
|
|
1 lb |
0.454 kg |
|
|
1 kg |
2.2 lb |
|
|
1 oz |
28.35 g |
|
|
1 cc |
1 mL |
|
|
Converting from a larger measurement to a smaller measurement within the metric system |
When going larger to smaller multiply. It will take more of a smaller unit to make the equivalent of the larger unit. e.g. 50kg to g 50kg x 1000g/1kg = 50,000g |
|
|
Converting from a smaller measurement to a larger measurement within the metric system |
When going from a smaller measurement to a larger divide. It will take less of a larger unit to make the equivalent of the smaller. e.g. 300mL to L 300mL x 1L/1000mL = 0.3 L |
|
|
Converting household measurements |
Units you have x Number of units you want/units you have e.g. 3 tablespoons to tsp 3 tbsp x 3 tsp/1 tbsp = 9 tsp |
|
|
Converting between measurement systems |
Units you have x Number of units you want/units you have e.g. 240 mL = ? oz, 30 mL = 1 oz 240mL x 1 oz/30mL = 8 oz |
|
|
Equation for ratio and proportion calculations |
a/b = c/d |
|
|
1 fluid dram (fl. dr) |
5 milliliters mL |
|
|
8 fluid drams |
1 fluid ounce |
|
|
16 fluid ounces |
1 pint |
|
|
1 ounce |
437.5 grains |
|
|
Weight to weight percentage |
Solids are expressed as a weight to weight percentage w/w%. This is a measurement of the amount of one solid expressed in g contained in a specific amount of another solid per 100 g. Divide amount of active ingredient by total weight of product. Multiply by 100% to get percentage value. |
|
|
Weight to volume percentage |
When a solid is mixed with a liquid the concentration is expressed as a weight to volume percentage w/v%. This is a measurement of the amount of the solid expressed in grams contained in a specific amount of liquid per 100 mL. Divide amount of active ingredient by total amount of solution. Multiply by 100% to get percentage value. |
|
|
Volume to volume percentage |
When two liquids are mixed together the concentration is expressed as a volume to volume percentage v/v%. This is a measurement of the amount of one liquid expressed in mL contained in a specific amount of another liquid per 100 mL. Divide amount of active ingredient by total amount of solution. Multiply by 100% to get percentage value. |
|
|
Dilution calculations |
Q1/Q2 = C2/C1 Q1 = initial quantity C1 = initial concentration % Q2 = final quantity C2 = final concentration % Set up equation with known values, cross multiply, divide both sides to get x by itself, solve. |
|
|
Flow rate calculations |
First set up fractions with known terms. Next set up ratio and proportion calculation to find the number of drops needed. Then cross multiply. Divide both sides of the equation to get x by itself. Solve for x. Calculate how many drops per minute will be needed for the amount of time by dividing the drops by the minutes. e.g. Known flow rate/known flow rate = x drops/known order amount |
|
|
Alligation calculations |
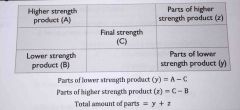
Set you table with known values. Solve for z and y. Calculate amount of higher strength needed: total parts/z = total amount prescribed/amount of higher strength Calculate amount of lower strength needed: total parts/y = total amount prescribed/amount of lower strength |
|
|
Infusion time calculations |
Convert to mL if necessary. Set up ratio and proportion, infusion rate = iv order/x hr. Cross multiply Divide to get x by itself. Solve for x. |
|
|
Milliequivalent calculations |
Set up calculation with known values. Cross multiply. Divide to get x by itself. Solve for x. |
|
|
AWP |
Average whole sale price or sticker price because it isn't the real price the pharmacies pay for a drug, but rather a published average of what wholesalers charge pharmacies. |
|
|
Cost |
Actual acquisition cost or cost of goods sold COGS. It is how much a a pharmacy pays for the drug, including the pharmacy's discounts, rebates, and other price adjustments. It does not include dispensing fees. |
|
|
Gross Margin |
Aka gross profit. It's the difference between the selling price and cost (acquisition cost/COGS). |
|
|
Inventory |
An itemized list of goods and materials, with costs, in a business. An inventory count is required at least yearly to check the business's net profit. |
|
|
Markdown |
A reduction of price. Most people use the terminology discount, or sale price, to reference a markdown. |
|
|
Markup |
The difference between the selling price and cost of an item. |
|
|
Net Profit |
The amount of money left after all expenses are paid, including overhead and inventory costs. If this number is positive, the business made money. If this number is negative, the business lost money. |
|
|
Overhead |
The cost of running a business, including rent, utilities, salaries, etc. Keep in mind, the cost of goods and materials is not part of the overhead cost. |
|
|
Selling Price |
The price the business charges for a product. It is the amount to be paid for the goods or service. |
|
|
Turnover Rate |
How often the total inventory is sold over a specific time period. A high turnover means inventory sold quickly. A low turnover means inventory sold slowly. |
|
|
Markup Calculation |
Markup = Selling price - Cost |
|
|
Gross Margin or Profit Calculation |
Gross profit = Selling price - Invoice cost (COGS) |
|
|
Markup Percent on Cost Calculation |
Markup % on cost = selling price - cost/cost x 100% |
|
|
Markup Percent on Retail Calculation |
Markup % on retail = Selling price - cost/selling price x 100% |
|
|
Gross Profit Percent of Sales Calculation |
Gross profit percent of sales = selling price - invoice cost (COGS)/selling price x 100% |
|
|
Gross Profit Percent of Cost Calculation |
Gross profit percent of cost = selling price - invoice cost (COGS)/invoice cost x 100% |
|
|
Net Profit Calculation |
Net profit = selling price - (cost + overhead) |
|
|
Annual Inventory Calculation |
Annual Inventory = beginning inventory + ending inventory/2 |
|
|
Inventory Turnover Rate (ITOR) for a Community Pharmacy Calculation |
ITOR community = costs over inventory time period/annual inventory |
|
|
Inventory Turnover Rate (ITOR) for a Hospital Pharmacy Calculation |
ITOR hospital = purchases/annual inventory |
|
|
Figuring Costs for Patients Calculation |
Use ratio and proportion calculation to solve these problems. e.g: Rx for 30 capsules costs $80.10, the patient only wants 7 capsules. 30 caps/$80.10 = 7 caps/x Cross multiply. Divide both sides by 30 to get x by itself. Solve for x. |
|
|
Average Wholesale Price (AWP)/Retail Price of a med based on its AWP Calculation |
If the AWP for 90 tabs is $354.31, and your pharmacy charges AWP + $5 dispensing fee, what will the retail price for 30 tabs be? Set up ratio and proportion calculation with known values, $354.31/90 tabs = x/30 tabs Cross multiply, divide both sides to get x by itself, solve for x, add dispensing fee. |
|
|
Capsules |
Small, oblong gelatin "containers" filled with medication. Capsules filled with liquid medications are more commonly known as gelcaps. |
|
|
Tablets |
Solid dosage forms in different shapes, sizes, weight and other properties. Mostly swallowed whole and later break apart and dissolve in the digestive tract. Tablets shaped like a capsule are more commonly known as caplets. |
|
|
Buccal tablets |
Placed in the buccal pouch or the area between the cheek and gum, usually behind the rear molar. Dissolve slowly and are absorbed directly into the blood stream without passing through the digestive tract. |
|
|
Sublingual tablets |
Place under the tongue. Dissolve rapidly and are absorbed directly into the blood stream without passing through the digestive tract. |
|
|
Chewable tablets |
Intended to be chewed before swallowing. |
|
|
Effervescent tablets |
Contains mixtures of acids and sodium bicarbonate plus the active drug ingredients. Made to be dissolved in water FIRST, then administered like a drink to the patient. Release carbon dioxide and dissolve rapidly in water. |
|
|
Enteric-coated tablets |
Coated to prevent the tablet from dissolving in the stomach. Most dissolve lower in the digestive tract, usually in the small intestines instead of the stomach. |
|
|
Troches and lozenges |
Held inside the mouth until they dissolve. Small, square-shaped tablets keep the medication in contact wit the mouth and throat for an extended period of time. |
|
|
Pills |
Solid dosage forms made from a paste, rolled between the first finger and thumb and then dried. |
|
|
Controlled-release products |
Release medications over an extended period of time. Can be identified by the following drug suffixes; LA (long-acting), TR (timed-release), SA (sustained-action), ER (extended-release), SR (sustained-release). |
|
|
Solutions |
Preparations in which the solid ingredients of medications are dissolved in a liquid (usually water). |
|
|
Suspensions |
Substances in which medication particles are suspended in liquid bu the medication is not completely dissolved. |
|
|
Elixirs |
Hydroalcohoic liquids (a combination of water and alcohol) |
|
|
Fluid Extracts and Tinctures |
Use alcohol, water, or a combination of the two as their base and usually contain plant extracts as their active ingredients. Fluid extracts contain the oil or active portion of a plant or herb, which is usually removed or extracted with alcohol. Tinctures are used today mostly as topical liquids, and not as oral liquids. |
|
|
Syrups |
Concentrated solutions of sugar (usually sucrose) in water, with or without active ingredients. Some may contain alcohol, but usually in very small amounts. |
|
|
Spirits or Essences |
Alcoholic or hydroalcoholic solutions of volatile substances. Usually contain such a high percentage of alcohol that they require storage in tight containers to prevent loss through evaporation. |
|
|
Ointments |
Oil-based, greasy preparations usually in petrolatum jelly base. Good for delivering medication to areas of skin that need protection, or for dry, scaly areas. Leave an oily coating on the skin. |
|
|
Creams |
Semi-solid emulsions or combinations of water, oil, and other substances, such as the active drug ingredient. Often used on weeping or oozing skin conditions. Less greasy and easier to spread and remove the ointments. |
|
|
Lotions |
Contain more liquid than creams. Can be applied easily over larger areas of the body. Good for applying to areas where friction is a problem (under the armpits or in between the thighs) or hair areas (scalp, legs, etc). |
|
|
Liniments or Balms |
Liquid mixtures of various substances in oil, alcoholic solutions of soap or emulsions intended for external application. Used to relieve achy muscles and joint pain. Should be rubbed in with friction and should never be applied to damaged or broken skin. |
|
|
Gels |
Semi-solid suspensions of very small particles, usually in a water base. Appear as solid, jelly-like substances. Penetrate deeper into the skin layers without causing skin damage. |
|
|
Collodions |
Highly flammable solutions made up of pyroxylin, ether, and alcohol that dry as flexible film on skin. Used as adhesives to close small wounds or as a surgical dressing. Some have medications added. |
|
|
Transdermal Patches |
Designed for drugs to be delivered through the skin. |
|
|
Suppositories |
Designed to remain solid at room temperature or a refrigerated temperature, and to melt when inserted into the body (rectum, vagina, or urethra). Once the suppository melts inside the body, the active drug ingredient is released and will produce a local or systemic (full-body) effect, depending on the medication. |
|
|
Vaginal tablets |
Uncoated bullet-shaped or ovoid tablets inserted in the vagina for local effect. Used to treat vaginal infection or to restore vaginal tissues to a normal state after surgery or from decreased hormone action during menopause. |
|
|
Parenteral
|
Refers to injectable routes of administration. IV, IM, SQ, etc.
|
|
|
Injectable solutions
|
Most injectable drugs are formulated as sterile solutions. Solutions are preparations in which the solid ingredients of medications are dissolved in a liquid.
|
|
|
Injectable suspensions
|
Suspensions are substances in which medication particles are suspended in liquid and the medication is not dissolved. Injected in the muscle, never into veins or arteries. Some suspensions are given as a depot where the injected drug is absorbed slowly over several weeks to months.
|
|
|
Injectable emulsions
|
Mixtures of water and oil. Injectable emulsions are most commonly used when patients are unable to take food by mouth, and they must be fed through their veins.
|
|
|
Intranasal aerosols
|
Administered inside the nose as drops or as a spray. Used most often for their local effects in the nose.
|
|
|
Inhaled aerosols
|
Used for getting medicines deep into the lung
|
|
|
Topical aerosols
|
Most commonly used for skin conditions
|
|
|
Required parts of a prescription
|
Patient's name, issue date, medication name and strength, sig, quantity, dispense as written (DAW), refills, prescriber's signature, DEA number if control substance.
|
|
|
Community setting prescription labels
|
Should contain drug name, strength, dosage form, amount to dispense, pharmacy name, phone number |
|
|
Hospital setting prescription labels
|
Should contain patient name, patient location (room number, floor, etc), drug name, dose, diluents, volume of diluents, rate of infusion, beyond use date
|
|
|
Graduated cylinders
|
Often used to measure liquid medications. The liquid's meniscus is the downward curve at the top of the liquid. When reading the meniscus, the lower level must align with the desired mark on the measuring device.
|
|
|
Pyxis
|
Used in hospital setting. Automatic dispensing cabinet where meds are stored.
|
|
|
Prescription balances
|
Used to weigh materials for compounding. Either a Class A torsion balance or an electronic balance can be used. A brass weight set will be needed for the use of a torsion balance and for checking an electronic balance.
|
|
|
Mortars and pestles
|
Used to crush tablets or mix ingredients in a compound. Glass mortar and pestle is best for liquid preparations and for chemicals that are oily and will stain. Ceramic mortar pestle is best for reducing the size of dry crystals or hard powder particles and for preparing emulsions. Porcelain mortar and pestle is best for blending powders and for pulverizing soft materials or crystals.
|
|
|
Compounding record
|
Includes the following: Name and strength of the compounded preparation. Formulation record reference for the compounded preparation. Sources and lot numbers of ingredients used, and actual quantities measured/weighed. Number of dosage units, or quantity, compounded. Name of the person who prepared the compound. Date of preparation. Internal identification number or prescription number. Beyond-use date. |
|
|
Formulation record
|
Name, strength, and dosage form of the compound. Ingredients and quantities. Required equipment. Mixing instructions. Assigned beyond-use date. Appropriate container for dispensing. Storage requirements. Quality control procedures. Source of recipe.
|
|
|
Small volume parenterals |
Consist of single-dose or multi-dose vials. E.g: ampules, prefilled syringes, minibags (25 mL, 50 mL, and 100 mL bags)
|
|
|
Large volume parenterals
|
Consist of IV bags that hold 250 mL or more. E.g: Iv fluids to avoid dehydration, Total Parenteral Nutrition (TPNs)
|
|
|
Laminar flow hoods
|
House the area where sterile compounds are made.
|
|
|
Types of laminar flow hoods
|
A horizontal laminar flow hood circulates the air from back to front. A vertical laminar flow hood circulates the air from top to bottom. Both contain a high-efficiency particulate (HEPA) filter.
|
|
|
Cleaning laminar flow hoods
|
Laminar flow hoods should be cleaned before and after each use with a 70% alcohol or 10% bleach solution and a lint-free cloth or gauze. Begin at the top of the hood, working from back to front. Once the top is finished, the sides will be next, working from the top and wiping back to front. Lastly, the work surface will be cleaned, working from back to front and wiping side to side (left to right). Hoods must be tested at least every 6 months and any times the hood is relocated.
|
|
|
Syringes
|
Used to get exact measurements of liquids. The size should be closet to the amount needed for the dose. Before liquid is pulled into a syringe, the plunger should be pulled back to the amount needed. The bottom of the black rubber stopper should line up with the desired marking on the side of the syringe.
|
|
|
Hypodermic needles
|
Used to draw up medications from vials or ampules for transfer to IV bags, or for administering the med directly to the patient. The smaller the gauge, the larger the lumen or bore of the needle. E.g. A 27 gauge needle is smaller (or skinnier) than a 16 gauge needle.
|
|
|
Total Parenteral Nutrition (TPN) compounding machines
|
Usually needed for institutions that commonly make TPNs for patients who cannot swallow or take meds by mouth.
|
|
|
Arrangement of supplies when using the laminar flow hood
|
All supplies should be placed in the back 2/3 of the hood. Medications are best prepared at least 6 inches in from the sides and front of the laminar flow hood. Critical items should be placed as close to the air source as possible, without touching the filter or back of the hood.
|
|
|
Preparing medications using the laminar flow hood
|
Disinfect all rubber stoppers, ampule necks, and ports on IV bags with an alcohol swab before inserting the needle. Use a 45 degree angle, bevel side up when inserting needles into rubber vial caps to prevent coring of the rubber. Use a filter needle when pulling up the contents of a glass ampule to prevent any broken glass particles from entering the syringe. Avoid blocking airflow to needles, vials, and ports with hands during preparation. Clean any spillage working from back to front and side to side.
|
|
|
Unit-dose prescriptions
|
Means each dose is packaged individually. Can be a vial, a syringe, a plastic bubble, an envelope, or baggie with the medicine inside.
|
|
|
Preparing unit-dose prescriptions
|
Many institutions will have a pre-packing machine to ease and quicken the process. Some will bubble pack unit dose prescriptions. Must be stored in appropriate containers.
|
|
|
Beyond use dating for unit-dose prescriptions |
State law regulates the beyond use date for most repackaged unit doses. Usually is one year from the date of dispensing or the manufacturer's expiration date, whichever comes first. |
|
|
Medicaid
|
Joint federal and state program that helps people with low income and limited resources pay for medical costs. Pays for outpatient prescriptions and care provided by nursing homes or hospitals. Rules and regulations will vary from state to state.
|
|
|
Medicare
|
Managed by the federal government and is the nation's largest health insurance program. Provides coverage for people 65 and older, some disabled people, and people with kidney failure who are treated with dialysis or with a kidney transplant. Divided into four different categories of coverage.
|
|
|
Medicare Part A
|
Hospital insurance. Helps pay for hospital visits, care in a skilled nursing facility, hospice care, and some home health care. Does not cover prescription drugs for outpatients.
|
|
|
Medicare Part B
|
Medical insurance. Helps pay for doctors' services, outpatient hospital care, physical therapy and home health care. Covers a limited number of prescription drugs for outpatients (vaccines, diabetic testing supplies, etc).
|
|
|
Medicare Part D |
Prescription drug plan. Pays for most Rx drugs in the outpatient setting. Coverage is optional and it can be added on to "original Medicare" or Part A and/or Part B. Is not require to cover every medication.
|
|
|
Medicare Part C
|
An alternative to "original Medicare" or Part D. Called the Medicare Advantage Plan or Medicare Health Plan. Ran by private insurance companies but approved by Medicare.
|