![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
73 Cards in this Set
- Front
- Back
|
Scrotal Transillumination |
Scrotal lesions that transilluminate include hydrocele, spermatocele, and varicocele |
|

|
Hydrocele, observed via scrotal transillumination |
|
|
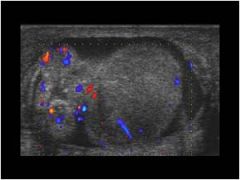
Testicular torsion |
Acute, unilateral scrotal pain usually occurring in adolescents due to sudden twisting of spermatic cord producing testicular ischemia. Involved testicle is tender, edematous and indurated Elevation of testicle does not relieve pain. Reduced blood flow via doppler US; requires immediate surgery. |
|
|
US: Testicular torsion with reduced blood flow to left testicle. Will become ischemic if not fixed in <6 hrs Differential diagnosis: acute epididymitis, renal stone, incarcerated hernia |
|
|
Deformity which predisposes males for testicular torsion |
Bell clapper deformity: tunica vaginalis joins high on the spermatic cord, leaving the testis free to rotate |
|
|
Testicular mass/nodule |
Non-tender, solid testicular mass; assumed to be cancer until proven otherwise. Testicular cancer is the most common solid cancer in men 15-35 yrs of age |
|
|
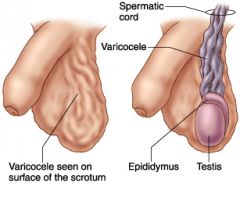
Varicocele |
Dilatation of pampiniform plexus of spermatic veins causes scrotal enlargement that feels like "bag of worms" Disappears when lying down (recumbence) On exam: cannot find sup. margin of lesion Usu. asymptomatic; more common on left side Can cause infertility; may signal renal cell carcinoma if cancer invades L renal vein, impedes L testicular venous drainage |
|
|
Varicocele Tortuous veins visible on examination On palpation, feels like "bag of worms" May be assoc. w/ renal cell carcinoma Common (15-20% in post-pub. males) "Nutcracker" syndrome: L renal vein compression by sup. mes. artery/aorta-->varicocele/hematuria |
|
|
Genital wart |
Reflects HPV infection (STD) HPV infection is also a risk factor for penile carcinoma |
|

|
Genital warts on upper shaft of penis |
|
|
Herpes simplex lesion |
Usu. occurs as multiple painful vesicles Due to HSV-2 infxn (most commonly) Primary infxn: ~6 days post-exposure -Very painful; assoc. w/ dysuria, fever, inguinal adenopathy, headache, occ. viral meningitis Recurrent dz: milder symptoms, occ. lesions Asymp. pt's may shed virus, transmit dz w/ sexual contact (70% attack rate in sero(-) people) |
|

|
HSV-2 lesions Painful vesicles on head and shaft of penis |
|
|
Paraphimosis |
Inability to replace retracted foreskin Usu. very painful, unless there is severe neuropathy Considered a medical emergency: increasing penile edema-->penile ischemia/necrosis |
|

|
Paraphimosis Risk in uncircumsized men Considered a risk factor for penile cancer Considered a medical emergency |
|
|
Penile cancer |
Squamous cell carcinoma (most) Begins as painless papule that progresses HPV DNA in 30-50% of lesions |
|

|
Penile cancer on head Usu. squamous cell carcinoma Progresses from painless papule Assoc. w/ HPV in 30-50% of cases |
|
|
Phimosis |
Inability to retract foreskin Strong risk factor for squamous cell carcinoma of the penis May use topical steroid cream |
|

|
Phimosis Strong risk factor for squamous cell carcinoma of penis Treat with circumcision |
|
|
Syphilitic chancre |
Painless lesion occurring ~21 days after exposure Reflects site of spirochete entry (Treponema pallidum) Solitary papule-->ulceration (indurated, w/out exudate) Heals in 4-8 weeks w/out treatment |
|

|
Syphilitic chancre (primary syphilis) Painless, indurated ulcer without exudate Occurs ~21 days post-exposure Heals in 4-8 weeks w/out treatment |
|
|
Hydrocele |
Fluid-filled sac (often painless) surrounding a testicle, causing scrotal swelling Common in newborns; usu. disappears w/out intervention in 1st yr of life (comm v. non-comm) May form in reaction to infection or injury Will cause scrotal transillumination |
|
|
Spermatocele |
Abnormal sac which develops in epididymis Usu. filled with clear/milky fluid Usu. asymptomatic unless it becomes large enough to cause discomfort |
|

|
Spermatocele Can be observed via transillumination or ultrasound Typically asymptomatic May require surgical removal if it becomes large enough to cause discomfort |
|
|
Testicular cancer |
Seminoma is most common malignant testicular tumor--usu. seen in men in their 20s-30s Typically painless on presentation Will not transilluminate (solid mass) Easily curable if detected early May present w/ mets (10%): supraclavicular lymph nodes, pulmonary symptoms, back/bone pain |
|

|
Seminoma Most common malignant testicular cancer; usually seen in men in their 20s and 30s |
|
|
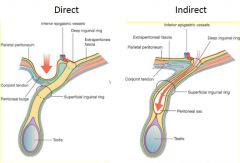
Direct inguinal hernia |
Usu. due to weakness in abdominal wall mms. Hernia proceeds directly through abd. wall; does not traverse inguinal canal Hernia sac will touch side of examining finger in inguinal canal Rare in children |
|
|
Direct and indirect inguinal hernia routes |
|
|
Indirect inguinal hernia |
Goes down inguinal canal, "indirectly" into scrotal sac Hernia sac will touch tip of finger in examination of inguinal canal Most common type of hernia in newborns/babies |
|
|
Femoral hernia |
More common in women Occurs through femoral canal, inferior to inguinal ligament (differentiates it from inguinal hernia) |
|

|
Femoral hernia More common in women Through femoral canal Inferior to inguinal ligament |
|
|
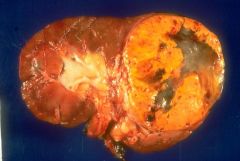
Palpable kidneys: differential diagnoses |
1. Adult Polycystic Kidney Disease (APDK) 2. Renal cell carcinoma (also assoc. w/ varicocele) 3. Angiomyolipoma (tubular sclerosis) 4. Xanthogranulomatous pyelonephritis (rare) |
|
|
Renal cell carcinoma Associated w/ varicocele in males Will present with palpable kidney |
|

|
Adult polycystic kidney disease 30s-40s: Will present w/ palpable kidney, flank pain, hematuria, renal stones Autosomal dominant: PKD1 (more severe), PKD2 75% hypertensive Cysts in multiple viscera (30%-liver) 5-10%: intracranial aneurysm (subarachnoid) 50% have renal failure by age 60 |
|

|
Angiomyolipoma (tubular sclerosis)
Benign tumor Mixed tissue findings on CT |
|
|
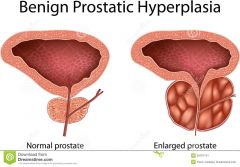
Benign prostatic hypertrophy (BPH) |
Common in older men Presents w/: frequent urination, weak stream, incomplete bladder emptying, nocturia, intermittency, hesitancy Exacerbated by anticholinergics (benadryl, cogentin, etc.)--distended bladder, anuria Digital Rectal Exam: diffusely enlarged gland, rubbery consistency, non-tender |
|
|
Benign Prostatic Hypertrophy (BPH) |
|
|
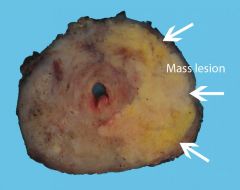
Adenocarcinoma of the prostate |
Common in older men Generally asymptomatic May present w/ mets (e.g. back pain--spine mets) May coexist w/ benign prostatic hypertrophy DRE: hard nodule |
|
|
Prostate adenocarcinoma |
|
|
Acute prostatitis |
Usu. presents as acute illness in young/middle-aged men Symptoms: fever, malaise, dysuria, pelvic/penile pain, obstructive complaints This is a medical emergency; give antibiotics DRE: tender, edematous gland |
|
|
Costo-vertebral angle tenderness |
Swelling of renal capsule; elicited by percussion w/ medial aspect of fist Due to pyelonephritis (most common), or hydronephrosis |
|
|
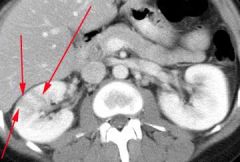
Pyelonephritis |
Usu. due to migrating UTI (cystitis), but can also arise from bacteria in bloodstream Presents w/ palpable kidney, radiating flank pain, fever, chills, and dysuria Can lead to sepsis, kidney failure, death Treat w/ antibiotics |
|
|
Pyelonephritis Striated nephrogram/CT imaging |
|
|
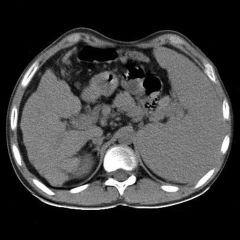
Hydronephrosis |
Typically due to obstruction in ureter May be due to congenital structural abnormalities (such as posterior urethral valves in males), injury, infection, or radiation exposure If left untreated, can lead to ESRD Increased incidence of UTIs may be only symptom of dysfunction early on |
|

|
Bilateral hydronephrosis |
|
|
Abdominal palpation findings |
1. Distended bladder (urethral strictures or BPH+anticholinergic medications)--intern's tumor 2. Splenomegaly (spleen will move with respiration; L kidney is retroperitoneal, will not move w/ resp.) |
|
|
Splenomegaly On palpation, will move with respiration |
|
|
Skin findings |
1. Impetigo (Staph aureus or Strep pyogenes; risk of post-strep glomerulonephritis) 2. Henoch-Schonlein purpura (IgA vasculitis; risk of glomerulonephritis) 3. Uremic frost |
|
|
Syphilis Stages |
Primary: painless, indurated chancre representing spirochete entry site (~21 days incubation) Secondary: skin manifestations 2-10 weeks after chancre; often palms/soles; may show constitutional findings Tertiary: neurologic, cardiovascular |
|
|
Impetigo |
Skin infxn caused by Staph aureus or Strep pyogenes (GAS) Flaccid vesicles and bullae-->rupture = honey-colored crusts Commonly seen in low-SES school children in warm climates If GAS-->risk for post-strep glomerulonephritis |
|

|
Impetigo |
|
|
Henoch-Schonlein purpura (HSP) |
IgA vasculitis Usu. in kids Assoc. rash, glomerulonephritis, risk for GI bleed (20-30%) Skin finding is palpable purpura |
|

|
Henoch-Schonlein Purpura IgA vasculitis Rash, acute glomerulonephritis, risk for GI bleed Palpable purpura--not specific to HSP; look for RBC casts in urine |
|
|
Uremic Frost |
Relatively uncommon; only occurs w/ serum BUN >200 mg/dl Crystallized urea from swet Indicates severe renal failure |
|

|
Uremic frost (crystallized urea) BUN >200 mg/dl Severe renal failure |
|
|
Urine sediment types |
1. Oxalate crystals 2. Struvite crystals (aka: triple phosphate) 3. White cell casts (aka: coarse granular cast) 4. Uric acid crystals 5. Red cell casts |
|
|
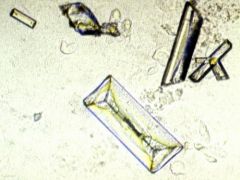
Oxalate crystals |
"Rhomboid crystals" Ethylene glycol (EG) ingestion Ethylene glycol-->oxalate w/ EtOH-dehydrogenase catalyzing step 1 of 2-step rxn EG metabolites-->renal failure, acidosis Treat w/ fomepizole+dialysis (old tx was EtOH) Methanol also-->increased AGAP acidosis/retinal injury (but no oxaluria) |
|

|
Oxalate crystals Ethylene glycol (anti-freeze) ingestion Acidosis + renal failure Tx: fomepizole+dialysis |
|
|
Struvite lithiasis (aka: triple phosphate) |
Composed of Mg, ammonium, and phosphate Occurs w/ upper UTI with urease-producing organism (PROTEUS)+alkaline urine Shaped like "coffin lids" Grows rapidly, forming branching structure ("staghorn" calculus) w/in renal pelvis & collecting system X-ray: dense calcific lesion |
|
|
Struvite crystals Struvite lithiasis Proteus most common organism involved Urease-producing organism |
|

|
Staghorn calculus Often associated with struvite lithiasis Proteus infection in upper UT |
|
|
Uric acid crystals in urine |
Usu. seen in acidic urine of patients w/ hyperuricemia, uric acid renal stones, and/or gout |
|

|
Uric acid crystals Seen in acidic urine Hyperuricemia, uric acid renal stones, &/or gout |
|
|
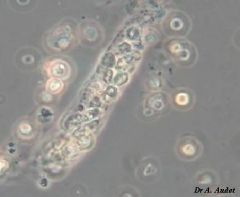
White cell cast (coarse granular cast) |
Assoc. w/ inflammation in kidney tubules Usu. acute pyelonephritis |
|
|
White cell casts (coarse granular casts) Assoc. w/ inflammation of kidney tubules, acute pyelonephritis |
|
|
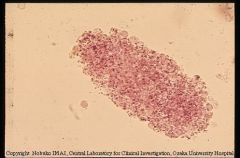
Red cell cast |
Specific for acute glomerulonephritis |
|
|
Red cell cast Assoc. w/ acute glomerulonephritis (not 100% sensitive) |
|
|
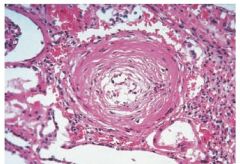
Malignant hypertension |
Nephrosclerosis due to vascular damage, fibrin and platelet deposits-->inadequate blood perfusion (DON'T GIVE DIURETICS--already intravascular volume depletion) Ischemia-->activation of renin-aldosterone system-->angiotensin II-->renal vasoconstriction, further elevation of blood pressure Onion-skin glomerular lesions on kidney biopsy; visual impairment/papilledema |
|
|
Onion-skin lesion Typical finding in disorders which cause thrombotic microangiopathy Malignant hypertension, scleroderma renal crisis, eclampsia, etc. Arterioles would show damage w/ necrosis |
|
|
Lindsay's nails ("half-and-half" nails) |
Assoc. w/ renal failure
Metab. acidosis + hyperkalemia Hyperkalemia-->peaked T waves, QRS complex widening-->sine wave pattern-->death Address w/ IV calcium, lower serum [K] w/ insulin/glucose, albuterol, dialysis |
|

|
Lindsay's nails Associated w/ hyperkalemia, renal failure |
|
|
Xanthogranulomatous pyelonephritis |
Due to recurrent UTIs Associated w/ palpable renal mass |
|

|
Xanthogranulomatous Pyelonephritis Will present w/ palpable kidney Due to recurrent UTIs |
|
|
Tumor Lysis Syndrome |
Risk usu. following chemo for some aggressive cancers (~58%) Lysis-->spillage of intracell'r contents (K, P, uric acid)-->acute tubular necrosis + hyperkalemia Acute tubular necrosis: urine shows "muddy brown casts" After 2-3 days: Intravasc. volume overload, high AGAP metab. acidosis, uremia |