Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
Iatrogenic Illness among elderly
|
- Nearly 1 in 3 acutely hospitalized patients
- Adverse drug reactions are the most common iatrogenic illness - Results are function losses and increased costs |
|
|
Polypharmacy Stats for old people
|
AV 4.5 prescription drugs
12-17 prescription annually Use over 25% of all prescription meds Use 3.5 OTC |
|
|
5 I's associated with the elderly
|
Iatrogenic
Immobility Incompetence Impaired Homeostasis Incontinence |
|
|
Illnesses associated with elderly
|
Infection
Physical (trauma) Immunologic Neoplastic Geriatric (metabolic) Iatrogenic Psychiatric Idiopathic |
|
|
|
|
|
Mrs. J is an 89 year old woman with
hypothyroidism. She is on replacement with Synthroid 0.20 mg qd. She recently had a hip fracture which was repaired. She has noted weight loss, jittery feelings, and malaise. Which of the following pharmacokinetic changes with aging accounts for her fracture and symptoms? |
Volume of Distribution
|
|
|
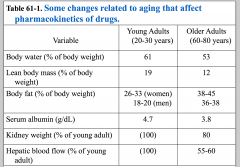
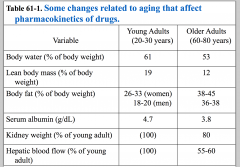
Factors affecting drug disposition and response in the elderly
|
Distribution:
- Body composition - Reduced total body water - Reduced lead body mass/kg - Body weight - Increased body fat - Protein binding - Reduced serum albumin |
|
|
Mr S is a 72 year old man with severe COPD. He is
O2 dependent. He is on multiple bronchodilators. You are also forced to use steroids to treat his symptoms and cannot wean him. You decide to use high dose vitamin D to try to antagonize the effects of the steroid on bone. On an office visit, his wife reports he is lethargic. |
Pharmacokinetic change seen with aging that can affect vit D -- can lead to hypercalcemia.
Lethargy can be due to hypoxia, enemia, muscargenics (due to bronchodilators) |
|
|
|
|
|
The use of triazolam has been associated with what side effect?
|
Daytime drowsiness
|
|
|
1. Which of the following medications should be avoided as hypnotics in older patients?
a. diazepam b. flurazepam c. oxazepam d. lorazepam |
Diazepam and Flurazepam -- long acting
Phase I Metabolism (affected by aging) |
|
|
Phase II: Hepatic Metabolism
|
- Mediated by cytoplasmic enzymes
- Addition of water soluble moieties to drug (e.g: acetylation, glucuronication, sulfation, glycine conjugation) - Not commonly altered with age |
|
|
Mrs K is an 80 year old woman living in a nursing home with dementia. She spikes a 103 degree fever and is admitted to your service.
What are the considerations for Mrs K’s fever? |
Pneumonia
UTI Pressure Ulcer GI - C. diff B symptoms of lymphoma Pulmonary Embolus Autoimmune issues - RA |
|
|
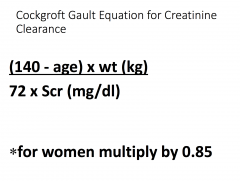
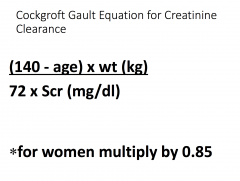
Mrs K has a serum creatinine of 1.0mg/dl. She weighs 72 kg. You feel she needs gentamicin. How do you go
about dosing her? How would your approach differ is she were 40 years old? How would you follow her? |
Creatinine clearance decreased with age. Less drug is excreted with age. Decreased dosage for older people.
If you dose her too high can result in nephrotoxicity (gentamicin is aminoglycoside) |
|
|
|
|
|
Pharmacokinetics
|
Processes of drug absorption, distribution and elimination from the body
|
|
|
Pharmacodynamics
|
Target organ sensitivity to drug
|
|
|
Pharmacodynamic issues
|
- Receptors and receptor binding
- Translation of receptor initiated response into biochem rxn - Cellular response to biochemical event |
|
|
Mr T is a 75 year old man with new onset of atrial
fibrillation. You decide to cardiovert him. You use I.V. valium for sedation. You aim to achieve a blood level of drug that has worked well for you in the past. To your surprise, his plane of anesthesia is deeper than you predicted. He has respiratory failure and must be intubated and placed on a ventilator. What went wrong? Does the problem have a pharmacokinetic basis? |
Organ sensitivity to drug
Pharmacodynamics helps to explain the problem |
|
|
Increased pharmacodynamic sensitivity
|
Benzos
Anesthetic Opioids Dihydropyridines (transient in naive patients) |
|
|
Mr Y is a 78 year old man who has lung cancer
with metastases to the brain. You administer decadron with good effect and he receives radiation for palliation. Two weeks later, he becomes lethargic. What pharmacodynamic effect of aging might explain his picture? |
Counter regulatory to insulin. Can become hypoglycemic and that made him lethargic
|
|
|
Decreased pharmacodynamic sensitivity
|
Can affect the beta adrenergic receptor
|
|
|
Mrs B is an 88 year old woman with pernicious anemia, arthritis, atherosclerotic heart disease, and hypertension. She is managed with vitamin B12, ibuprofen, aspirin, nifedipine, and a thiazide diuretic. She has noted some insomnia so flurazepam is prescribed. She gradually becomes depressed. Her appetite is poor and she is non functional. Emergent ECT is considered.
What would be your approach to this patient? |
Flurazepam caused the side effect.
|
|
|
|
|
|
Avoiding adverse drug effects in older patients
|
- Start low, go slow
- Watch for key risk factors: -- greater than or equal to 6 concurrent chronic diagnoses -- greater than or equal to 12 doses of meds per day -- greater than or equal to 9 drugs -- 1 prior drug reaction -- low body weight or bmi -- age 85 or older -- estimated CrCl < 50 mL/min ** worry most about GFR, then vol of distribution, then hepatic metabolism |
|
|
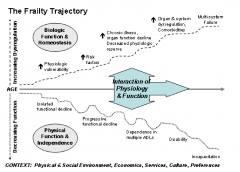
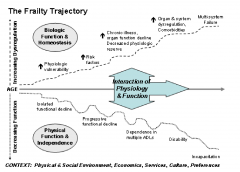
Primary Frailty
|
Intrinsic to the aging process
A physiologic process with mult-factorial conrtibuting cases |
|
|
Secondary Frailty
|
Associated with progression or end-stage of chronic progressive disease associated with inflammation and wasting:
For ex: - HIV/AIDS - COPD - Cancer - Dementia |
|
|
Domains affects by Frailty
|
Balance
Motor speed and processing Strength and endurance Nutrition Mobility Physical activity Cognition |
|
|
Frailty Syndrome
|
As an operational phenotype:
Shrinking: weight loss: unintention > 10lbs per year and sarcopenia Weakness Poor endurance Low Activity |
|
|
Sarcopenia
|
Low muscle mass: > 2SD below the mean measured in young adults aged 18-39
Low muscle function defined by low gait speed - rate of < 0.8 m/s in the 4 m walk test |
|
|
Weakness
|
Grip strength: lowest 20% by gender and BMI
|
|
|
Poor Endurance
|
Exhaustion by self-report
Slowness: walking time/15ft - slowest 20% by gender and height |
|
|
Low Activity
|
Caloric intake - lowest 20$
- Males < 383 Kcal/wk - Female < 270 Kcal/wk |
|
|
Scoring of frailty
|
Greater than or equal to 3 items = frail
1-2 : hypothesized "pre-fail" 0 : robust |
|
|
|
|
|
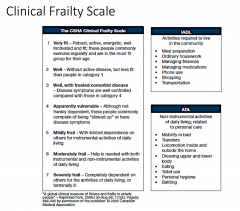
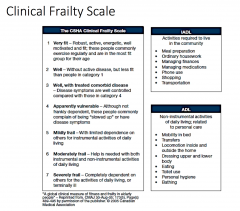
Rockwood Frailty Index
|
Accumulation of comorbidities
|
|
|
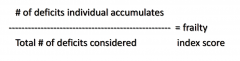
Frailty Index
|
accumulation of deficits. “Studies of frailty as deficit
accumulation demonstrate remarkable consistency in how deficits accumulate with age, the limit to how many things can go wrong, and how deficit counts change over time.” |
|
|
Comorbidity Accumulation
|
Highest weight on sensory loss and self-perceived health
Next highest on loss of ADL abilities - "disability" Next is systemic dysfunction - either diagnosed comorbidities like PD, or functional complaints |
|
|
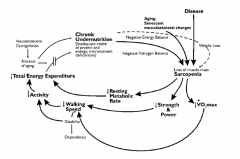
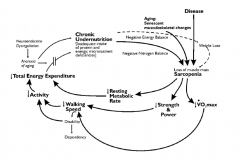
Proposed Pathophysiology of Frailty
|
Balance between stressor reactions of senescence or apoptosis across the musculoskeletal, immunologic, and neuroendocrine systems.
|
|
|
Musculoskeletal pathophysiology of frailty
|
• Decreased skeletal muscle mass
• Decreased VO2 max • Decreased strength and exercise tolerance • Diminished thermoregulation • Decreased energy expenditure and resting metabolic rate • Diminished muscle innervation • Decreased glucose uptake |
|
|
Immunologic Pathophysiology of Frailty
|
• Immunologic
• Decrease: • IgG • IgA • IL-2 • Mitogen response • Increase: • IL-6 • IL-10 • CRP |
|
|
Neuroendocrine Pathophysiology of Frailty
|
• Decrease:
• GH • IGF1 • Vitamin D • Estrogen / Testosterone (DHEA-S) • Increased • Insulin resistance • Cholecystokinin • Sympathetic tone • Steroid dysregulation |
|
|
|
|
|
Gavrilov and Gavrilova – reliability theory.
|
• Aging is the progressive accumulation of random damage to a complex system of
redundant parts. • Accumulation of damage and defects over time (aging) reduces this redundancy until the system becomes a series of elements connected in series. • The system’s loss of redundancy and resilience lead to vulnerability from external or internal stressors. • Loss of adaptability reduces responses to stressors to the equilibrium, eventually pushing systems (organs) to failure thresholds with an increased risk of adverse outcomes. • THIS IS FRAILTY |
|
|
Co-occurance Secondary Fraily
|
Interplay and co-occurence of multiple diseases, particularly
• Myocardial infarction • Angina • CHF • Claudication • Arthritis • Cancer • Diabetes • Hypertension • COPD |
|
|
Symmorphosis
|
• The multisystem interplay and “coadjustment” of different organs and functions relative to energy available for an organism.
• Example: exercise increases O2 requirement above baseline, with resultant changes in cardiac output, capillary density, hematocrit, muscle mitochondrial count and capacity. This is measured as VO2 max. |
|
|
Causes of Frailty
|
Genetic
Disease and Injury Lifestyle Aging Rate of Change |
|
|
|
|
|
At risk populations for aging
|
- Female
- AA - Low Education - Low Income - Poorer Health - Increased comorbid chronic disease - Increased disability - Impaired cognition - Increased depressive symptoms |
|
|
Defined Risk Areas
|
Falls
Hospitalization Disability Death |
|
|
Assessment of Frailty
|
• Medical domain
• Chronic illnesses • Falls • Medications • Cognitive/psychiatric domain • Cognitive impairment / dementia • Delirium • Depression • Substance abuse • Functional domain • Sensory deficits - especially vision and hearing • Slowed gait, weakness, and decreased physical activity • ADL and IADL function • Weight loss / malnutrition • Social domain • Social history |
|
|
Frailty Exam
|
General Exam with additional focus on:
Neuro-cognitive: cognitive testing, depression screens • Sensory: vision, hearing • Function: strength (especially thigh muscles and grip), range of motion (shoulders, hips, and knees), walking speed |
|
|
Labs to order
|
CBC
Metabolic Panel Inflammatory markers: CRP, ESR 25-OH D3 B12, folate TSH Any testing targeting chronic disease conditions |
|
|
Management of Frailty
|
Treat modifiable risk factor
Improve core manifestations -- exercise tolerance and endurance, physical activity, nutrition Minimize risks and stressors |
|
|
Treat frailty as?
|
Chronic Disease - focus on areas of impact
- Exercise programs - Comorbid disease risk factor improvement - Optimize access to nutrition and socialization Frailty is a syndrome Frailty is dynamic |