Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
146 Cards in this Set
- Front
- Back
|
anterior thoracic cage
|
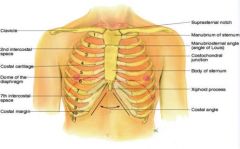
-suprasternal notch
-sternum (manubrium, body, xiphoid process) -manubriosternal angle (angle of louis) -costal angle -ribs |
|
|
manubriosternal angle aka "angle of louis"
|
-elevated part of sternum where manubrium meets the body of the sternum
-continuous w/ 2nd rib--2nd intercostal space is right below this rib -corresponds w/ upper atria of the heart -where trachea bifurcates |
|
|
What is a normal costal angle? What would be abnormal?
|
< 90
> 90 may indicate emphysema; barrel chest increases this angle |
|
|
How many ribs?
|
We have 12!
1-7 are directly attached to sternum via cartilage 8, 9, 10 fuse with the above ribs; "false ribs" 11, 12 are floating ribs w/ no anterior connections |
|
|
posterior thoracic cage
|
-vertebra prominens (C7)
-spinous processes -inferior border of scapula is ~7/8th rib -12th rib- palpate midway b/w spine and side to find " free tip" *C7-T4 is usually palpable |
|
|
anterior reference lines
|
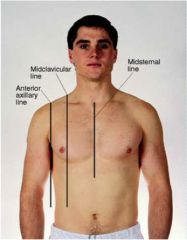
anterior axillary, midclavicular, midsternal
|
|
|
posterior reference lines
|
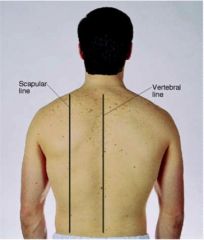
scapular, vertebral
|
|
|
lateral reference lines
|
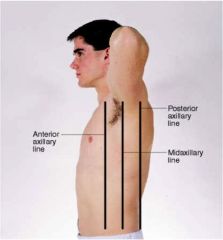
anterior axillary, posterior axillary, midaxillary
|
|
|
thoracic cavity
|
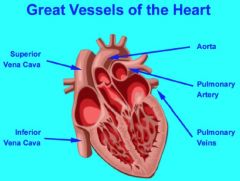
1/ mediastinum- esophagus, heart, trachea, great vessels (aorta, vena cavae, pulmonary artery)
2/ R pleural cavity 3/ L pleural cavity |
|
|
everything you wanted to know about lungs
|
2 lobes on left; 3 lobes on R
R side is shorter (b/c of liver) L side is narrower (b/c of the heart) anterior landmarks-- apices of lungs are above clavicle base of lungs rest on diaphragm ~6th rib posterior landmarks-- apex is C7 base is T10 During inspiration, lungs will expand to T12 when listening anteriorly- upper lobes when listening posteriorly- lower lobes (easier to hear congestion when patient is sedentary) |
|
|
Where do you auscultate RML?
|
laterally, more anterior
|
|
|
visceral v. parietal plurae
|
visceral lines the lungs
parietal lines chest walls *pleural cavity is filled w/ moisture and allows lungs to deflate/inflate (-) pressure holds lungs against the chest walls |
|
|
purposes of respiration
|
*respiration is the physical act of breathing
1/ supply O2 to body for energy production 2/ remove CO2 as waste product 3/ maintain acid-base balances of arterial blood 4/ maintain heat exchange |
|
|
What happens to the thoracic cavity during inspiration and expiration?
|
During inspiration, thoracic cavity has (-) pressure, diaphragm descends. Intercostal muscles are used.
Expiration is passive; diaphragm relaxes, creating (+) pressure, and air expels. |
|
|
subjective questions for respiration
|
-cough
-dyspnea -orthopnea (need pillow to sleep) -chest pain w/ breathing -hemoptysis -hx respiratory infections -hx smoking -environmental exposure |
|
|
What does a dry cough indicate? What about a congested cough?
|
dry cough- cardiac
congested cough- bronchitis pneumonia |
|
|
parasimal nocturnal dyspnea
|
patient lying flat at night and suddenly needs to sit up due to SOB; related to fluid accumulation in lung
|
|
|
barrel chest
|
thorax is squared off
AP transverse is 1:1 e.g. emphysema *normal AP transverse is 1:2 |
|
|
pectus excavatum v. pectus carinatum
|
pectus excavatum- sternum indented
pectus carinatum- sternum extended usually cosmetic but can affect heart and breathing |
|
|
scoliosis v. kyphosis
|
scoliosis- spine is curved from side to side
kyphosis- hunchback, usually due to aging |
|
|
pink puffer v. blue bloater
|
pink- emphysema; tripoding due to barrel chest--lungs are always inflated
blue- COPD, chronic bronchitis; decreased lung capacity *smokers will have combination |
|
|
respiration patterns
|
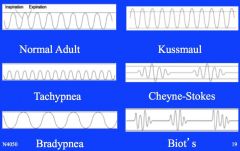
tachypnea- RR > 20; exercise, fever, pneumonia
bradypnea- RR < 12; drugs, increased intracranial pressure kussmaul- faster than normal, deep hyperventilation; anxiety, fear, diabetic ketoacidosis cheyne-stokes- waxing and weaning w/ periods of apnea; ESRD, CHF, increased intracranial pressure biot's- irregular, shallow; brain trauma, heat stroke, end of life |
|
|
palpation: symmetric expansion of lungs
|
both hands on posterior chest w/ thumbs @ T9 or T10
thumbs should move apart symmetrically when patient takes a deep breath if not symmetrical, could be pneumonia or collapsed lung |
|
|
T/F. Sound is conducted better through a dense/solid structure than porous.
|
True
Therefore, anything that increases density of lung will increase fremitus. |
|
|
name a condition w/ increased tactile fremitus
|
pneumonia
|
|
|
name three conditions w/ decreased tactile fremitus
|
1/ pneumothorax
2/ lung collapse 3/ any sort of obstruction |
|
|
percussion
|
*intercostal space
*only good for 6-7cm; cannot detect small pneumonia, but if you need pleural infusion, want to percuss to outline the area *would only percuss if patient comes in with *start at apices of lungs and go side to side |
|
|
percussion sounds
|
resonance- healthy lung (louder, deeper sound; air allows it to move freely)
dullness- liver, heart, pneumonia (high, shorter sound) flat- bone |
|
|
expected notes on posterior chest
|
resonance cuts off ~T8
|
|
|
diaphragmatic excursion
|
should be 3-5 cm bilaterally; runners can be > 5 cm
|
|
|
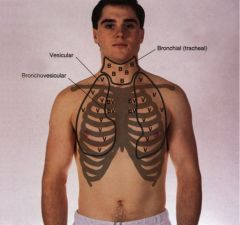
lung sounds
|
*use diaphragm
ratio represents inspiration : expiration vesicular; 2:1 bronchial vesicular; 1:1 bronchial; 1:2 |
|
|
adventitous breath sounds
|
crackles, rales, crepitations (fine to medium)
crackles, rales, crepitations (medium to coarse) wheezes (sonorous) wheezes (sibilant) stridor pleural friction rub |
|
|
crackles, rales, crepitations (fine to medium)
|
end of inspiration
air is colliding w/ secretions; possible in AM- if it doesn't go away, something could be in alveoli |
|
|
crackles, rales, crepitations (medium to coarse)
|
beginning of inspiration- sounds like velcro pulling apart
|
|
|
wheezes (sonorous)
|
low pitch, snoring sound aka rhonchi
|
|
|
wheezes (sibilant)
|
high pitch, musical, squeak
e.g. bronchitis, emphysema |
|
|
stridor
|
high pitch, loud, crowing during inspiration; something caught in trachea
e.g. child w/ croup |
|
|
pleural friction rub
|
"leather rubbing together"
e.g. pleural inflammation |
|
|
costal diaphragmatic recess
|
empty space under lung that can fill up w/ extra fluid
|
|
|
Where is the trachea?
|
trachea is anterior to esophagus and bifurcates below angle of louis
|
|
|
What is the difference between the R and L bronchus?
|
R bronchus is shorter, wider, and straighter making it easier to aspirate. L bronchus is at angle.
|
|
|
Explain the bifurcation of the bronchus. Where does gas exchange occur?
|
bronchus >> bronchiole >> alveoli
Gas exchange occurs in the alveoli. |
|
|
If concerned about pneumonia, what other sounds are you listening for?
|
transmitted voice sounds--normally is muffled, if you have consolidation, will be able to hear sound
bronchophony: "99" is clear rather than muffled egophony: "E" changes to "A" whispered pectoriloquy: whispered 99 is heard clearly rather than faint or absent sound |
|
|
T/F. Lungs are higher anteriorly than posteriorly.
|
True
|
|
|
percussion sounds, anterior chest
|
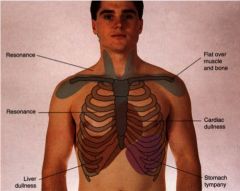
resonance @ apices, down to 6th rib
dullness @ heart/lung tympani @ stomach |
|
|
auscultation sounds, anterior chest
|
|
|
|
normal lung
|
trachea- midline
tactile fremitus- normal breath sounds- vesicular except over bronchi/trachea percussion- resonant adventitious sounds- none |
|
|
atelectasis
|
bronchial obstruction; diaphragm elevates to fill in space left by shrunken section
e.g. lobar obstruction trachea- shifted toward involved side tractile fremitus- absent breath sounds- absent when bronchial is plugged percussion- dull over airless area |
|
|
consolidation
|
alveoli consolidated w/ fluid, bacteria, RBCs, WBCs
e.g. pneumonia tactile fremitus- increased over involved area breath sounds- bronchial or bronchial/vessicular percussion- dull over airless area adventitious sounds- late inspiratory crackles |
|
|
bronchitis
|
bronchial inflammation w/ copious secretions; deflated alveoli
adventitious sounds- none OR scattered coarse crackles in early inspiration/expiration; wheezes and rhonchi |
|
|
emphysema
|
hyper-inflated lungs; overdistended alveoli w/ destruction of septa
tactile fremitus- decreased breath sounds- decreased/absent percussion- hyperresonant (tympani) adventitious sounds- none OR scattered coarse crackles in early inspiration/expiration; wheezes and rhonchi |
|
|
asthma
|
similar to bronchitis, but with more spasms
edema of bronchial mucosa, thick mucus tactile fremitus- decreased breath sounds- obsured by wheezes percussion- resonant to hyperresonant adventitious sounds- wheezes, possibly crackles |
|
|
pleural effusion
|
compressed alveoli
trachea- shifted toward opposite site of large effusion tactile fremitus- decreased/absent breath sounds- decreased/absent; bronchial sounds can be heard near top of large effusion percussion- dull to flat over fluid adventitious sounds- possible rub |
|
|
pneumothorax
|
lung collapse; air in pleural space due to rupture in lung wall, leak in chest wall
trachea- shifted toward opposite side if there is a lot of air tactile fremitus- decreased/absent over pleural air breath sounds- decreased/absent over pleural air (because lung is not inflated) adventitious sounds- possible pleural rub |
|
|
CHF
|
like pneumonia; dependent airways deflated, engorged capillaries, bronchial mucosa may be swollen
tactile fremitus- decreased adventitious sounds- late inspiratory crackles in dependent portions of lungs; possible wheezing |
|
|
external anatomy of breasts
|
between 2nd and 6th ribs
between sternal edge to mid axillary line nipple is just below center *tail of spence- superior lateral corner; projects up and into axilla |
|
|
What is breast tissue composed of?
|
-Glandular tissue; 15-20 lobes surrounding the nipple
-Fibrous bands i.e. suspensory ligaments (Cooper's) which support the glandular tissue -Fat/adipose tissue surrounds breasts (it's the most abundant) |
|
|
What happens to suspensory ligaments in Breast Cancer patients?
|
shortens & tightens
|
|
|
Where are most breast cancers found?
|
Females: upper outer quadrant (tail of spence)
Males: deep under nipple |
|
|
lymphatics of breasts
|
*drains into supraclavicular and infraclavicular
axillary nodes -central axillary -pectoral -subscapular -lateral |
|
|
T/F. Malignant tumors have increased blood supply due to increased venous return.
|
True
|
|
|
T/F. Sometimes there's a 2nd nipple following the milk line; it also has glands.
|
False; 2nd nipple has no glands
|
|
|
How long should a thorough breast exam take?
|
3 minutes
|
|
|
things to note about lump(s)
|
-location
-size -shape -consistency (firm, hard, soft) -motility -distinctness -nipple retraction -overlying skin -tenderness (cancer is not usually tender, although they can be) -lymphadenopathy |
|
|
T/F. Pituitary tumors usually result in milky discharge.
|
True
|
|
|
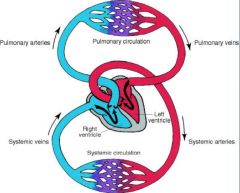
pulmonary/systemic circulation
|
|
|
|
Where is the heart?
|
2nd to 5th intercostal
R border of sternum to L clavicular line |
|
|
Where is the apical impulse (PMI)?
|
5th intercostal
midclavicular line |
|
|
compare the base/apex of the heart and lungs
|
lungs- apex top, base bottom
heart- base top, apex bottom |
|
|
Where are the R and L ventricle?
|
R ventricle- anterior
L ventricle- posterior |
|
|
great vessels
|
|
|
|
Where do the common carotid arteries go?
|
Common carotid arteries go to the brain.
|
|
|
layers of the <3
|
1/ epicardium- protective connective tissue covered by epithelium
2/ myocardium- thick muscle tissues responsible for pumping out blood 3/ endothelium- inner connective tissue w/ epithelium; purkinje fibers |
|
|
<3 internal anatomy
|
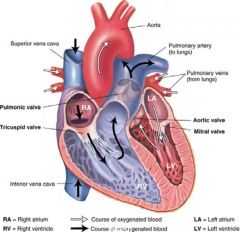
know the pathway of blood
|
|
|
compare the pressure of the R and L <3
|
R <3 is lower pressure system
L <3 is higher pressure system |
|
|
compare the L and R atriums
|
R atrium- thinner walls, reservoir
L atrium- thicker walls, pump |
|
|
systole
|
"lub"
S1- closing of the AV valves (MT) *ventricles contract -right ventricle pumps blood into pulmonary arteries via pulmonic valve -left ventricle pumps blood into aorta via aortic valve |
|
|
diastole
|
"dub"
S2- closing of semilunar valves (AP) *ventricles relax -blood flows from R atrium >> R ventricle via tricuspid valve -blood flows from L atrium >> L ventricle via mitral valve |
|
|
What is so special about S1?
|
It correlates to carotid pulse and QRS on ECGs.
|
|
|
What happens to the <3 of a HTN patient?
|
If diastolic is 100 (or generally high), it takes more isometric muscle contractions to open the valve--patient will develop L ventricular hypertrophy and the heart will go into failure.
|
|
|
After S2, what should you hear during diastole?
|
Usually very silent; will hear a rumbling if ventricles are resistant to filling (stiff due to hypertrophy or excess fluid); S3 and S4
|
|
|
S3 v. S4
|
S3- beginning of diastole
S4- end of diastole after atria contracts to get rids of blood (atrial systole or atrial kick) |
|
|
cardiac output (CO)
|
stroke volume x heart rate
stroke volume- the amount of blood in systole |
|
|
blood pressure
|
CO x SVR
SVR- systolic ventricular resistance in artery |
|
|
preload
|
length of which ventricular muscle stretch at the end of diastole
Starling's Law: greater stretch = stronger contraction |
|
|
afterload
|
opposing pressure ventricle has to generate to open aortic valve against aortic pressure
|
|
|
How much blood does a resting adult pump out every minute?
|
4-6 L
|
|
|
cardiac risk factors
|
smoking, poor diet, weight, family history, high BP & cholesterol, sedentary life style
|
|
|
cardiac subjective data
|
chest pain
dyspnea orthopnea cough fatigue cyanosis/pallor edema nocturia; CHF heart is too lazy to bring fluid back so it will go to kidneys instead |
|
|
T/F. Bruit can be heard if 30% of artery is occluded.
|
False; 70%
|
|
|
blood pressure
|
SBP- pressure generated by L ventricle during systole; LV ejects blood into aorta and arterial tree
DBP- pressure generated by blood remaining in arterial tree during diastole; ventricles are relaxed |
|
|
When will you see distention of neck veins?
|
R heart failure; fluid is backed up
> will also cause fluid overload in legs |
|
|
jugular venous pressure
|
-indicates how R <3 is working
-expressed as vertical height (cm) of column of blood relation to angle of louis -mean height of this column represents hydrostatic pressure within right atrium |
|
|
How deep is the right atrium to the sternum?
|
5 cm deep
|
|
|
How do you measure jugular venous pressure?
|
one at right atrium (5 cm)
one at height of distended vein, where internal jugular vein collapses ADD! *normal is height is 8-10 cm |
|
|
<3 auscultation sounds
|
@ AP, S2 > S1
@ TM, S1 > S2 @ erb's point, S1 = S2 |
|
|
Where is erb's point?
|
3rd intercostal
|
|
|
What are the three positions for auscultation? What purposes do they serve?
|
sitting, lying down, L lateral decubitus
sitting- base of heart is closer to chest wall; can hear AP better L lateral decubitus- L and R ventricles are closer; can hear MT, S3 and S4 better |
|
|
What are you inspecting for when looking at precordium?
|
Looking for heaves and lifts; if present--
@ tricuspid- RV hypertrophy due to fluid @ mitral- LV hypertrophy due to pressure |
|
|
S2 split
|
will hear aortic valve before pulmonic valve b/c there's more blood in R <3 than L <3
*normal during inspiration; heard @ base |
|
|
S3
|
ventricular gallop
"ken-tuc-ky" best w/ bell, L lateral decubitus position can be normal in children and young adults--will go away if they sit up; if this doesn't go away in adults >> CHF |
|
|
S4
|
atrial gallop
ten-ne-see best w/ bell may hear in athletes; usually in adults w/ <3 disease (stiffness due to CAD, systemic HTN) |
|
|
summation gallop
|
when you hear both S3 and S4
|
|
|
first signs of CHF
|
fluid overload, edema, neck distention, S3
|
|
|
rating of mumurs
|
i. barely audible
ii. clearly audible iii. moderately loud iv. loud, associated w/ thrill v. very loud vi. heard w/ steth off the chest wall |
|
|
mumurs
|
*turbulence through a valve
timing- systolic or diastolic? location- apex, base, sternal border? loundness/intensity pitch pattern- plateau, crescendo, decrescendo quality radiation- to neck? position of patient |
|
|
T/F. Diastolic murmurs are worse than systolic murmurs.
|
True
|
|
|
structural changes that may cause murmurs
|
stenotic valve- calcification can cause turbulence
incompetent valve- blood goes backwards (e.g. varicose vein or mitral valve) |
|
|
murmurs during systole
|
midsystolic ejection- aortic stenosis, pulmonic stenosis
pansystolic- mitral regurgitation, tricuspid regurgitation *aortic stenosis & mitral regurgitation are more common b/c it is a higher pressure system |
|
|
murmurs during diastole
|
diastolic rumbles- mitral stenosis, tricuspid stenosis
early diastolic- aortic regurgitation, pulmonic regurgitation |
|
|
pericardial rub
|
inflammation in lining of heart; treated w/ advil
|
|
|
ischemia v. infarction
|
ischemia- deficient supply of oxygenated blood
e.g. pain s/p exercise in smokers infarction- complete blockage |
|
|
T/F. Body has more arteries and they are closer to the skin.
|
False; veins
|
|
|
T/F. Veins and arteries run parallel.
|
True
|
|
|
mechanisms of venous flow
|
-contract skeletal muscles to milk the blood proximally back to heart
-intraluminal valves ensure unidirectional flow -patent lumen -inspiration: (-) thoracic pressure, (+) abdominal pressure helps blood get back to heart |
|
|
lymphatic ducts & draining patterns
|
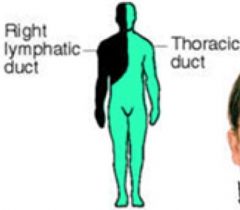
thoracic ducts drains most of body
R lymphatic duct drains R face, arm, mediastinum (heart and lung) |
|
|
functions of lymphatic system
|
-conserve fluid and proteins that leak out of capillaries
-immune system -absorb lipids from intestinal tract |
|
|
subjective PV
|
1/ pain or cramps
2/ skin changes on arms or legs 3/ swelling 4/ lymph node enlargement 5/ medications- oral contraceptives can cause more blood clots |
|
|
clubbing
|
greater than 160 degrees; normal is less
|
|
|
palpate aortic pulsation
|
patient should be supine, knees flexed
-press firmly on ABD left of midline, just above belly button -should be less than 3 cm wide *important to perform on older people (over 50), smokers, HTN |
|
|
inguinal lymph nodes
|
palpable--should be soft, mobile, less than 1 cm
*normal to feel them in groin area |
|
|
indications for ABD aneurysm
|
-if femoral is decreased compared to carotid
-if bruit is heard over ABD area -if aortic pulsation is greater than 3 cm |
|
|
edema
|
1+ to 4+ (if indentation remains)
causes-- 1/ deep venous thromosis (DVT)- blood clot in veins, swelling in one leg but not the other, femoral vein tenderness 2/ chronic venous insufficiency- previous DVT or varicose vein; skin will thicken and get brawny brown color 3/ lymphedema- lymph obstruction from inflammation or tumor, does not pit 4/ orthostatic edema- prolonged standing 5/ CHF- heart has decreased ability to take up fluid |
|
|
allen test
|
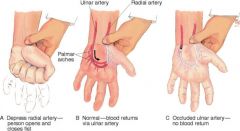
make sure ulnar artery is working if IV is on radial artery
|
|
|
manual compression test
|
compress vein
competent valves- if no wave is felt incompetent valve- if wave felt |
|
|
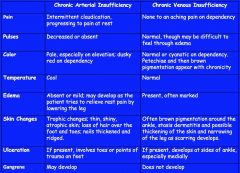
chronic arterial insufficiency v. chronic venous insufficiency
|
|
|
|
venous insufficiency
|

varicose veins- regurgitating blood back to legs
browning will lead to ulcer |
|
|
arterial insufficiency
|
when you raise feet, pallor
standing, erythema |
|
|
homan's sign
|
support thigh & bend knee slightly, abruptly dorsiflex ankle
(+) if patient experiences deep calf pain which could indicate blood clot in the calf 30% accurate |
|
|
What are better indicators of DVT?
|
red, hot, swollen behind knees
|
|
|
T/F. Heart and great vessels develop during first 3 to 8 weeks of gestation.
|
True
|
|
|
fetal circulation
|
lung sacs are collapsed and blood is oxygenated through the placenta
high pulmonary vascular resistance limits blood flow into the lungs and redirects it through the patent ductus arteriosus (PDA) to the descending aorta and lower body with a baby’s first breaths, pulmonary vascular resistance falls, causing a dramatic increase in pulmonary blood flow at birth, the right ventricle is larger than the left due to high pulmonary resistance during fetal life |
|
|
notable cardiac differences in peds
|
infant's <3 is proportionately larger to body
depended to HR and rhythm to maintain CO; cannot adjust (+) stroke volume myocardial muscle is less efficient >> more sensitive to volume pressure overload heart sounds are higher pitched, greater intensity |
|
|
maternal health history related to cardiac function
|
rubella is associated w/ <3 defects
lithium DM esp. if untreated |
|
|
What is one of the best health indicators in infants?
|
weight gain, height, BMI (starts at age 2), head circumference (until age 3)
|
|
|
How many bpm does an increase in one degree fahrenheit cause?
|
8-10 bpm
|
|
|
T/F. It is normal for pulse to increase w/ inspiration.
|
True
|
|
|
peds cyanosis
|
central- mouth
acrocyanosis- hands and feet, common in infants |
|
|
T/F. The infant heart is more horizontal.
|
True
-apex is higher, 4th intercostal space -PMI is usually palpated at an intercostal space higher (~3rd or 4th intercostal space) -apex is in the adult position (5th intercostal space) by age 7 |
|
|
T/F. You should palpate the radial and femoral pulses simultaneously.
|
True. Absence or weaker pulses in the lower extremities compared to the upper extremities is suggestive of coarctation of the aorta.
|
|
|
What is the most important assessment skill in evaluation of infants?
|
auscultation- sitting and lying down, use diaphragm
|
|
|
T/F. It is unusual for peds to have skipped heart beat, fast HR, or an extra beat.
|
False; it is NOT unusual
|
|
|
other usual findings for peds
|
-S2 split; w/ inspiration
-S3 is common; benign -murmurs are common; 50% are innocent |
|
|
What does S4 indicate in peds?
|
S4 is rare; decreased ventricular compliance
|
|
|
physiological murmurs in peds
|
innocent, systolic, vibratory, musical, does not transmit to other areas of heart
short duration grade III or less; do not increase over time |
|
|
pathological murmurs in peds
|
diastolic, loud
long duration greater than grade II usually caused by aortic or pulmonic regurgitation or mitral stenosis |