![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
hypospadias |
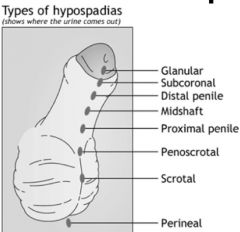
**abnormally palaced meatus **can cause infertility |
|
|
chordee w/ dorsal hood |
**crooked penis • congenital downward curvature due to strand of connective tissue b/w urethral opening and the glands • a/w hypospadias |
|
|
penile torsion |
• abnormal rotation of glands & urethral meatus • most often counterclockwise • not a/w functional abnormalities • treatment reserved for rotation >60° |
|
|
buried penis |
• normally developed • hidden beneath suprapubic fat pad; common in obese patients • consequence of penile skin being inadequately anchored to deep fascia of penis • a/w phimosis |
|
|
What is the best way to measure a buried penis? |
• use 10cc syringe • OR push down suprapubic fat |
|
|
micropenis |
**results from interruption of penile growth after 14th week gestation
• first 3 months of gestation- initial phase of penile development resultss from hCG • 4 mos-2 yrs- penis size (+) from testosterone
assessment-- • must stretch penis for length • penis smaller than 2SD • minimum of 2cm @ birth • 1 inch @ one year f/u |
|
|
harriet lane |

**measured when flacid & stretched |
|
|
physiologic v. pathologic phimosis |

physiologic-- • foreskin has not complete normal separation from epithelium of glans penis • treatment can include hydrocortisone
pathologic-- • can't be retracted after it has ben previously retractable • OR when foreskin cannot be retracted after puberty |
|
|
paraphimosis |
• foreskin is retracted & remains in proximal of glands penis & can't be pulled forward • can constrict penis & cause edema of the glans |
|
|
priaprism |
**prolonged penile erection; >4 hours
a/w-- • spinal cord trauma • sickle cell disease • leukemia • pelvic tumor or infection • penile tumor |
|
|
T/F. Priaprism is a urological emergency. |
True; needle is placed in corporal body to drain blood |
|
|
meatal stenosis |
**scarring & narrowing of urethral meatus
• delicate meatal edges lose superficial epithelial lining • occurs following hypospadias surgery, urethral instrumentation, & circumcision • narrow, high velocity urinal stream • dysuria |
|
|
cathing boys |
1 yr- 5 french 1-6 yrs- 8 frnch |
|
|
testes assessment |
• stand to side • ask patient to hold own penis • explain procedure • examine by grasping b/w thumb and first two digits • epipdidymis should be palpable, soft, w/ smooth ridge posterolateral to testes • testes should be same size |
|
|
vericoceles |
• usually L sided & not painful • not found in children < 9 y/o • if R sided, usually bilateral • a/w elevated temp in scrotum & testes • hallmark of testicular damage is testicle atrophy |
|
|
grading of vericocele |
**patient should be standing
• subclinical- not palpable or visible even w/ valsalva maneuver; demonstrable on dobbler • grade 1- can only be palpable when patient valsalvas • grade 2- nonvisible but palpable • grade 3- palpable vericocele feels like bag of worms; visible distention |
|
|
testicular torsion |
• more common in newborn & early stages of puberty • can occur perinatally if entire testis complex has not yet fused to scrotum >> testis, spermatic cord, and vaginalis twist en bloc • need surgery; ER/OR within 4 hours
clinical presentation-- • erythema/blue discoloration of scrotum >> apears as asymptomatic swelling • severe pain; can resolve spontaneously • n/v • child may c/o lower abdominal or inguinal pain due to embarassment |
|
|
cause of testicular torsion |
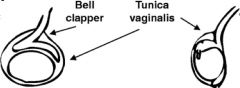
• bell clapper deformity caused by peritoneal investiture of testis lying on cord • abnormal insertion of tunica vaginalis >> spermatic cord can twist |
|
|
testicular torsion diagnosis |
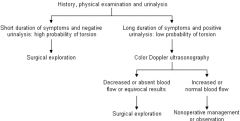
if suspect >> perform cremasteric reflex (-) >> urology will order US |
|
|
torsion of testicular appendages |
• more common in school age; 7-12 y/o • appendix testes is mullerian duct remnant located @ superior pole of testes; when it becomes twisted >> similar to spermatic cord torsion
clinical presentation-- • mild to moderate gradual pain • cremasteric reflex intact • affected testicle is tender @ top superior pole • blue dot sign • as pain increases, physical findings become less specific |
|
|
urethritis |
**inflammation of urethra w/o concurrent bladder infection |
|
|
epididymitis |
prepubertal boys-- • a/w urinary tract anomaly • if w/ UTI >> renal/bladder sonogram & bladder cystourethrogram to r/o structural problems
adolescents & young adults-- • r/t sexual activity • does not present w/ UTI |
|
|
urethral stricture |
fibrotic narrowing of urethra caused by scarring |
|
|
bladder outlet obstruction |
• diminished force & caliber of urinary stream • results from trauma or untreated/severe urethral infection |
|
|
cryptochidism |
**testicular maldescent **testes usually descend into scrotum @ 36 weeks; if not descended by 1 year >> refer
risk groups-- • first born • C-section • low birth weight • toxemia pregnancy • hypospadia • congenital subluxation of hip • winter |
|
|
true v. ectopic cryptorchidism |
• risk of malignancy/infertility if left in abdomen • examine in warm environment • milk testes |
|
|
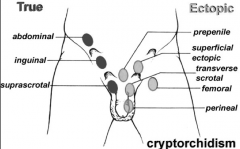
cryptorchid v. ectopic testes |
cryptorchid-- • descent arrested b/w normal pathway in its original abdominal location and scrotal position
ectopic-- • diverted from normal pathways • gubernaculum testes has abnormal insertion point, e.g. suprapubic, penile, femoral, perineal, contralateral position |
|
|
cryptochidism hormones |
hCG IM, RSH, LH, and testosterone >>if no increase in testosterone, no testes |
|
|
hernias |
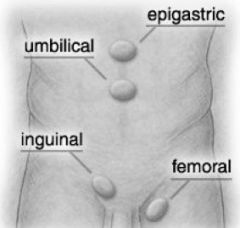
• common in males, R side, premies • iguinal & femoral hernias require surgery |
|
|
iguinal hernia |
due to failure of processus vaginalis to obliterate >> bowel forced into scrotum >> surgical repair
PE-- • suspect if child c/o intermittent groin swelling • crying/older child raising arms >> prominent lump • palpate testes • put arms over head |
|
|
hydrocele |
• accumulation of peritoneal fluid inside patent process vaginalis • a/w iguinal hernias • transillumination reveals homogeneous glow w/o shadows • usually resolves by one year |
|
|
communicating v. noncommunicating hydrocele |

communicating hydrocele-- • communicates w/ fluids of abdominal cavity
noncommunicating hydrocele-- • may be present @ birth or develop years later for no reason • usually remains the same size, very slow growth • needs surgical repair |
|
|
T/F. If varicocele is painful, patient should be reffered to urology. |
True |
|
|
examining the vagina |
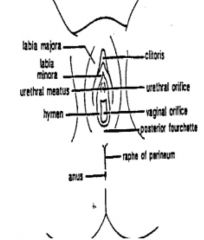
two positions-- • supine frog leg • knee chest
• pull down and out • no speculum needed unless unknown bleeding; speculum reserved for sexually active • physiological hymenal changes r/t pubertal development • look @ anal area • 2 openings; vaginal & urethral |