![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
357 Cards in this Set
- Front
- Back
|
primary HTN
|
occurs in 90%–95% of cases & tends to develop gradually over many yrs
risk factors: obesity, stress, sedentary lifestyle & smoking |
|
|
secondary HTN
|
appears suddenly & causes higher blood pressure than primary
has specific identified causes: renal disease, adrenal gland tumors, congenital coarctation, & obstructive sleep apnea meds that can cause: hormonal contraceptives, cold remedies, certain pain relievers & illegal drugs (cocaine & amphetamines) |
|
|
malignant HTN
|
a severe & sudden form of HTN
|
|
|
HTN (prognosis)
|
good if detected early & tx begins before complications develop
|
|
|
hypertensive crisis
|
severely elevated bp. may be fatal. are associated w/ evidence of target organ damage
|
|
|
HTN (s/s)
|
possibly none
blurry vision bruits over abdominal aorta or carotid, renal & femoral arteries confusion dizziness or lightheadedness edema elevated bp from baseline fatigue nocturia nose bleeds |
|
|
chest tube drainage system (requires nursing action)
|
continuous bubbling in the water–seal chamber indicates a possibility of an air leak & should be investigated promptly, intermittent bubbling in water–seal chamber means it's functioning properly
occasional bubbling in the suction chamber indicates something could be wrong (bubbling should be continuous) presence of small clots in tubing indicates nurse needs to "milk" tubing in direction of drainage chamber (important but not urgent) during transport, drainage system should remain as is and stay below pt's chest level to maintain tubing patency & prevent fluid from flowing back |
|
|
chest tube drainage system
|
tidaling (fluid fluctuation) in water–seal chamber indicates system is working effectively. drainage system should be placed below pts chest level
blocking (clamping) of the chest tubing can lead to a tension pneumothorax water–seal drainage: used to maintain neg intrathoracic pressure |
|
|
cardiac surgery (monitor for)
|
cessation of chest tube drainage may signal clotting which can lead to fluid build–up in the pericardium & cardiac tamponade
hypokalemia can cause dysrhythmias & even cardiac arrest. renal failure is a possible complication that is indicated by urinary output that drops below 25mL/hr but is not first priority temp of pt after cardiac surgery is usually low due to the bypass machinery & procedures used |
|
|
aminoglycoside [gentamicin sulfate] (AE)
|
nephrotoxic (especially in older)
|
|
|
cor pulmonale
|
R–sided heart failure w/ chronic respiratory failure. irritability & agitation are signs of air hunger
s/s: sob, cough, edema, & h/a (cor pulmonale w/ R ventricular failure) clinical manifestations: increasing edema of feet, distended neck vein, enlarged palpable liver, pleural effusion, ascites & heart murmurs, h/a, confusion & somnolence. pt will show wt gain especially when associated w/ COPD |
|
|
normal VS
|
bp: 120/80P: 60–100
R: 12–20 O2: 95%–100% |
|
|
thrombolytic therapy (contra)
|
contra: active, uncontrolled bleeding (pt is at risk for bleeding during therapy)
|
|
|
myocardial infarction (nursing action)
|
assess cardiac enzymes
|
|
|
pt w/ lung ca who develops superior vena cava syndrome
|
monitor neurological status which can be compromised by increased intracranial pressure & lack of o2 as a result of superior vena cava syndrome
|
|
|
super vena cava syndrome (nursing care)
|
monitor for dysphagia which is a clinical manifestation of edema associated. position pt based on facilitating breathing to improve comfort & decrease anxiety
|
|
|
sickle cell crisis (priority)
|
oral hydration is of highest importance during painful sickle cell crisis (dehydration is a common complication)
|
|
|
chronic anemia (s/s)
|
fatigue, weakness, dyspnea, & anorexia
|
|
|
delegation
|
pt education should not be delgated
|
|
|
pacemaker
|
telephone–based pacemaker monitoring is now available from home or at pacemaker clinic site
"loss of capture" place pt on L side before changing battery or generator or adjusting sensitivity "failure to sense" pacemaker is unable to detect an electrical conducted signal produced by the heart such as a P wave or QRS complex & ST segment "failure to capture" no response of the ventricle to the electrical conducting system VVI: ventricular paced, ventricular sensed, inhibited avoid high–output electrical generators b/c they can reprogram pacemakers. affected arm should NOT be raised above shoulder for 1 wk following placement |
|
|
angina
|
anginal cisode is often precipitated by insufficient coronary blood flow. coronary insufficiency results in a decreased o2 supply to meet an increased myocardial demand for o2 in response to a physical condition or emotional stress
exposure to extreme temps, especially cold, leads to increased o2 demand, as does exercise. pt should be encouraged to exercise but avoid adding stress of extreme temps. pt should balance rest w/ activity. sexual activity may trigger angina but proper planning can make it possible to continue |
|
|
congestive heart failure (infant)
|
tachycardia (rapid sleeping heart rate, greater than 160 in infants) is often first sign. tachypnea is also early sign (breaths greater than 60/min in infants)
|
|
|
digoxin (lanoxin)
|
.8 – 2.0 ng/mL
must be admin over min of 5 mins cardiac glycoside that slows the heart rate (monitor pulse!). useful for pts w/ HF who remain symptomatic w/ ACE inhibitors & beta blockers strengthens myocardial contraction, thus increasing cardiac output. useful to control ventricular response to a–fib ab pain in pt whose dose has been increased may indicate early toxicity early s/s of toxicity: fatigue, nausea, anorexia & depression. bradycardia & dysrhythmia may indicate toxicity vision changes** w/hold if HR is less than 60 or irregular. brush teeth after admin to avoid tooth decay quinidine, verapamil & amiodarone tend to increase serum digoxin concentration. metoclopramide tends to decrease serum dig lvls |
|
|
nifedipine (procardia)
|
calcium channel blocker that decreases contractility and o2 demand. prescribed for angina
|
|
|
nitroglycerin (nitrostat)
|
smooth muscle relaxation in blood vessels around the heart. reduces o2 demand and decreases L ventricular preload & afterload. causes vasodilation, decreases venous return, decreases cardiac output (reduces stroke volume).
prescribed for angina. pt should rest 15–20 after taking since fainting still may persist. tab sublingual q 5 mins up to 3, if pain persists go to hospital. replenish q 6 months & protect from light. |
|
|
propranolol hydrochloride (inderal)
|
beta blocker that reduces o2 demand, heart rate & bp. can produce insomnia in conjunction w/ mental depression.
commonly used to prevent migraines |
|
|
first action at onset of acute anginal pain
|
pt should sit or lie down to promote comfort & reduce chance of injury from a fall
|
|
|
coronary artery disease
|
cigarette smoking increases risk of clot formation by promoting platelet aggregation
|
|
|
infant w/ iron deficiency
|
infant can receive supplemental iron from iron–fortified cereals & formula
|
|
|
warfarin sodium (coumadin) therapy
|
take at the same time everyday. blood tests need to be scheduled regularly to ensure proper levels of anticoagulant. vegetables contain vitamin K which counteract the affects of warfarin
therapeutic level: prothrombin time (pt) is 11/2 to 2 times the control. higher values indicated increased risk of hemorrhage, lower values indicate increased risk of blood clot formation |
|
|
antihypertensive meds (se)
|
some have sexual SEs, nurse should indicate willingness to help help pt if they occur. meds can possibly be changed to avoid this
can cause postural hypotension or light–headedness w/ movement |
|
|
coupled PVCs
|
means that 2 premature ventricular contractions (beats) are occurring together. this increases the potential that the ventricles will not be fully repolarized, leading to a more dangerous arrhythmia
|
|
|
unifocal PVCs
|
occur in isolation & are not especially associated w/ serious arrythmias
|
|
|
premature ventricular contractions (PVCs) [ecg] |
have no associated p waves. most dangerous PVCs are r/t the t wave |
|
|
pernicious anemia
|
linked w/ vitamin b12 deficiency & in most cases is addressed w/ monthly injections
smooth, beefy red tongue children w/ persistent anemia: otitis media & URIs |
|
|
disseminated intravascular coagulation (DIC)
|
coagulation disorder characterized by formation of tiny clots in the microcirculation. normal hemostatic mechanisms are altered
clinical manifestation profuse hemorrhaging increased fibrin split products (norm hemostatic mechanisms are altered & many tiny clots form in microcirculation which cause increased fibrin split products in lab results) aka consumption coagulopathy & defibrination syndrome s/s: abnormal bleeding w/o hx of serious hemorrhagic disorder, bleeding in skin, excessive bleeding for IV site, n&v, chest pain, hemoptysis, epistaxis, seizures, oliguria, severe muscle back & abd pain, acrocyanosis, dyspnea, diminished peripheral pulses, decreased bp & mental status change dx: d–dimer (measure fibrin breakdown), considered more specific than fibrin degradation products in DXing DIC |
|
|
furosemide (lasix)
|
K wasting diuretic. muscle weakness is a sign of hypokalemia
bolus should take effect within 5 mins |
|
|
L–sided heart failure (s/s)
|
restlessness is one of the key features caused by decreased cardiac output
**exertional dyspnea frothy sputum sometimes develops & indicates pulmonary edema crackles indicate failure of L ventricle cough d/t congestion is one of the earliest signs |
|
|
anticoagulant therapy
|
long–term therapy: pt must consult physician before taking any meds or supplements
avoiding injury & bleeding is key |
|
|
atherosclerosis
|
a type of arteriosclerosis. primary cause of heart failure
embolization of plaque (fats, cholesterol & other substances) at increased risk when homocysteine is elevated |
|
|
myocardial infarction (MI)
|
**thrombic occlusion is the pathophysiological factor
irreversible cell damage (necrosis) of muscle tissue due to prolonged ischemia (20 mins) of the coronary artery ventricular dysrhythmias following thrombolytic therapy is generally considered a sign of reperfusion of coronary artery |
|
|
acute coronary syndrome
|
spasm of the peripheral arteries occur
|
|
|
ventricular tachycardia
|
wide & bizarre QRS complexes at regular intervals, pt may not have a pulse
suspected cause should be atrial fibrillation for v–tach w/ irregular rhythm after initial d–fib, 5 cycles of CPR alternating w/ rhythm check & d–fib are TX to convert v–fib to electrical rhythm that produces a plus |
|
|
premature ventricular contractions (cardia monitor)
|
wide & bizarre QRS complexes at regular intervals but pt may feel nothing or report a sense of that the heart has skipped a beat
|
|
|
ventricular fibrillation (cardiac monitor)
|
displays irregular waves w/ no recognizable QRS complexes & disorganized, quivering ventricular rhythm. pt will have no palpable pulse
|
|
|
sinus tachycardia (cardiac monitor)
|
usually displays normal QRS shape. pt will have a pulse
|
|
|
cardiac failure (nrsng intervention)
|
**support low arm of pt w/ pillows when head of bed is elevated 30 degrees. this decreases workload of the heart
**if pulse is less than 60 w/ atrial fibrillation, digitalis should be w/held, this may indicate that an AV conduction block is developing place pt in fowler's & give supplemental o2 to help breathe easily. organize activity for max rest periods. weigh pt daily, mntr for peripheral edema, mntr i&o, blood urea nitrogen & serum creatinine, K, NA, Cl & Ma levels. help prevent dvt from vascular congestion w/ ROM exercises |
|
|
decreased cardiac output r/t loss of mechanical pumping ability secondary to MI: cardiogenic shock as an affect of inadequate output of the heart following a myocardial infarction (s/s)
|
cyanotic nail beds, decreased urinary output & cool skin
|
|
|
transfusion reaction
|
stop transfusion & admin NS to maintain venous patency & then notify physician & follow protocols
|
|
|
pericarditis
|
inflammation of pericardium (fibroserous sac that envelops, supports & protects the heart)
*classic sign: friction rub to relieve pain place pt in fowler's position, if pt is able to sit upright and lean forward, chair rest may be appropriate. pain will be worse with lying down |
|
|
R–sided ventricular failure
|
dependent edema is key indicator
|
|
|
pt suddenly develops chest pain
|
applying o2 is first priority to minimize myocardial damage
|
|
|
plasma transfusion
|
platelet count is usually ordered 1 hr after & data on coagulation is reviewed to determine effectiveness of transfusion
|
|
|
anxiety
|
increases body's o2 demand
|
|
|
acute PAD
|
peripheral artery disease
requires emergent, aggressive tx to revascularize the extremity & prevent limb loss |
|
|
chronic PAD
|
peripheral artery disease
may vary in severity from mild to sever ischemia (w/ tissue necrosis) risk factors: smoking, aging, htn, hyperlipidemia, diabetes mellitus, & family hx of vascular disorder |
|
|
PAD (s/s)
|
peripheral artery disease
intermittent pain w/ exercise relieved w/ rest (chronic PAD), pain at rest, tingling, numbness, pallor, dependent rubor, cyanosis, coolness of affected extremity w/ delayed capillary refill, hardness of extremity from fibrotic changes, diminished or absent pulses, hair loss, thick nails, necrotic ulcers (severe ischemic disease), paralysis (severe ischemic disease) |
|
|
PAD (tx)
|
peripheral artery disease
bypass sx to revascularize limbs w/ acute occlusion or severe chronic disease, fibrinolytics to dissolve clot, balloon angioplasty, atherectomy or stenting, meds to lower cholesterol, antiplatelet meds, anticoagulants, control risk factors & regular exercise program |
|
|
PAD (nursing mngmnt)
|
peripheral artery disease
mntr affected limb frequently for changes, admin analgesics & anticoagulants if indicated, post–sx mntr limb for circulation & wound healing. encourage increasing activity as ordered & tolerated. emotional support & other appropriate support if amputation |
|
|
angina pectoris
|
a symptom of ischemic heart disease characterized by paroxysmal & usually recurring substernal or precordial chest pain or discomfort
caused by vary combo of increased myocardial demand & decreased myocardial perfusion |
|
|
angina (classifications)
|
chronic exertional angina, variant angina (prinzmetal's), unstable or crescendo angina, or silent ischemia
|
|
|
chronic exertional angina
|
(stable, typical)
usually caused by obstructive coronary artery disease chronic stable: characterized by exertional, rest relieved discomfort, located anywhere btwn umbilicus & ears that may be associated w/ numbness of arms or hands, generally caused by fixed obstructive atheromatous lesions, TXed w/ rest & nitrates during attacks & beta–adrenergic blockers for prevention |
|
|
prinzmental's (variant) angina
|
may occur in people w/ normal coronary arteries who have cyclically recurring angina at rest
characterized by resting discomfort. caused by coronary artery vasospasm, causes reversible ST–segment elevation during event TXed w/ CA channel blockers & nitrates, possibly beta–adrenergic blockers or coronary stenting if hard to deal w/ |
|
|
unstable angina
|
DXed in pts who report changing character, durtion & intensity of their painsi
|
|
|
silent ischemia
|
not all ischemic events are perceived by pts even though such events may have adverse implications for the pt
|
|
|
microvascular (cardiac syndrome X) angina
|
characterized by stable angina–like chest pain, caused by impairment of vasodilator reserve, poses no risk of cardiac ischemia b/c capillaries are too small to block oxygenation of cardiac cells, TXed w/ nitrates, beta–adrenergic blockers or calcium channel blockers
|
|
|
beta blockers
|
antianginal: reduce myocardial o2 demands by slowing heart rate & ^ force of myocardial contractions. rx long–term prevention of angina
anti–htn: clock catecholamine–induced ^ bp |
|
|
thrombolytics
|
complication: systemic bleeding
|
|
|
angiotension–converting enzyme (ACE) inhibitors
|
cough: most common se, usually resolves in 1–4 days after therapy begins
antihypertensive: decrease vasoconstriction & re–uptake of fluid ae: hyperkalemia (w/hold next dose & notify physician) enalapril: decreases ventricular remodeling which results in less than optimal ventricular function work by blocking conversion of angiotensin I to angiotensin II |
|
|
Angina (risk factors)
|
increases w/ age & predispositions to atherosclerosis (smoking, htn, diabetes mellitus, hyperlipoproteinemia)at younger age men are at greater risk for MI but for women prevalence of angina is higher w/ AM 40–74
|
|
|
angina (nursing assessment)
|
ask pt to describe past chest discomfort quality (aching, sharp, tingling, knifelike, choking, squeezing), location, radiation, precipitating factors, duration, alleviating factors & associated s/s during attack
often described as ache than actual pain, chest heaviness, pressure or tightness, squeezing, indigestion. typically located in substernal region or across anterior upper chest. often the pain is the size of a clenched fist & pt may place first over area of discomfort (levine's sign). sensation may radiate to neck, jaw, tongue; to elbow, write or hand; or to upper abd. discomfort is typically of short duration (3–5 mins) but can last up to 30 mins or longer. upon auscultation pt may have atrial or ventricular gallops |
|
|
angina (nursing dx)
|
altered tissue perfusion r/t narrowing of coronary artery & associated w/ atherosclerosis, spasms & thrombosis
|
|
|
angina (nursing planning & implementation)
|
pain mngmnt is priority not only for comfort but to also decrease myocardial o2 consumption. physician orders therapies that either decrease myocardial o2 demand or increase coronary blood & o2 supply
|
|
|
angina (diet)
|
low cholesterol, fat, calories & Na. drinks usually decaf & not too cold or hot
|
|
|
antianginals (beta–adrenergic blockers)
|
beta–adrenergic blockers: reduce myocardial o2 demands by slowing heart rate & increasing force of myocardial contractions
|
|
|
CA channel blockers (–olol)
|
antianginal. slow ventricular rate
dilate coronary & peripheral arteries & prevent coronary vasospasm, used when other drugs fail to prevent angina anti–htn: dilate arteries to lower bp & decrease cardiac contractility verapamil: used to control rapid ventricular response to either a–fib or atrial flutter metoprolol: avoid for those w/ asthma, can cause bronchospasms |
|
|
nitrates
|
antianginal
produce vasodilation, decrease preload & afterload, & reduce myocardial o2 consumption, ex: nitroglycerin (nitro–bid, nitrostat, nitrolingual), isosorbide dinitrate (isordil) |
|
|
abd aortic aneurysm
|
localized outpouching or abnormal dilation of a weakened arterial wall of aorta. when developing, lateral pressure increases, causing vessel lumen to widen & blood flow to slow. may result in hemodynamic forces that can create pulsatile stresses on weakened wall & press on small vessels that supply nutrients to arterial wall causing aorta to b/c bowed & torturous. aneurysm may rupture or tear suddenly, possibly causing death (medical emergency)
pt can feel heartbeat in and when lying down, and mass or throbbing signs of impending rupture: restlessness, lower back pain & hypotension or shock symptoms aortic dissection occurs when innermost lining of arterial wall separates from the other 2 to allow blood flow between layers rather than through the lumen of the artery, as is norm. this can completely obstruct true lumen of vessel. most classic sign of aortic dissection is "ripping" or "tearing" w/ abrupt onset |
|
|
abd aortic aneurysm [abd] (s/s)
|
lumbar pain radiating to flank & groin, systolic bruit over aorta, tenderness on deep palpation & palpation of abd throbbing
|
|
|
abd aortic aneurysm [ascending] (s/s)
|
bradycardia, different bp in R & L arm (more than 20 mmHg), jugular vein distention, murmur of aortic insufficiency, pain, pericardial friction rub & unequal carotid & radial pulses
|
|
|
abd aortic aneurysm [descending] (s/s)
|
dry cough, dysphagia, dyspnea & stridor, hoarseness & pain (sudden, between shoulder blades & chest)
|
|
|
abd aortic aneurysm (tx)
|
small, asymptomatic aneurysms: mntr q 6 mnths w/ ultrasonography, x–ray or ct
large or symptomatic aneurysms: resection or repair to prevent rupture mntr of bp & tx w/ antihypertensives as needed |
|
|
abd aortic aneurysm (nursing considerations)
|
allow pt to express fears & concerns. help pt identify effective coping strategies as they deal w/ dx
before elective sx, weigh pt, insert indwelling catheter & IV. assist w/ insertion of arterial line & pulmonary artery cath to mntr hemodynamic balance |
|
|
abd aortic aneurysm (tx in acute situation)
|
insert multiple large–bore IV to facilitate blood replacement, prep pt for impending sx, as ordered, obtain blood samples for kidney function tests, cbc w/ differential, blood typing & cross matching, & ABG levels, admin ordered meds. mntr pts cardiac rhythm & VS. assist w/ insertion of pulmonary artery line.
be alert for signs of rupture which may be fatal. watch closely for signs of acute blood loss (decreasing bp, increasing pulse & respiratory rates, restlessness, decreased sensorium & cool clammy skin) |
|
|
gangrene
|
death of tissue caused by lack of blood supply. poor circulation of lower extremities contribute to poor wound healing & development of gangrene which occur after prolonged, severe ischemia & represent tissue necrosis
Dry & Wet gangrene |
|
|
dry gangrene
|
occurs when portion of bodily tissue dies b/c blood supply has been decreased or completely cut off. it will NOT spread to other healthy tissue & infection is not present. usually slow process w/ affected area gradually b/c cold, discolored & eventually totally black. shrinkage & withering away of affected tissue occurs as tissue dies
|
|
|
wet gangrene
|
when dry gangrene b/c infected, often due to injury. infection cause tissue to die
|
|
|
dry gangrene (common causes)
|
arterial obstruction or occlusion of an artery caused by arteriosclerosis, diabetes mellitus, aids or blood clot; severe blunt trauma causing obstruction of artery; frostbite; diseases that affect blood vessels especially arteries (buerger's or raynaud's disease); traumatic occurrences (crushing injuries, fractures, burns & even injections into skin or muscles)
|
|
|
wet gangrene (common causes)
|
streptococcus (serious but rare form of infection w/ group A strephtococcus. necrotizing fasciitis or infectin of skin & tissues directly beneath skin) & staphylococcus
|
|
|
gas gangrene
|
most serious form of wet gangrene, often caused by clostridium bacteria (normally inhabitants of gi, repiratory & female genital tracts). initially characterized by red line on skin that marks border of affected tissues. onset of dry gangrene normally characterized by dull aching pain at site
dramatically sudden, rapid onset. frequently first noticed as marked swelling & either pallid or brownish–red colored area surrounding wound site. borders of infected area can expand w/in mins |
|
|
gas gangrene (s/s)
|
edema at injury site that expands quickly, pain in area surrounding injury, crepitus (bubbly) crackling sound hear upon palpation, pallor at injury site then increasingly dusky discoloration, low–grade – mod temp elevation
|
|
|
coronary artery disease [CAD]
|
occurs when arteries that supply blood to the heart muscle harden & narrow. result is loss of o2 & nutrients to myocardial tissue b/c of diminished coronary blood flow. reduction in blood flow can lead to coronary syndrome (angina or mi)
|
|
|
CAD (s/s)
|
possibly none, abnormal stress test or echocardiogram findings, angina, typically w exertion of stress, uncontrolled htn & diabetes mellitus, & major complications (acute coronary syndrome, heart failure, arrhythmias or sudden death)
|
|
|
CAD (tx)
|
drug therapy: angiotensin–converting enzyme inhibitors, thrombolytics, diuretics, glycoprotein IIb/IIIa inhibitors, nitrates, beta–adrenergic or CA channel blockers, antiplatelet, antilipemic, antihypertensive drugs
coronary artery bypass grafting (cabg) angioplasty arthrectomy stent placement to maintain patency of reopened artery lifestyle modifications to limit progression of CAD: smoking cessation, exercising, maintain ideal body wt & eating low–fat, low–sodium diet |
|
|
CAD (nursing considerations)
|
during anginal episode: mntr bp & hr. 12–lead elecrtocardiogram before admin nitro or other nitrates. record duration of pain & amount of meds to relieve & accompanying symptoms.after cardiac cath: mntr catheter site & check for distal pulses
after percutaneous transluminal coronary angioplasty (ptca) & intravascular stenting: maintain heperinization, observe for bleeding at site, keep affected leg immobile & chek for distal pulses. precordial blood must be taken q 8 hrs for 24 hrs for cardiac enzyme levels. complete bld count & electrolyte levels are monitored after rotational albation: mntr pt for chest pain, hypotension, coronary artery spasm & bleeding from cath site. provide heparin & antibiotic therapy for 24–48 hrs as ordered after bypass sx: mntr bp, i&o, breath sounds, chest tube drainage & cardiac rhythm. watch for signs of ischemia & arrhythmias. mntr cap glucoase, electrolyte levels & ABGs. follow weaning parameters while pt is on mechanical ventilator. pt may need temporary epicardial pacing, especially if sx included replacement of aortic valve |
|
|
myocarditis
|
inflammation of myocardium (heart muscle) & is often asymptomatic w/ spontaneous recovery. may occasionally result in cardiomyopathy & heart failure
causes: infection, immune reactions (rheumatic fever), radiation therapy, toxins & alcoholism |
|
|
myocarditis (s/s)
|
fatigue, dyspnea, fever, mild chest soreness, tachycardia, palpitations, mitral murmur, pericardial friction rub (scratchy sound over intercostal space on L chest) & heart failure
|
|
|
myocarditis (dx test)
|
elevated CK–MB, WBC, eosinophil sedimentation rate (esr), positive blood culture, ecg, chest x–ray, echocardiogram & endomyocardial biopsy
|
|
|
myocarditis (nursing interventions)
|
admin antibiotics, diuretics, anitpyretics & possibly antidysrhythmics & anticoagulants, admin corticosteroids & immunosuppressants, admin o2 & provide rest
|
|
|
myocarditis (sx mngment)
|
often not necessary but may include temporary pacemaker, cardiac assist devices or transplantation
|
|
|
acute pericarditis
|
can be fibrinous or effusive w/ purulent, serous or hemorrhagic exudate. fluid buildup can cause pericadial effusion. if effusion builds up too rapidly, cardiac tamponade can occur
prognosis depends on underlying cause but is generally good w/ acute pericarditis unless constriction occurs |
|
|
chronic constrictive pericarditis
|
characterized by dense fibrous pericardial thickening which causes constriction of normal heart size & movement. this can lead to permanently reduced stroke volume & cardiac output.
|
|
|
acute pericarditis (s/s)
|
pericardial friction rub at L third intercostal space, sharp sudden pain usually starting over the sternum & radiating to the neck, shoulders, back & arms
|
|
|
chronic pericarditis (s/s)
|
ascites, peripheral edema, chest pain w/ exertion, dyspnea, fatigue & inspiratory jvd (kussmaul's sign)
|
|
|
pericarditis (tx)
|
bed rest as long as fever & pain persist, tx of underlying cause, nsaids, coricosteroids, antibacterials, antifungals, antivirals, partial or total pericardectomy, diuretics & pericardiocentesis
|
|
|
pericarditis (nursing considerations)
|
stress the importance of bed rest, assist pt w/ bathing if needed, place pt n upright position to relieve dyspnea & chest pain, provide analgesic meds to relieve pain & o2 to prevent tissue hypoxia, cardiac tomponade requires immediate tx so keep pericardiocentesis tray handy if suspect pericardial effusion, assess cardiovascular status frequently, reduce anxiety & allow pt to express concerns, reassure that restrictions are temporary, observe venipuncture site for signs of infiltration or inflammation, rotate venous access sites to reduce risk
|
|
|
endocarditis
|
infection of endocardium, heart valves or cardiac prosthesis resulting from bacterial or fungal invasion
infection causes fibrin & platelets to aggregate on the valve tissue & engulf circulating bacteria or fungi that flourish & form friable, wartlike vegetative growths on the heart valves, the endocardial lining of a heart chamber or the epithelium of a blood vessel growth may cover the valve surfaces causing ulceration & necrosis. they may also extend to the chordae tendineae, leading to rupture & subsequent valvular insufficiency, ultimately they may embolize to the spleen, kidneys, cns & lungs |
|
|
endocarditis (s/s)
|
weakness & fatigue, anorexia, arthralgia, intermittent fever that may recur for weeks (in 90% of pts), wt loss, loud, regurgitant murmur (petechiae), osler nodes & asymmetrical arthritis
|
|
|
endocarditis (tx)
|
long–term antibiotic therapy, adequate rest periods, aspirin or acetaminophen for fever & aches, sufficient fluid intake, corrective urgery if refractory herat failure develops or heart structures are damaged, replacement of infected prosthetic valve, prophylactic tx for high–risk individuals
|
|
|
endocarditis (nursing considerations)
|
stress importance of adequate rest, provide bedside commode, reduce anxiety & allow to express concerns, assess cardiovascular status frequently & watch for s/s of L–sided heart failure (dyspnea, hypotension, tachycardia, tachypnea, crackles & wt gain). watch for changes in cardiac rhythm or conduction, adimin o2 & evaluate ABGs to ensure adequate oxygenation, mntr pts renal status to check for signs of renal emboli & drug toxicity
|
|
|
rheumatic fever, heart/valve disease
|
inflammatory autoimmune disease that affects connective tissues of the heart, joints subcutaneous tissues & blood vessels of the cns
presents 2–6 wks following unTXed or partially TXed group A beta–hemolytic streptococcal infection of upper respiratory tract |
|
|
rheumatic fever, heart/valve disease (most serious complication)
|
rheumatic heart disease (affects cardiac valves, particularly the mitral valve)
pt is at high risk for new infection & worsening of problems r/t to heart & joint damage |
|
|
rheumatic fever, heart/valve disease (dx)
|
jones criteria
|
|
|
rheumatic fever, heart/valve disease (assessment)
|
low–grade fever that spikes in the late afternoon, elevated antistreptolysin 0 titer, elevated sedimentation rate, elevated c–reactive protein level, aschoff bodies (lesions) found in herat, blood vessels, brain & serous surfaces of the joints & pleura
|
|
|
rheumatic fever, heart/valve disease (nursing intervention)
|
control joint pain & inflammation w/ massage & alternating hot/cold applications as rx, provide bed rest during acute febrile phase, limit physical exercise in the child w/ carditis, admin antibiotics, salicylates, anti–imflamatory (meds should not be admin before dx b/c the mask polyarthritis), seizure precaution if child is experiencing chorea
|
|
|
kawasaki disease
|
mucocutaneous lymph node syndrome, acute systemic inflammatory illness, cardiac involvment is most serious complication, aneurysms can develop
|
|
|
kawasaki disease (assess)
|
acute stage: fever, conjuctival hyperemia, red throat, swollen hands, rash & enlargement of cervical lymph nodes
subacute stage: cracking lips, fissures, desquamation of skin on tips of fingers & toes, cardiac manifestations & thombocystosis convalescent stage: child appears norm but signs of inflammation may be present |
|
|
kawasaki disease (intervention)
|
mntr temp frequently, asses heart, extremities for edema, redness & desquamation, eyes for conjunctivitis, mucous membranes for inflammation, strict i&o, admin soft foods & liquids (neither too hot or cold), weigh daily, provide passive ROM exercises, admin meds & parent education
|
|
|
cardiac failure
|
syndrome characterized by myocardial dysfunction that leads to diminished cardiac output or frank heart failure & abnormal circulatory congestion
R–sided, L–sided, systolic or diastolic and acute or chronic |
|
|
cardiac failure
|
congestion of systemic or venous circulation may result in peripheral edema or hepatomegaly, congestion of pulmonary circulation may cause pulmonary edema. pump failure usually occurs in damaged L ventricle but may occur in R ventricle either as primary disorder or secondary to L sided heart failure. sometimes L & R heart failure develop simultaneously
|
|
|
L–sided heart failure
|
result of ineffective L ventricular contraction causing fluid to possibily accumulate & backing into L atrium & then into the lungs. may lead to pulmonary congestion or pulmonary edema & decreased cardiac output
|
|
|
L–sided heart failure (common causes)
|
L ventricular MI, htn & aortic or mitral valve stenosis or insufficiencey
|
|
|
L–sided heart failure (s/s)
|
dyspnea (initially on exertion), confusion, bibasilar crackles, cough, cyanosis or pallor, fatigue, muscle weakness and tachycardia
|
|
|
R–sided heart failure
|
result of ineffective R ventricular contraction
pedal edema (gen in heart failure but more suggestive of R–sided) |
|
|
R–sided heart failure (possible cause)
|
R ventricular infarction or pulmonary embolism. most common cause is profound backward blood flow due to L–sided heart failure
|
|
|
R–sided heart failure (s/s)
|
edema (initially dependent), generalized wt gain, hepatomegaly, jvd & ascites. n&v (from venous stasis & venous engorgment w/in the abd organs
hepatojugular reflex: hob @ 45 degrees, put pressure on R upper abd, liver, for 30–40 seconds |
|
|
systolic herat failure
|
L ventricle can't pump enough blood out to systemic circulation during systole & ejection fracture fails causing blood to back up into pulmonary circulation, pressure rises in pulmonary venous system & cardiac output fails
|
|
|
diastolic heart failure
|
L ventricle can't relax & fill properly during diastole & stroke volume fails. large ventricular volumes are needed to maintain cardiac output
|
|
|
acute heart failure
|
refers to timing of onset of s/s. & whether compensatory mechanisms kick in. fluid status is typically normal or low & sodium & water retention doesn't occur
|
|
|
chronic heart failure
|
s/s have been present for some time, compensatory mechanisms have taken effect & fluid volume overload persists. drugs, diet change & activity restrictions usually control symptoms
|
|
|
cardiac failure (tx)
|
tx underlying disorders may improve heart failure. lifestyle changes, meds
|
|
|
MI (defined by location of damage)
|
R coronary artery (rca) occlusion results in inferior MI or R ventricular infarction
L circumflex artery (cx) occlusion results in lateral wall infarction L anterior descending artery (lad) results in anterior wall infarction |
|
|
MI (defined by extent of damage) |
q–wave (transmural) damage occurs when all layers of myocardium are affected |
|
|
MI (result of damage)
|
infarcted myocardial cells release cardiac enzymes into the bloodstream (ck–mb, troponin). *troponin T & I levels are elevated 3–4 hrs following MI, peak at 4–24 hrs & remain elevated 1–3 wks
w/in 24 hrs, infarcted area b/c edematous & cyanotic w/in several days, leukocytes arrive & remove dead cells by wk 3, scar formation may inhibit contractility compensatory mechanisms may be enabled by body in attempt to increase cardiac output ventricular dilation may occur due to heart's remodeling process after MI |
|
|
schilling test
|
tests for vit b12 deficiency
requires urine produced over 24 hr period to be collected along w/ admin of radioactive & nonradioactive preparations of vitamin b12 |
|
|
deep vein thrombophlebitis (dvt)
|
primary sign is pain in affected area & unilateral edema
|
|
|
atropine
|
drug of choice for 3rd degree atrioventricular block (bradydysrhythmias, sinoatrial arrest & av block)
drug of choice for symptomatic sinus bradycardia (admin 0.5mg IV rapidly bolus q 3–5 mins to a max total of 3mg |
|
|
epinephrine
|
initial tx for ventricular asystole. increases cardiac output
|
|
|
lidocaine
|
**initial drug of choice for premature ventricular contractions (PVCs)
|
|
|
chronic arterial occlusive disease (teaching)
|
pt is very susceptible to tissue injury, daily walking program provides appropriate level of activity, elevating legs impedes arterial flow, keep legs dependent as much as possible
|
|
|
abdominal aortic aneurysm
|
abdominal throbbing is common complaint
severe back pain indicates impending rupture & need for emergency measures |
|
|
nicotine
|
increases risk for clots by increasing platelet aggregation & are a key factor in peripheral arterial disease
|
|
|
iron deficiency anemia
|
serum ferritin lvls will be low reflecting depletion of iron stores, serum hemoglobin will be low reflecting effect of depletion
long–term: smooth, sore tongue is characteristic, brittle nils & corner of mouth ulcers imferon (IM iron) given IM Z track method |
|
|
chronic arterial occlusive disease (manifestation)
|
diminished hair growth on extremities is indicative of arterial insufficiencycool skin, diminished or absent pulses is also typical
|
|
|
venous insufficiency (manifestations)
|
swelling of extremities
|
|
|
congestive heart failure CHF (normal values for adult)
|
pulmonary artery wedge pressure (PAWP): 4–12 mmHg
cardiac output (CO): 4–7L/min systemic vascular resistance (svr): 800–1500 dynes/sec central venous pressure (cvp): 0–8mmHg |
|
|
combo of nitro IV & dopamine
|
admin for cardiogenic schock
|
|
|
NSAIDs
|
admin to tx dressler's syndrome (pericarditis after myocardial infarction). if bacterial, admin antibiotics
|
|
|
morphine sulfate to tx acute myocardial infarction
|
drug of choice for MI to reduce preload & in turn decrease cardiac workload overall
|
|
|
idiopathic thrombocytopenic purpura (ITP)
|
**occurs after certain childhood illnesses. clinical manifestations: bruises especially over boney prominences
platelets are mistaken as a threat & gets attacked by immune system |
|
|
MI (rehab)
|
phase 1 rehab begins as soon as pt is hemodynamically stable (when medical tx has stabilized cardiac supply & demand)
period immediately following discharge from coronary care unit is later part of phase 1 rehab early period of convalescence home is part of phase II rehab phase III: pt may return to norm activity w/in 6–8 wks after MI |
|
|
cardiac system (physiological changes in adults)
|
may have enlarged L atrium & increased atrial irritability, slower SA node rate of impulse discharge, decreased conduction speed across AV node & increased interval for the heart rate to return to baseline after any elevation
|
|
|
digitalis (se)
|
nausea is fairly common. if combined w/ several other symptoms, it can be an early indicator of digitalis toxicity
|
|
|
pacemaker
|
designed to provide electric stimulus to heart by generating a pulse. tx dysrhythmias not demand problems
|
|
|
defibrilator
|
automatically delivers a countershock upon sensing ventricular fibrillation
|
|
|
balloon angioplasty
|
pacemaker is inserted into coronary artery where it is inflated & opens artery
|
|
|
nitroglycerin (use)
|
place 1 tab under tongue when pain begins
potency decreases over time, supply should be replaced w/in 6 mnths or less for long–term nitro therapy pt should take a tab if an angina–causing activity is planned pt may take 3 tabs in 5 min intervals. if pain is not relieved call for emergency medical services |
|
|
stage IV adenocarcinoma
|
indicates tumor has metastasized, gas exchange b/c impaired as cancerous tissues increase
|
|
|
tumor lysis syndrome
|
arises when contents of cells destroyed by chemo or radiation are released into the body causing electrolyte imbalances.
increasing fluids assists kidneys in flushing the material |
|
|
cachexia
|
weakness & wasting away for body due to chronic illness
|
|
|
lost chord club
|
support group of those who have had laryngectomies (removal of larynx including vocal chords)
|
|
|
abdominal–perineal resection for rectal CA
|
sidelying position in bed is resting position that is least likely to be uncomfortable or irritating while surgical wound is healing
|
|
|
wilm's tumor
|
palpation of abd may cause CA cells to migrate into nearby or even distant sites
|
|
|
radical prostatectomy
|
impotence is expected
a penile prosthesis can enable pt to achieve erection |
|
|
multiple myeloma
|
dx test: serum electrophoresis reveals excessive bence jones proteins
hypercalcemia is a common complication b/c breakdown of bone releases calcium into bloodstream. maintaining hydration is important to help prevent hypercalcemia |
|
|
nitrites & nitrates (cause risk of...)
|
associated w/ increased risk of CA
|
|
|
ileal conduit
|
appliance most typically last 3–7 days w/ leakage, should be changed before it leaks. to modify opening in skin barrier, open to a max of 1.6mm or 1/8inch larger than stoma
skin barrier between pts skin & appliance protects against infection & excoriation around stoma. tape is used around skin barrier but never directly on pouch |
|
|
colostomy sx
|
return of norm fecal output may take several days following sx. in 3–6 days colostomy will begin to function
dark red or black coloring of stoma may indicate infection edema at stoma site & small amount of drainage from stoma is norm postSX finding |
|
|
claudication
|
leg pain resulting from obstruction of blood vessels
intermittent claudication: pain in legs, edema & hair loss ABI <1.0 indicates possible claudication of peripheral arteries. used to assess degree of stenosis of peripheral arteries |
|
|
causes person to be more susceptible to CA
|
pts w/ genetic abnormalities are several times more susceptible
|
|
|
radiation therapy (diet)
|
high protein, high carb & low residue
it affects gi tract, diet should be highly nutritious but not irritating |
|
|
distant metastasis of a neuroblastoma
|
indicated by periorbital edema & exophthalmus
|
|
|
neutropenia
|
low absolute neutrophil count
greatest risk is infection |
|
|
colostomy
|
wash area w/ mild soap & PAT dry to prevent skin breakdown
pouch opening should be trimmed 0.3cm (1/8 inch) larger than stoma drainage bag should be emptied when 1/3 – 1/4 full. drainage pouch may not be needed if pt is able to learn an irrigation routine for emptying colon |
|
|
unilateral modified radical mastectomy
|
elevation of arm on affected side relieves pain after mastectomy
|
|
|
risk for infection (entry sites)
|
oral cavity, IV sites & perineum
|
|
|
combo chemo
|
uses drugs that target diff phases of cell cycle or have diff chemical action to increase the # of cells destroyed
|
|
|
internal radiation therapy (visitors)
|
no pregnant women! visitors must remain 6 feet from source of radiation
|
|
|
myocardial infarction (s/s)
|
crushing stubsternal chest pain that may radiate to L arm, jaw, neck or shoulder blades, n&v, cool extremities, diaphoresis, anxiety, elevated bp & pulse in early stage & jvd
many older adults don't have common signs of chest pain, instead dyspnea, fatigue & syncope. women & those w/ diabetes mellitus may experience dyspnea, back pain or be asymptomatic |
|
|
myocardial infarction (dx tests)
|
serial 12 lead ECG, serial cardiac enzymes (CK–MB, troponin), echocardiogram, nuclear imaging & cardiac cathm
|
|
|
myocardial infarction (nursing intervention)
|
w/in 10 mins of onset "MONA greets every client" (IV morphine, o2 2–3L/min, nitro if BP >90 systolic & aspirin)
continuous cardiac mntr, ECG, IV fibrinolytic therapy w/in 6 hrs, IV or SQ heparin, admin appropriate drugs in recovery stage, pt may need cardiac rehab & education (meds, diet, daily wt) immediate cardiac cath may be needed, CABG may be needed for multiple lesions or L main coronary artery disease |
|
|
aortic insufficiency
|
incomplete closure of aortic semilunar valve. usually caused by scarring or retraction of valve leaflet
s/s: blowing diastolic murmur or s3, cough, exertional dyspnea or chest pain, L–sided heart failure, pulsus bisferiens (rapidly rising & collapsing pulse), fatigue, weakness & palpitations tx: valve replacement, low NA diet, digoxin, diuretics, vasodilators, & ace inhibitors |
|
|
aortic insufficiency (nursing considerations)
|
stress adequate rest, provide bed–side commode, alternate periods of activity w/ periods of rest, place pt in upright position to relieve dyspnea & admin o2 to prevent tissue hypoxia
|
|
|
aortic stenosis
|
increased L ventricle pressure tries to overcome resistance of narrowed valvular opening. added workload increased demand for o2 & diminished cardiac output causing poor coronary artery perfusion, ischemia of L ventricle & L–sided heart failure
|
|
|
aortic stenosis (s/s & tx)
|
s/s: angina, palpitations, cardiac arrhythmias, exertional dyspnea, paroxysmal nocturnal dyspnea, L–sided heart failure, syncope & systolic murmur at base of carotids
tx: commissurotomy (child & no calcification), valve replacement in symptomatic or those at risk of L–sided heart failure, percutaneous balloon aortic valvuloplasty, antibiotic prophylaxis, digoxin |
|
|
aortic stenosis (nursing considerations)
|
stress adequate rest, provide bed–side commode, alternate periods of activity w/ periods of rest, keep pt's legs elevated while seated in chair to improve venous return to heart, place pt in upright position to relieve dyspnea & admin o2 to prevent tissue hypoxia, low NA diet
notify physician of change in peripheral pulses distal to the insertion site, in cardiac rhythm & vs & chest pain. |
|
|
mitral insufficiency
|
abnormality of mitral leaflets, mitral annulus, chordae tendineae, papillary muscles, L atrium or L ventricle can lead to mitral insufficiency
can start suddenly w/ characteristic sign of dyspnea. chronic mitral insufficiency is slow process accompanied w/ fatigue & insomnia s/s: angina, palpitations, fatigue, now–onset atrial fibrillation, orthopnea, dyspnea, systolic murmur, light–headedness, cough (especially when supine) & pitting leg edema |
|
|
mitral insufficiency (tx & nursing considerations)
|
tx: drugs to relieve symptoms, valvuloplasty, valve replacement
nursing considerations: provide periods of rest between activity, reduce anxiety, low–NA diet, mntr for L–sided heart failure, pulmonary edema, provide O2 to prevent tissue hypoxia mntr: vs, ABGs, i&o, daily wt, bld chemistry, chest xray & pulmonary artery cath readings |
|
|
mitral valve prolapse
|
click–murmur syndrome (d/t ascultatory sound)
one or both valve leaflets protrude into L atrium. occurs more commonly in women. typically bengin s/s: possibly none, chest pain, dizziness, heart murmur, palpitations, syncope, fatigue, dyspnea tx: beta blockers, aspirin, anticoagulants, valve repair or replacement |
|
|
mitral valve prolapse (nursing considerations)
|
provide rest between activities, reduce anxiety, low–NA diet, mntr vs, ABGs, i&o, daily wt, bld chemistry, chest xray & pulmonary artery cath readings
|
|
|
mitral valve stenosis
|
narrowing of valve by valvular abnormalities, fibrosis or calcification that obstruct blood flow from L atrium to L ventricle causing L atrial vol & pressure rise & camber dilates. greater resistance to blood flow causes pulmonary htn, R ventricular hypertrophy & R–sided heart failure. inadequate filling of L ventricle produces low cardiac output
|
|
|
mitral valve stenosis (s/s & tx)
|
s/s: holosystolic murmur at apex, angina, crackles, dyspnea, fatigue, hepatomegaly (R–sided heart failure), jvd, orthopnea, palpitations, peripheral edema, pulmonary edema & tachycardia
tx: anticoagulants, drugs for heart, synchronized cardioversion for atrial fibrillation & valvuloplasty or valve replacement |
|
|
mitral valve stenosis (nursing considerations)
|
stress adequate rest, reduce anxiety, upright position to relieve dyspnea, o2 to prevent tissue hypoxia, low–NA diet
|
|
|
cardiomyopathy
|
disease of heart where muscle tissue can't work properly or efficiently
primary: changes in heart muscles w/o specific cause secondary: involves other organs as well as the heart 4 types: dilated, restrictive, hypertrophic & arrhythmogenic R ventricular dysplasia |
|
|
dilated cardiomyopathy
|
result from extensively damaged myocardial muscle fibers. interferes w/ myocardial metabolism & grossly dilates all four chambers giving heart globular appearance & shape. poor prognosis
s/s: sob, orthopnea, dyspnea on exertion, paroxysmal nocturnal dyspnea, fatigue, dry cough at night from L–sided heart failure, tachycardia w/ irregular pulse (if atrial fibrillation exists), pansystolic murmur associated w/ mitral & tricuspid insufficiency, peripheral cyanosis, peripheral edema, hepatomegaly, jvd, wt gain from R–sided heart failure, s3 gallop tx: o2 therapy, ace inhibitors as 1st line, diuretics, digoxin if not responding to ace inhibitors & diuretic therapy, vasodilators, beta–adrenergic blockers (for mild or mod heart failure), antiarrhythmics, cardioversion, automatic implanted cardioverter defibrillator insertion, anticoagulants (w/ atrial fibrillation), revascularization, valvular repair or replacement, lifestyle mods, L ventricular assists device |
|
|
dilated cardiomyopathy (nursing considerations)
|
alternate rest & ADLs, provide active or passive rom exercises to prevent muscle atrophy, low–NA diet, mntr for progressive failure, mntr for compromised renal perfusion, admin o2 prn, wt daily, prevent constipation & stress ulcers
|
|
|
restrictive cardiomyopathy
|
restricted ventricular filling (from L ventricular hypertrophy) & endocardial fibrosis & thickening. severe & irreversible.
s/s: fatigue, chest pain, dyspnea, edema, high systemic & pulmonary venous pressure, liver engorgement, orthopnea, abd distention & palpitations tx: mngmnt of underlying cause, digoxin, diuretics, restricted–NA diet, oral vasodilators, pacemaker, cardiac transplantation if intractable disease |
|
|
cardiogenic shock
|
clinical syndrome of reduced perfusion to organs & tissues, hypovolemic shock, cardiogenic shock, anaphylactic shock, septic shock, neurogenic shock
s/s: tachycardia, restlessness, tachypnea, diminishing urine output, hypotension, cold clammy skin, loss of consciousness, shallow cheyne–stokes respirations & anuria (in late stages) dx tx: bld, urine or sputum cultures, SBC & ESR rates, hematocrit & coagulation studies, ABGs, chest xray, echocardiogram & ECG |
|
|
cardiogenic shock (nursing considerations)
|
tx underlying cause, maintain airway, IV fluids to help maintain bp, continuous hemodynamic mntring, & appropriate drugs for each type of shock
|
|
|
venous thrombosis
|
acute condition characterized by inflammation & formation of thrombus w/in a vein. damage to epithelial lining of vein wall causes platelets to aggregate & release clotting factors that cause fibrin in the blood to form a clot. superficial thrombophlebitis, dvt & pe
s/s: superficial: palpable induration fo affected vein, heat & redness along vein & pain & tenderness along vein | dvt: fever, chills, malaise, severe pain in affected extremity, sudden nonpitting edema of affected extremity, prominent superficial veins, erythema of affected extremity, cool, pale, edematous extremity tx: anticoagulants, thrombolytics, venal caval filter to prevent PE, bed rest & elevation of extremity, warm moise soaks to the area, analgesics prn, thrombectomy |
|
|
venous thrombosis (nursing considerations)
|
perform risk assessment for DVT on admissions. high risk pts admin prphylactic meds, admin anticoagulants & o2 therapy, measure girth of affected area, encourage ambulation when appropriate or limb exercise, elevate affected limb, mntr coagulation studies
|
|
|
cardiac tamponade
|
rapid, unchecked increase in pressure in pericardial sac. results from blood or fluid that accumulates in sac & compresses the heart which obstructs blood flow to ventricles & reduces amount of blood pumped
pulmonary artery wedge pressure (pawp) is typically increased. fever is not typical. s/s: falling bp, restlessness, & sob, narrowing pulse pressure s/s: 3 classic signs (beck's triad) 1. elevated central venous pressure w/ jvd 2. muffled heart sounds due to fluid accumulation 3. pulsus paradoxus (drop in systemic bp > 15mmHg) due to arterial compression during inhalation tx: o2, continuous ecg & hemodynamic mntrng, pericardiocentesis, pericardial window, pericardectomy, trial val lading w/ crystalloids, inotropic drugs, for post–traumatic injury (bld transfusion, thoracotomy, repair bldng), for heparin–induced tamponade (protamine sulfate), emergency resuscitation & for warfarin–induced tamponade (vit K) |
|
|
cardiac tamponade (nursing considerations)
|
after pericardiocentesis: reduce anxiety, mntr bp & cvp during & after. IV solutions as ordered to maintain bp. decrease in cvp & concomitant increase in bp indicating relieve of cardiac compression, admin o2 as needed
after thoracotomy: antibiotic, protamine sulfate or vit k as ordered. post–op mntr vs, ABGs, heart & breath sounds.maintain chest drainage system |
|
|
iron deficiency anemia
|
common world–wide. inadequate supply of iron for optimal formation of RBCs which produce small cells w/ less color on staining. insufficient iron stores lead to depletion of RBC mass & in turn decrease hemoglobin lvl & o2 carrying capacity of bld
causes: inadequate diet, iron malabsorption, bld loss, pregnancy, intravascular hemolysis & mechanical erythrocyte trama s/s: fatigue, inability to concentrate, h/a, sob, increased infections, pica, numbness of extremities, dysphagia, hx of menorrhagia, vasomotor disturbances, neuralgic pain, red swollen smooth shiny & tender tongue, mouth may be eroded, tender & swollen, brittle nails, tachycardia, increased cardiac output & o2 sat < 90% tx: iron replacement, parenteral iron, total–dose IV infusion of supplemental iron |
|
|
iron deficiency anemia (nursing considerations)
|
provide o2 therapy prn, assess family dietary habits, nonirritating foods due to sore mouth & tongue, analgesics, pt's drug hx (pancreatic enzymes & vit E interfere w/ iron metabolism & absorption), provide fx rest periods, admin total dose IV infusions of iron dextran in NS over 8 hrs, z–track injection for iron IM to prevent skin discoloration scarring & irritation from iron
|
|
|
megaloblastic anemia
|
cause by incomplete formation of RBCs result in gin large # of immature & incompletely developed cells. results from a deficiency of vit B12 & folic acid & can be result of a lack of intrinsic factor
s/s:fatigue, muscle weakness, loss of appetite, wt loss, diarrhea, nausea, tachycardia, smooth or tender tongue, tingling in hands & feet schilling test helps w/ dx (evals vit B12 absorption) |
|
|
pernicious anemia
|
chronic, progressive, microcytic anemia caused by deficient intrinsic factor which prevents absorption of vit B12. RBCs are defective as they mature w/o intrinsic factor
s/s: tingling & paresthesia of hands & feet, wt loss, anorexia, dyspepsia dx: bone marrow aspiration show increased megaloblasts, peripheral bld smear |
|
|
sickle cell anemia
|
congenital hemolytic disease from defective hemoglobin molecule that cause RBCs to become sickle shaped
s/s: Developing after 6 mnths old, chronic fatigue, unexplained dyspnea, joint welling, ching bones, chest pain, ischemic leg ulcers, ^ susceptibility to infection, hx of pulmonary infarctions & cardiomegaly, jaundice or pallor, small for age appearance in children, growth & puberty delays, spiderlike body build (narrow shoulders & hips, long extremities, curved spine & barrel chest), tachycardia, hepatomegaly, systolic & diastolic murmurs & avascular necrosis |
|
|
sickle cell crisis
|
hx of conditions or situations tat provoke hypoxia, sleepiness w/ difficulty waking up, severe pain, hematuria, pale lips tongue palms & nail beds, lethargy, istlessness & irritability, body temp > 104 or temp of 100 that persists for 2 days or longer
tx: polyvalent pneumococcal & haemophilus influenzae B vaccine, anti–infective, chelating agent, analgesics, iron supplements, hydroxyurea to increase hemoglobin level, prophylactic penicillin, transfusion of packed RBCs, hematopoietic cell transplantation using sibling donors (curative potential) |
|
|
acute sequestration crisis
|
sedation & admin of analgesic, bld transfusion, o2 therapy, large amounts of oral or IV fluids
|
|
|
sickle cell anemia (nursing considerations)
|
HHOP: Heat, Hydration, Oxygen & Pain relief
in sudden development of painful priapism, reassure that episodes lasting 1–2 hrs are common w/o harmful effects, ensure pt receives adequate folic acid–rich foods & encourage adequate fluid intake to hydrate pt, warm compress on painful areas, bed rest w/ hob elevated to decrease tissue o2 demand, admin bld transfusions as ordered, w/ general anesthesia for sx, ensure pt received adequate ventilation to prevent hypoxic crisis, provide preop transfusion of packed RBCs prnpo |
|
|
polycythemia vera
|
aka primary poplycythemia, erythema, polycythemia rubra vera splenomegalic polycythemia & vaquez–osler disease. chronic myeloproliferative disorder characterized by RBC mass, leukocytosis, thrombocytosis & increased hemoglobin level w/ norm or decreased plasma vol
increase in rbc concentration in blood (due to body attempting to improve o2 carrying capacity) thicker than normal blood. onset is gradual & runs chronic but slowly progressive course. mortality is high if unTXed s/s: in early stages possibly no s/s, fullness in head, rushing in ears, tinnitus, h/a, dizziness, vertigo, epistaxis, night sweats, epigastric & join pain, scotomas, double & blurred vision, decreased urine output, pruritus, sense of abd fullness, pleuritic chest pain or L–upper quad pain tx: phlebotomy therapy (350–500mL of bld can be removed till pt's hematocrit is reduced to low–norm values, myelosuppressive therapy, radioactive phosphorus or chemo, pheresis technology that allows removal of RBCs, WBCs & platelets individually or collectively, admin cyproheptadine & allopurinol to reduce serum uric acid lvl |
|
|
polycythemia (nursing considerations)
|
keep pt active & ambulatory to prevent thrombosis, regularly examine for bleeding, give pt additional fluids to compensate for increased uric acid producion, small rx meals followed by rest period for those w/ symptomatic splenomegaly to prevent n&v, report acute abd pain immediately (may signal splenic infarction, renal calculus formation or abd thrombosis), check vs prior to phlebotomy & immediately following, have pt sit up for about 5 mins before walking to prevent vasovagal attack & orthostatic hypotension
|
|
|
hemophilia/hemophilia A
|
factor VIII deficiency, inhearied coagulation disorder. genetic disorder carried by females but mostly affects males
|
|
|
christmas disease/hemophilia B
|
factor IX deficiency, less common w/ similar s/s to hemophilia A
|
|
|
disseminated intravascular coagulation disorder
|
consumption coagulopathy. accelerates clotting which can cause hemorrhaging
|
|
|
thrombocytopenia
|
**most common coagulation disorder. lack of circulating platelets in bld. includes idiopathic thrombocytopenia
low bld platelet count, usually improves when underlying cause is TXed causes of thrombocytopenia: enlarged spleen, condition that involves bone marrow, pregnancy, idiopathic thrombocytopenic purpura (itp), autoimmune diseases, bacteria in blood, thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome, meds s/s: easy or excessive bruising, superficial bleeding, prolonged bleeding, spontaneous bleeding from gums or nose, blood in urine or stools, unusually heavy menstrual flow, profuse bleeding during sx or after dental work |
|
|
von willebrand's disease
|
hereditary disorder w/ prolonged bleeding time d/t clotting factor deficiency & impaired platelet function. most common hereditary coagulation disorder
|
|
|
hypoprothrombinemia
|
congenital deficiency of clotting factors that can lead to hemorrhage
|
|
|
hemophilia C
|
factor XI deficiency. afflicts 1 in 100,000 people & 2nd most common bleeding disorder among women
|
|
|
factor VII deficiency
|
serum prothrombin conversion accelerator (SPCA) deficiency. 1 in 500,000 people may be afflicted, often dx in newborns b/c bleeding into brain as result of traumatic delivery
|
|
|
myoglobin test
|
when elevated, first marker of cardiac injury following acute MI
|
|
|
high–sensitivity C–reactive protein (hs–CRP)
|
excess lvls may indicate increased risk of CAD
|
|
|
HDL
|
primarily protein
the higher the lvl the lower the risk of CAD |
|
|
LDL | VLDL
|
primarily cholesterol | primarily triglycerides
the higher the LDL | VLDL lvl the higher the incidence of CAD |
|
|
triglycerides
|
excess lvls identify hyperlipidemia in pts at risk for CADt
|
|
|
total cholestrerol
|
excess lvls may indicate hereditary lipid disorders, CAD
|
|
|
A–type natriuretic peptide (ANP) & B–type natriuretic peptide (BNP)
|
neurohormones produced from cardiac cells. help ensure cardiac equilibrium. disruption can trigger release of these hormones which act as natural diuretics & antihypertensives
***BNP help accurately dx & grade severity of heart failure*** |
|
|
electrolytes
|
K: 3.5–5 mEq/L (imbalance is life threatening)
NA: 135–145 mEq/L (low lvls indicate severe HF) CA: 8.2–10.3 mg/dl (high lvls cause cardiac toxicity & arrhythmias) Cl: 100–108 mEq/L (partners w/ NA, low lvls indicate HF & metabolic acidosis) MG: 1.3–2.1 mg/dl (high lvls cause ECG changes, ventricular tachy & v fib. low lvls cause ECG changes, bradycardia & hypotension) CO2: 23–30 mEq/L (bicarb, regulate kidneys, reduce thiazide diuretics) |
|
|
partial thromboplastin time, prothrombin time (pt) & activated clotting time
|
measures response to tx as well as screens for clotting disorder
|
|
|
international normalized ratio (INR)
|
generally viewed as best standardized measurement of PT. used to mntr warfarin tx.
increased INR may indicate DIC, cirrhosis, hepatitis, vit K deficiency, salicylate intoxication or uncontrolled oral anticoagulation |
|
|
12–lead ECG
|
can identify myocardial ischemia, MI, rhythm, conduction disturbances, chamber enlargement, electrolyte imbalances & drug toxicity
|
|
|
exercise ECG
|
assess heart's response to increased workload
|
|
|
holter monitor
|
ambulatory ECG. used to identify intermittent arrhythmias. usually 24 hrs (about 100,00 cardiac cycles)
|
|
|
cardiac cath
|
*assess coronary artery patency.
involves passing of cath through veins & arteries to measure heart chambers, lungs, blood flow btwn chambers, valve competence, cardiac wall contractility, artery pressures, intracardiac status, visualize coronary artery |
|
|
echocardiography
|
uses ultra–high fx sound waves to help examine size, shape & motion of heart's structures. special transducer is place over pts chest
TEE (transesophageal echocardiography) combo w/ endoscopy. used to dx thoracic aortic disorders, endocarditis, congenital heart disease, intracardiac thrombi & tumors. *NPO 6 hrs pre–op, continuous mntring, not heavily sedated |
|
|
anticoagulants
|
reduce blood's ability to clot. rx for mitral insufficiency & a fib or prevent clots in artery or vein
avoid vit K which can interfere w/ anticoagulation |
|
|
angiotensin II receptor blockers (ARBs)
|
antihypertensive: inhibit vasoconstriction, protect against renal failure in pts w/ type 2 diabetes
routine blood work is required |
|
|
diuretics
|
anti–htn: help kidneys excrete h2o & electrolytes which lower bp
|
|
|
antilipemics
|
lower cholesterol, triglyceride & phospholipid lvls. used in combo w/ lifestyle changes to decrease rick of CAD
|
|
|
inotropics
|
increase force of the heart's contractions
cardiac glycosides (slow heart rate & electrical impulse conduction through sinoatrial & AV nodes) & phosphodiesterase (PDE) inhibitors (short–term mngmnt of heart failure or long–term mngmnt for pts awaiting heart transplant sx) |
|
|
fibrinolytics
|
can dissolve clot or thrombus that caused acute MI, ischemic stroke or peripheral artery occlusion or pe. they can dissolve thrombi & reestab bld flow in arteriovenous cannulas, grafts & IV cath
|
|
|
ginseng (risk)
|
can increase risk of digoxin toxicity & can decrease clotting time
|
|
|
temporary transvenous pacemaker
|
provides more reliable pacing beat. this type of pacing is more comfortable for the pt b/c the pacing wire is insereted in the heart via a major artery
|
|
|
permanent pacing
|
self–contained device surgically implanted under pt's skin. allow's pt's heart to beat on it's own but keep heartbeat from falling below a preset rate. pacemakers tx persistent bradyarrhythmias, complete heart block, congenital or generative heart disease, stokes–adams syndrome, wolff, parkinson–white syndrome & sick sinus syndrome
pacing electrodes can be placed in atria, ventricles or both |
|
|
implantable cardioverter–defibrillators (ICD)
|
used for arrhythmia pacing, cardioversion & defibrillation. detects & terminates life–threatening episodes of v–tach & v–fib. some have the ability to pace atrium & ventricle & some perform biventricular pacing. leads are placed transvenously in endocardium of chambers and connects to generator box implanted in R or L upper chest near clavicle. if lethal rhythm is detected a shock is delivered to convert rhythm
|
|
|
coronary artery bypass graft (CABG)
|
surgery relieves symptoms of CAD & decreases rick of future heart attack or HF. performed either on pump or off pump (beating heart method or OPCAB). termed according to how many vessels are bypassed
monitor for complications of severe hypotension, decreased cardiac output & cardiogenic shock |
|
|
minimally invasive direct coronary artery bypass (midcab)
|
performed on a beating heart through a small thoracotomy incision, pt receives only R lung ventilation & drugs to slow heart rate & reduce heart movement during sx. procedure is minimally invasive so fewer complications & shorter hospital stay
pts eligible: proximal L anterior descending lesions & some lesions of R coronary & circumflex arteries |
|
|
heart transplantation
|
tx end–stage cardiac disease in pts who have poor quality of life & aren't expacted to survive for more than 6–12 months
pts must be TXed for rejection w/ monoconal antibodies & potent immunosuppressants that can increase the risk of life–threatening infection |
|
|
intra–aortic balloon pump conterpulsation (iabp)
|
temporarily reduces L ventricular workload & improves coronary perfusion. tx cardiogenic shock caused by acute MI, septic shock, intractable angina before surgery, intractable ventricular arrythmias, ventricular septal or papillary muscle ruptures & pump failure
|
|
|
enhance external counterpulsation (eecp)
|
provides pain relief for pts who suffer from recurrent stable angina when standard tx fail. noninvasive, increases o2–rich blood flow to heart & reduces heart's workload. can reduced angina pain, improve exercise tolerance & stimulate collateral circulation
|
|
|
percutaneous transluminal coronary angioplasty (ptca)
|
angioplasty, nonsurgical alternative to CABG. performed in cardiac cath lab under local anesthesia involves balloon–tipped cath to dilate blocked coronary artery
pts usually recuperate quickly, walking same day, return to work in 2 wks |
|
|
valve tx
|
prevent HF w/ valvular stenosis or insufficiency accompanied by severe, unmanageable symptoms
valvuloplasty (valvular repair), commissurotomy (separation of adherent, thickened leaflets of mitral valve), valve replacement (w/ mechanical or prosthetic valve) can cause serious complications: hemorrhage, stroke, bacterial endocarditis, valve dysfunction or failure. |
|
|
percutaneous balloon valvuloplasty
|
used when valve surgery isn't an option. used to enlarge orifice of stenotic heart valve
|
|
|
aortic endovascular stent graft
|
used to repair abd aortic aneurysm & other aneurysmal arteries by reinforcing vessel walls. fluoroscopic guidance is used to insert a delivery cath w/ an attached compressed graft through a small incision into the iliac or femoral artery. cath is advanced into aorta & positioned across aneurysm below the renal arteries.
helps present aneurysm from enlarging & possibly rupturing |
|
|
arterial bypass graft
|
serves to bypass arterial obstruction resulting from arteriosclerosise
|
|
|
embolectomy
|
remove an embolism from artery by balloon–tipped indwelling cath in artery & passing it through embolus, inflates balloon & w/draws cath to remove occlusion
|
|
|
vena caval filter
|
umbrella traps emboli originating from pelvis or LE in vena cava preventing them from reaching pulmonary vessels but allowing venous blood flow
|
|
|
ventricular assist device (VAD)
|
implantable device that consists of a bld pump, cannulas & pneumatic or electrical drive console. pump is synchronized to pt's electrocardiogram & functions as heart's ventricle. decreases heart's workload while increasing cardiac output
|
|
|
subjective hx
|
chest pain, persistent fatigue, dyspnea, palpatations, syncope
|
|
|
objective hx
|
diet, meds, past illness, personal habits, health hx
|
|
|
priorities
|
set based on assessment of pt needs
|
|
|
expected outcomes
|
care r/t to health promotion, health maintenance & health restoration
|
|
|
nursing interventions
|
on basis of estab standards to help pt move toward expected outcomes
|
|
|
implementation for cardiac nursing measures to...
|
improve circulation, cardiac output, increase o2 supply & decrease o2 demand, maintain bld vol, prevent complications, |
|
|
systole
|
action of heart chambers becoming smaller & ejecting blood
time between s1 & s2 |
|
|
normal conduction route of heart
|
SA node AV node to bundle of HIS to purknje fibers
|
|
|
apical (PMI)
|
left midclavicular line of chest wall @ 5th intercostal space. usually palpable. heart at first heart sound, lasting for only half of systole
|
|
|
myocardium
|
responsible for pumping action of heart
|
|
|
afterload
|
influences stroke volume
arterial vasoconstriction increases systemic vascular resistance which increases afterload |
|
|
following MI (fear of resuming sexual activity)
|
physiologic demands of sexual activity are equivalent to walking up 2 flights of stairs
|
|
|
peripheral & central cyanosis
|
peripheral: nails, lilps, earlobes & extremities
central: tongue & buccal mucosa |
|
|
pulse pressure
|
difference between systolic & diastolic pressure
|
|
|
diastole
|
time between s2 & s1
|
|
|
exercise stress test
|
up to 4 hr fast required, avoid stimulants prior
positive result: ST segment depression (ECG changes) |
|
|
hypo/hypervolemia | central venous pressure monitoring
|
hypovolemia may cause decreased CVP
hypervolemia may cause increased CVP |
|
|
pulmonary artery pressure monitoring (PAPM)
|
assess L ventricular function, dx etiology of shock & evaluating pt's response to medical interventions like fluid fluid admin & vasoactive meds
|
|
|
systemic arterial pressure monitoring (SAPM)
|
continually monitors BP
|
|
|
heart sounds |
s1 & s2 are norm & s3 could indicate L ventricular failure which is life threatening s3: heart w/ heart failure from increased filling pressure s3 gallop: best heard w/ bell & when pt is lying on L side |
|
|
cardiac health
|
exercise 3–4 times a week
|
|
|
friction rub
|
classic sign of pericarditis
auscultate: use diaphragm of stethoscope & have pt sit up & lean forward |
|
|
blood specimen for lipid profile
|
should be obtained after 12 hr fast. routinely done in morning
|
|
|
prolonged uncontrolled htn
|
can result in renal failure, MI, stroke, impaired vision, L ventricular hypertrophy, & cardiac failure
|
|
|
chlorothiazide
|
alcohol can potentiate SE of postural hypotension
|
|
|
smoking
|
doesn't not cause HTN but increase risk of heart disease
|
|
|
spironolactone (aldactone)
|
K–sparing diuretic, puts should avoid salt substitutes b/c they are high in K
|
|
|
NY heart association classification of heart failure
|
class I: ordinary physical activity doesn't cause undue fatigue, dyspnea, palpitations or chest pain
class II: slight limitations w/ ADLs but symptoms present w/ increased physical activity class III: marked limitations on ADLs class IV: cardiac insufficiency at rest |
|
|
sleeping w/ heart failure
|
cardiac workload is decreased & renal perfusion is increased & GFR is increased which may lead to nocturia
|
|
|
how to reduce venous return to heart
|
upright w/ LEs dependent
|
|
|
sodium bicarb
|
initial dose is 1mEq/kg IV
|
|
|
pulsus paradoxus
|
systolic bp markedly lower during inhalation (exceeding 10 mmHg)
|
|
|
v–fib or v–tach
|
immediate defibrillation
|
|
|
confirm placement of endotracheal tube
|
primary: visualization of ET through vocal chords, auscultation of BS in 5 areas of chest or bilateral chest expansion (over R & L chest w/ airflow heard & over stomach w/ no airflow heard)
secondary: CO2 detector |
|
|
t–wave
|
ventricular muscle depolarization, resting state
|
|
|
QRS complex
|
represents depolarization of ventricle (electrical activity of ventricle)
|
|
|
calculate heart rate on ECG
|
1500 divided by # of small boxes between R waves
|
|
|
3rd degree AV block
|
fewer QRS complexes than p waves
|
|
|
atrial fibrillation
|
s/s: palpitations, light–headedness, weakness & pulse deficit
loss of P waves w/ wavy baseline. QRS can be normal but heart rate ranges from 100–160bpm loss of atrial kick which means approx 30% less cardiac output |
|
|
amiodarone
|
promotes conversion to sinus rhythm
antidysrhythmic drug of choice for stable v–tach |
|
|
BP & Pulse Rate (indicate...)
|
hemodynamic effect of dysrhythmias
|
|
|
defibrillation
|
maintain good contact between paddles & pt's skin to prevent arcing, apply appropriate conducting agent between skin & paddles, d–fib must be in non–sync mode, "all clear" must be called 3 times
NEVER attempted on pt w/ pulse epinephrine is admin after 3 consecutive d–fibs to make it easier to convert dysrhythmia to normal sinus rhythm |
|
|
cryoablation therapy
|
uses cooled probe to create small scar on endocardium to eliminate source of dysrhythmias.
|
|
|
endocardium resection
|
involves peeling away a specified area of endocardium
|
|
|
electrical ablation
|
uses shocks to eliminate area causing dysrhythmias
|
|
|
radio frequency ablation
|
uses high–fx sound waves to destroy area causing dysrhythmias
|
|
|
cardiac conduction sx
|
considered in pots who don't respond to TXs for atrial & ventricular tachycardia
|
|
|
atrial flutter (stable, ARS narrow & R–R interval is regular
|
6mg of adenosine may be rapidly admin followed by 20mL saline flush & elevate arm. if rhythm doesn't convert to sinus rhythm w/in 1–2 mins admin 12mg bolus & repeat if needed w/in 1–2 mins
if adenosine fails to convert rhythm or if R–R interval is irregular then admin magnesium, diltiazem or beta–blockers |
|
|
atrioventricular nodal reentry tachycardia [avnrt] (no response to vagal maneuvers & meds)
|
cardioversion
|
|
|
ventricular asystole
|
TXed the same as pulseless electrical activity (PEA). focus on high quality CPR w/ minimal interruptions
CPR>intubation>epinepherine |
|
|
sinus bradycardia
|
most common arrhythmia that occurs during endotracheal suctioning. vagal stimulation (vomiting, suctioning, severe pain & extreme emotions may cause sinus bradycardia)
when experiencing syncope, weakness & low bp, prepare to have pacemaker inserted sinus & atrial rate of < 60 if pt suddenly develops bradycardia emergency pacing can be started w/ transcutaneous pacemaker which most defibrillators can now perform. if pt is alert, sedation & analgesia should be used |
|
|
ST segment
|
represents early ventricular repolarization. analyzed to id whether it is above or below isoelectric line which may be a sign of cardiac ischemia
|
|
|
catheter ablation therapy
|
uses radio frequency energy to ablate or burn accessory pathways or ectopic sites in atria, AV node or ventricles that cause tachyarrhythmias
|
|
|
decreased cardiac output r/t cardiac arrhythmias
|
sudden drop in bp & symptoms of hypoxemia (decreased mentation, chest pain & dyspnea)
|
|
|
ECG (pt prep)
|
slightly abrade skin w/ a clean, dry gauze pad & place electrodes on body at specific areas. abrading enhances signal transmission
|
|
|
raynaud's disease
|
intermittent arteriolar vasoconstriction causing coldness, pain & pallor of fingertips or toes. best when one has control of environmental temp & avoid exposure to extreme weather
|
|
|
arterial ulcers
|
small, circular, deep ulcers usually on tips of toes or in web spaces between toes. pain w/ rest may be present. gangrene & pale wound bed`
|
|
|
hydrocolloid dressing
|
maintains a moist environment & promotes granulation but should NOT be used if ulcer is infected
|
|
|
antiembolism stockings
|
prevent DVT by forcing blood into the deep venous system instead of allowing it to pool
|
|
|
venous ulcer
|
mod – heavy exudate, irregular wound margins, superficial wound bed & ruddy granular tissue
|
|
|
buerger's disease
|
spasms of arteries & veins occur primarily in LE. nonatherosclerotic inflammatory vascular disorder, typically occurs in young men who are cigarette smokers
tobacco is highly detrimental to this disease b/c it is a powerful vasoconstrictor s/s: toe & finger ischemia, advanced condition frequently have ulcerations on fingers & toes. complications include progressive ischemia leading to gangrene & amputatino |
|
|
virchow's triad
|
characteristics that put pt at significant risk for DVT
1. venous stasis 2. vessel wall injury 3. altered blood coagulation |
|
|
cellulitis
|
s/s: acute onset of swelling, localized redness, & pain. frequency associated w/ signs of fever, chills & sweating
|
|
|
lymphangitis
|
actue inflammation of lymphatic channels.characteristic red streaks that extend up arms or legs from infected wounds outlining the course of lymphatic vessels as they drain
|
|
|
unstable angina vs acute MI
|
acute MI involves myocardial cell death
|
|
|
tissue perfusion (complications in elders)
|
peripheral vascular resistance increases w/ age
|
|
|
acute MI
|
dysrhythmia is major cause of death
elevated ST segments in early phase indicate injury ST depression indicate ischemia Q waves reveal necrosis ventricular dysrhythmia can indicate hypoxemia, hypokalemia or reperfusion following thrombolytic therapy |
|
|
major precipitating factor of endocarditis in the US
|
IV drug use
|
|
|
pt w/ heart disease experiences dyspnea
|
this finding is not normal & indicates diminished cardiac reserve
|
|
|
JVD
|
jvd w/ HOB elevated indicates significant fluid overload
|
|
|
patent ductus arteriosus (pda)
|
significant murmur, signs of heart failure & bounding pulses
|
|
|
ventricular septal defect
|
will have symptoms of heart failure, abnormal ABGs, dusky skin color d/t pulmonary congestion
|
|
|
negative chronotropic effect
|
expected to decrease heart rate
|
|
|
pain not relieved by nitro
|
often associated w/ MI
|
|
|
ventricular dysrhythmias
|
most commonly caused by hypokalemia & hypoxemia
|
|
|
niacin therapy
|
helps to reduce LDL & raise HDL. can cause extreme flushing of the face, neck & ears. take 325mg of aspirin 30 mins prior to reduce flushing
ae: hyperglycemia |
|
|
heparin (antidote)
|
antidote: protamine sulfate
|
|
|
aspirin
|
for post–MI pts to help prevent reinfarction by decreasing platelet aggregation
|
|
|
BP cuff too large
|
bp would be falsely low
|
|
|
parasympathetic
|
influences decrease heart rate & slow conduction through AV node
|
|
|
transient ischemic attach (TIA)
|
effects are temporary.TIA is a warning that there is a problem w/ perfusion to part of the brain. TIA should initiate investigation into cause of disruption in perfusion
nursing dx: ineffective peripheral tissue perfusion |
|
|
carotid disease
|
meds: aspirin (anti–platelet), balloon angioplasty w/ carotid stenting,
|
|
|
carotid endarterectomy
|
plaque is surgically removed from carotid artery to reduce chance of stroke
priority assessment: ABCs, cranial nerve function assessment by checking for speech difficulty, facial symmetry, ability to show one's teeth, determine smells, shrug shoulders, swallow, etc |
|
|
subclavian steal syndrome
|
occur if subclavian artery is obstructed, particularly if internal mammary is then used for bypass grafting in coronary artery bypass pt.may not be apparent till after bypass
s/s: dizziness, syncope & vertigo, bp difference of >20 mmHg between arms |
|
|
SA node
|
located at junction of R atrium & superior vena cava. considered to be main pacer of heart rate
|
|
|
av node (atrioventricular
|
located in interventricular septum & receives impulse & transmits to bundle of his
|
|
|
heart block
|
conduction system of heart fails to conduct impulses normally. can occur from structural changes or toxic effects of drugs
assessed through ECG |
|
|
first–degree av block
|
when sa node continues to function normally but transmission of impulse fails causing heart to beat irregularly
pts are usually asymptomatic & all impulses eventually reach ventricles |
|
|
second–degree heart block
|
impulses reach ventricles but others don't
|
|
|
third–degree heart block
|
complete heart block
none of sinus impulses reach ventricle causing erratic heart rates where sinus node & av nodes are beating independently results: hypotension, seizures, cerebral ischemia or cardiac arrest |
|
|
normal ECG
|
//fce-study.netdna-ssl.com/2/images/upload-flashcards/54/87/87/11548787_m.jpeg
|
|
|
v tach
|
absence of p wave. usually exceeds 140–180bpm. lethal arrhythmia that leads to v fib.
tx: o2, amiodarone, procainamide, or mag sulfate to slow rate & stabilize rhythm |
|
|
v fib
|
primary mechanism associated w/ sudden cardiac arrest
hypotension or lack of BP & heat sounds tx: d fib. o2 & antidysrhythmic meds |
|
|
v fib
|
primary mechanism associated w/ sudden cardiac arrest
hypotension or lack of BP & heart sounds tx: d fib. o2 & antidysrhythmic meds |
|
|
normal sinus rhythm |
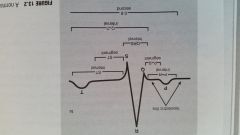
|
|
|
pulmonary embolism |
positive d-dimer & ventilation/perfusion (v/q) indicate pulmonary embolus |
|
|
valvular heart disease (most common cause) |
rheumatic heart disease |
|
|
marfan's syndrome r/t cardio problems |
pts w/ marfan's syndrome have life threatening cardio problems (mitral valve prolapse, progressive dilation of aortic valve ring & weakened arterial walls. don't usually live past 40 |