Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
56 Cards in this Set
- Front
- Back
|
What are the most abundant WBC's in the blood?
|
Segmented Neutrophils = 50-70%
|
|
|
WBC that usually make up 2-6% of total WBC count but during acute inflammation their number can elevate and cause a left shift
|
Band neutrophils
|
|
|
Decrease in the neutrophil count = ?
|
Neutropenia
|
|
|
What is the Absolute count of Neutrophils below in Neutropenia?
|
< 1800 / microliter
|
|
|
What would be the treatment for Neutropenia?
|
G-CSF = stimulates the BM to produce Neutrophils
|
|
|
List 7 causes of Neutropenia due to decreased production
|
1. Radiation = physician-induced; BM transplant patients
2. Drugs --> Daunorubicin, Chloramphenicol (specific for only causing Neutropenia) 3. Viruses = CMV and HIV 4. Alcohol 5. Megaloblastic Anemia = Folate/B12 deficiency cause Pancytopenia 6. Hereditary disorders 7. Myelodysplastic syndrome |
|
|
List 3 causes of Neutropenia due to increased destruction
|
1. Overwhelming infection = severe sepsis causes bacteria to be phagocytosed, causing neutrophils to die quickly
2. Hypersplenism = spleen has increased size and function in which it sequesters and destroys hematopoietic cells 3. Autoimmune = SLE and RA cause autoantibody production directed at Neutrophil antigens |
|
|
What is the definition of Neutrophilia?
|
Neutrophil count > 7000 / uL
|
|
|
List 6 causes of Neutrophilia
|
1. Bacterial infection
2. Tissue necrosis 3. Collagen vascular disease = SLE and RA = cause acute inflammation and stimulate BM production 4. Pregnancy = induces mild neutrophilia 5. Neoplasia = Paraneoplastic syndrome that secretes G-CSF 6. Drugs = Prednisone, Lithium, & Epinephrine cause de-margination of Neutrophils which releases them from vessel walls into circulation |
|
|
Normal Neutrophils
- 2-5 lobes with Secondary granules |
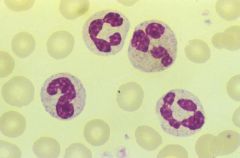
What is shown here?
|
|
|
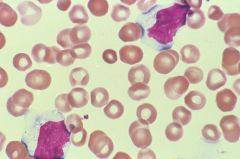
Toxic Granulation of Neutrophils
-Primary granules = play role in host defense = Respiratory burst -Cytokines that stimulate acute inflammation stimulate Neutrophils to make Primary Granules |
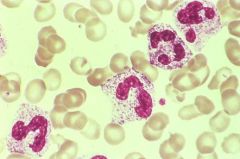
What is shown here? What is the cause?
|
|
|
Dohle Bodies = one or two light blue inclusion within the cytoplasm of Neutrophils
- aggregates of dilated RER - occur in acute inflammatory conditions |
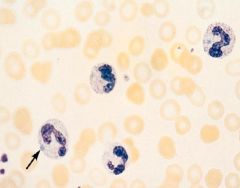
What is shown at the arrow?
|
|
|
What do Toxic Granulation and Dohle Bodies allow you to differentiate?
|
Their presence tells you that there is inflammation going on (Reactive, non-neoplastic neutrophilia), which rules out Malignant Neutrophilia
|
|
|
What is the definition of Lymphocytosis?
|
Lymphocyte count > 4000 / uL
|
|
|
What are the causes of Lymphocytosis? (2)
|
1. Viral infections
- Infectious Mononucleosis - Cytomegalovirus - Herpes Simplex Virus 2. Allergic Drug reactions |
|
|
Normal Lymphocyte
- nucleus is 1.5 times the size of RBC; cytoplasm is minimal |
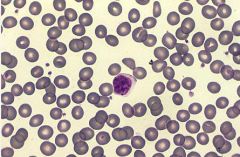
What is the cell shown in the middle?
|
|
|
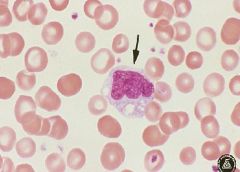
Reactive Lymphocytes
-nucleus is large and elongated -cytoplasm is abundant and basophilic where it touches RBC's = "ballerina skirt phenomenon" |
What is shown here?
|
|
|
What is the definition of Monocytosis?
|
Monocyte count > 800 / uL
|
|
|
What are the causes of Monocytosis?
|
1. Tuberculosis (chronic disease)
2. Bacterial Endocarditis 3. Collagen Vascular Disease = SLE and RA 4. Inflammatory Bowel Disease = Crohn's or Ulcerative colitis 5. Malignancy **response to Chronic inflammation & Malignancy |
|
|
Monocyte
-irregular, folded nucleus -highly vacuolated -has some granules |
Cell type seen here?
|
|
|
What is the definition of Eosinophilia?
|
Eosinophilia count > 500 / uL
|
|
|
What are the causes of Eosinophilia?
|
PAANIC
1. Parasitic infection 2. Allergic rxn (Type 1) 3. Adrenal insufficiency = Glucocorticoids have a suppressor effect on Eosinophils = take them away, Eosinophilia 4. Neoplastic disease = paraneoplastic that secretes IL-5 5. Idiopathic 6. Collagen vascular disease |
|
|
What is Idiopathic Hypereosinophilia Syndrome?
|
Eosinophil count > 1500 / uL X 6 months
|
|
|
What is the pathology of Idiopathic Hypereosinophilic Syndrome?
|
Endomyocardial fibrosis --> restrictive heart failure
|
|
|
What is the prognosis of Idiopathic Hypereosinophilic Syndrome
|
-10% survival at 3 years without therapy
-70% survival at 5 years with Corticosteroids **Prednisone/Corticosteroids sequester Eosinophils in Lymph Nodes |
|
|
Eosinophil
-pinkish granules containing Major Basic Protein, Histaminase, Arylsulfatase |
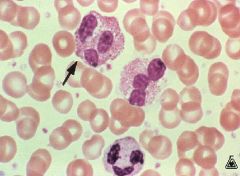
What is the arrow pointing at?
|
|
|
Define Basophilia
|
Basophil count > 200 / uL
|
|
|
What are the 4 causes of Basophilia?
|
1. Allergy
2. Collagen vascular disease 3. Inflammatory Bowel Disease 4. Severe Hypothyroidism **involved in mediating allergic rxns |
|
|
Basophil
-granules contain Heparin and Histamine Chronic Myelogenous Leukemia |
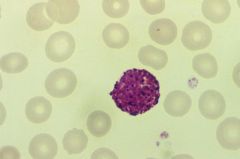
What cell is seen here?
It's -philia is seen with what cancer? |
|
|
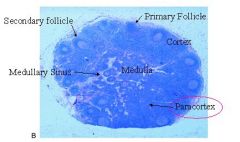
Follicles = B-cell rich zones
-Primary follicles = unstimulated B cells -Secondary follicles = stimulated B cells Paracortex = T cell rich zone Medulla = contains both B and T cells; filled with sinuses where lymph percolates through |
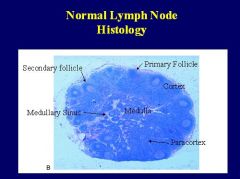
Describe each label
|
|
|
Explain Acute Lymphadenitis
|
when Pyogenic microbes cause prominent Follicular Hyperplasia and infiltration of the lymph nodes sinuses and stroma by Neutrophils
|
|
|
Give 2 examples of Acute Lymphadenitis
|
1. Bacterial Tonsillitis = cervial lymphadenopathy b/c bacteria are being drained into the nodes and the neutrophils respond
2. Acute appendicitis = mesenteric lymph nodes will be enlarged |
|
|
List the 3 types of Chronic Lymphadenitis
|
1. Follicular Hyperplasia
2. Paracortical Lymphoid Hyperplasia 3. Sinus histiocytosis |
|
|
List 4 causes of Acute Lymphadenitis and the lymph nodes they affect
|
1. Tooth abscess = cervical
2. Bacterial pharyngitis = cervical 3. Appendicitis = Mesenteric 4. Gonorrhea = Inguinal |
|
|
What is the pathology of Acute Lymphadenitis?
|

1. Neutrophil infiltrate in Sinuses and Paracortex
2. Suppurative necrosis |
|
|
What are the 3 causes of Follicular Hyperplasia?
|
1. Rheumatoid arthritis
2. HIV infection 3. Toxoplasmosis **typically in response to bacterial infections |
|
|
What is the pathology of Follicular Hyperplasia?
|
1. increased Secondary Follicles = stimulated B cells
2. High mitotic activity 3. Tingible body macrophages = phagocytosed apoptotic cells |
|
|
Follicular Hyperplasia -> Secondary Follicle
Mitotic figure Tingible body macrophage |
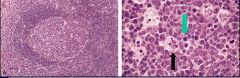
What is shown on the left?
Green Arrow? Black arrow? |
|
|
What are 3 causes of Paracortical Lymphoid Hyperplasia?
|
1. Infectious Mononucleosis = T cell response to infected B cells with EBV
2. Phenytoin = Dilantin 3. Vaccination |
|
|
What is the pathology of Paracortical Lymphoid Hyperplasia?
|
1. Increased T cell immunoblasts = activated T cells
2. Decreased Follicles |
|
|
What are the causes of Sinus Histiocytosis?
|
1. Lymph nodes draining cancer
-breast cancer = axillary LN -macrophage are responding to the tumor antigens 2. Idiopathic |
|
|
What is the pathology of Sinus Histiocytosis?
|
1. Increased Histiocytes in sinuses
2. Preserved follicles |
|
|
In the Spleen, what comprises the Red Pulp?
|
RBC's and Histiocytes (macrophages)
|
|
|
In the Spleen, where are the B and T cells?
|
B cells = Follicles
T cells = Periarteriolar sheath |
|
|
List the causes of Splenomegaly
|
1. Congestion = Portal HTN = Red pulp hyperplasia = increased RBC's and Histiocytes
2. Primary Neoplasms = Lymphangioma = enlarge the spleen itself 3. Secondary Neoplasms = Lymphoma/Leukemia = White Pulp Hyperplasia 4. Collagen Vascular Diseases = SLE and RA = White Pulp Hyperplasia 5. Storage diseases = Mucopolysaccharidoses & Gauchers = Red pulp hyperplasia b/c of Histiocytes 6. Misc. = Cysts, Amyloidosis |
|
|
List the causes of Splenic Infarction
|
1. Thromboembolism = from heart in post-MI patient
2. Subacute bacterial endocarditis = infected valve = thrombus 3. Sickle Cell Anemia = sickle cells occlude small vessels = Autoinfarction 4. Neoplasms = grow into vessel and occlude them |
|
|
What infections are those with Sickle Cell Disease at an increased risk for? Why?
|
Encapsulated microbes = S. pneumo and H. Influenza
Autosplenectomy due to sickle cells occluding small vessels |
|
|
What is the clinical significance fo Splenic infarction?
|
Hyposplenism making patients more susceptible to encapsulated bacterial infections
|
|
|
Splenic Infarction
-contains several infarcts -splenic infarcts are well circumscribed |

What is this picture showing?
|
|
|
What are the causes of Splenic Rupture?
|
1. Trauma
2. Infections = EBV, malaria, typhoid fever 3. Neoplasm |
|
|
What is the significance of Splenic Rupture?
|
Hypovolemic shock
-presents without anemia (takes 24 hours to develop) |
|
|
Congenital anomaly of the spleen that is present in 20-30% of people
|
Accessory spleen
|
|
|
What are the most common locations of Accessory Spleen?
|
1. Gastrosplenic ligament
2. Pancreas tail 3. Omentum 4. Mesentery |
|
|
What is the clinical significance of Accessory Spleen?
|
Some conditions treated by Splenectomy may not respond due to Accessory Spleen
-Hereditary Spherocytosis -Autoimmune Cytopenias |
|
|
What are the malignant Splenic neoplasms?
|
Hematopoietic
- Chronic Lymphocytic Leukemia -Chronic Myelogenous Leukemia -Acute Lymphoblastic Leukemia |
|
|
What are the benign Splenic Neoplasms?
|
1. Lymphangioma
2. Hemangioma 3. Fibroma 4. Osteoma 5. Chondroma *1&2 are Blood Vessel tumors |