![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
199 Cards in this Set
- Front
- Back
|
Describe the embryologic derivations of the Ethmoturbinals (appear in 8th week gestation) |
A: 1st ethmoturbinal, Ascending portion – Agger nasi A: 1st ethmoturbinal, Descending portion – Uncinate process A: 2nd ethmoturbinal – Bulla ethmoidalis A: 3rd ethmoturbinal – Middle turbinate A: 4th ethmoturbinal – Superior turbinate A: 5-6th ET: Usually fuse and degenerate, but occasionally can form a Supreme turbinate 3: Maxilloturbinal – Arise inferiorly, eventually becomes theInferior turbinate |
|
|
Development of the Maxillary sinus |
A: Begins at the 10th week of gestation, along with the hiatus semilunaris A: Present at birth, conspicuous growth by 3 years, second sinus to fully develop A: Inferior expansion starts with permanent dentition (7-8 years, overlies the 2nd bicuspid to 2nd molar) A: Reaches adult size by midadolescence; volume up to 15 cc 3: Remember “10 = 3 + 7” |
|
|
Development of the Ethmoids sinus |
A: Begins at the 14th week of gestation A: Present at birth, first sinus to fully develop A: Pneumatization begins significantly at 3-7 years, reaches adult form by 12-14 years, with ~14 cells (2-3 cc) 3: Remember “14” |
|
|
Development of the Sphenoid sinus |
A: Begins during the 3rd month A: Later becomes the Ossiculum of Bertini; third sinus to fully develop A: Does not pneumatize and become clinically significant until 4-5 years A: Growth complete by midadolescence, variable pneumatization 3: Remember “3-4-5” |
|
|
Development of the Frontal sinus |
A: Last sinus to fully develop A: Not present at birth, begins growth in the 3rd-5th year, and continues into adolescence A: Pneumatization highly variable; volume up to 7 cc; 5-10% are atretic 3: Remember “3-5 years” |
|
|
Name the Plain Film projections useful for each Sinus |
A: Frontal – Lateral and Caldwell A: Ethmoid – Lateral and Caldwell A: Maxillary – Waters A: Sphenoid – Lateral and Submentovertex |
|
|
Describe the Mucociliary flow in the frontal sinus |
A: Medial to the ostium – Flows superiorly then laterally along the roof A: Lateral to the ostium – Flow medially and inferiorly toward the ostium |
|
|
Six bones of the Nasal Septum |
A: Perpendicular plate of Ethmoid A: Vomer A: Maxilla – Anterior nasal spine and Maxillary crest A: Palatine bone – Maxillary crest A: Sphenoid A: Nasal bones (included in Schuenke) |
|
|
Define Agger nasi cell |
A: Product of 1st ethmoturbinal, found superior, lateral & anterior to attachment of the middle turbinate; can also refer to the anteriormost ethmoid cell, anterior to the frontal recess A: Boundaries are frontal process of maxilla anteriorly, nasal bones anterolaterally, frontal recess superiorly, lacrimal bone inferolaterally, uncinate process inferomedially |
|
|
Define Suprabullar recess |
A: Air cell space left between the ethmoid bulla and the fovea ethmoidalis when the bulla does not extend up to the fovea |
|
|
Define Sinus Lateralis/Retrobullar Recess |
A: Variable air space found posterior and superior to the ethmoid bulla, in the anterior ethmoid region A: Boundaries are the ethmoid roof superiorly, lamina papyracea laterally, vertical portion of the basal lamella posteriorly |
|
|
Define Terminal Sinus/Recessus Terminalis |
A: Superior boundary of the ethmoid infundibulum when the uncinate process terminates in the lamina papyracea (80%); the frontal recess drains medial to the uncinate process in this instance |
|
|
Define Haller cell |
A: An infraorbital ethmoid cell, pneumatizes into the maxilla |
|
|
Define Onodi cell |
A: A sphenoethmoidal cell, a posterior ethmoid air cell pneumatizing into the sphenoid |
|
|
Keros classification of lateral cribriform plate lamella length/olfactory fossa depth |
A: Type 1 – Cribriform plate 1-3 mm below fovea A: Type 2 – Cribriform plate 4-7 mm below fovea A: Type 3 – Cribriform plate 8-16 mm below fovea (greatest risk of intraoperative CSF leak) A: Type 4 – Asymmetrical |
|
|
Describe the Kuhn classification of frontal cells |
A: Definition – An anterior ethmoid cell above the agger nasi that can obstruct the frontal recess or the frontal sinus A: Type I – Single frontal recess cell above agger nasi but below the floor of the frontal sinus A: Type II – Multiple cells (tier) in frontal recess above agger nasi but below floor of frontal sinus A: Type III – Single cell pneumatizing cephalad into frontal sinus A: Type IV – Single isolated cell completely within the frontal sinus, not located within the frontal recess |
|
|
What are the six cell types found in olfactory epithelium? |
A: Ciliated Bipolar receptor cells – Increase surface area, lack dynein arms and do not beat A: Sustentacular cells – Microvilli, insulate bipolar cells, deactivate odorants, protect epithelium from foreign agents, regulate mucus composition A: Microvillar cells – 1/10th as frequent as bipolar cells, may have a receptor function (unknown currently) A: Lining epithelium of Bowman’s glands & ducts A: Globose (light) Basal cells A: Horizontal (dark) Basal cells3: “Be My Big Sister HoBo!” |
|
|
Olfactory neuroepithelium histology |
A: Pseudostratified columnar epithelium |
|
|
Describe the histology of the Olfactory Bulb |
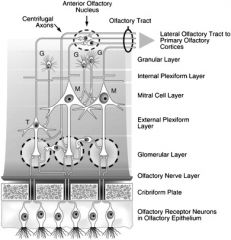
A: Two layers – Internal and External Plexiform layers A: Synapses form aggregates called Glomeruli A: Three cell types – Mitral, Tufted, and Granular cells A: Synapses are mostly GABAergic and Dopaminergic 3: “My Tough Granny lives in the olfactory bulb, Dopi Grama!” |
|
|
List the central olfactory connections |
A: Olfactory tubercle A: Prepyriform cortex A: Lateral Entorhinal cortex A: Periamygdaloid cortex A: Amygdaloid nucleus A: Nucleus of the Terminal Stria A: Dentate and Semilunate gyri |
|
|
Describe the olfactory transduction mechanism |
A: Odorants are solubilized in mucus, or hydrophobic odorants by Odorant Binding Protein (OBP) A: G-Protein coupled receptors (~1000, 1% of expressed genes) A: Second messenger = cAMP |
|
|
Three differences between Olfactory and Respiratory epithelium |
A: Olfactory epithelium is thicker (60-70 nm) than respiratory epithelium (20-30 nm) A: Olfactory epithelium has cilia that lack dynein arms A: At physiologic flow rates olfactory epithelium gets ~15% of nasal airflow, 50% flows through middle & inferior meati |
|
|
Describe Foster Kennedy syndrome |
A: Ipsilateral anosmia/hyposmia A: Ipsilateral optic atrophy A: Central/contralateral papilledema 3: Due to tumors of the olfactory groove or sphenoid ridge (e.g. meningiomas) |
|
|
Define Kallmann’s syndrome |
A: Transmitted X-linked (Cummings) A: Endocrine anomalies – Diabetes; Hypogonadotropic hypogonadism (deficiency of hypothalamic GnRH secretion) A: Genito-urinary anomalies – Micropenis, Cryptorchidism,Unilateral renal agenesis A: Anosmia - Agenesis of the olfactory bulbs A: Deafness A: Midline facial deformities |
|
|
Define Anosmia |
A: Loss of ability to smell A: Can be specific, partial, or total depending on whether certain odors or no odor can be detected, uni or bilateral |
|
|
Define Hyposmia/Microsmia and Hyperosmia |
A: Decreased ability to smell and hypersensitivity to odors, respectively |
|
|
Define Dysosmia |
A: Distorted or perverted smell perception 3: Causes (Bailey’s): degenerative-regenerative process (post trauma, URTI), psychosis, aura-like hallucinations from central dysfunction, foul odors (purulence in CRS) |
|
|
Define Parosmia/Cacosmia |
A: Change in the quality of the olfactory cue, particularly of putrefactive odor |
|
|
Define Phantosmia |
A: Odor sensation in the absence of an olfactory stimulus (olfactory hallucination) |
|
|
Define Olfactory Agnosia |
A: Inability to recognize an odor |
|
|
Two surgical treatment options for Parosmia/Phantosmia |
A: Olfactory bulbectomy A: Endoscopic removal of olfactory neuroepithelium |
|
|
Six Methods of olfactory testing |
A: Subjective odorant testing/Detection threshold – Sniffing sticks, 1 minute smell test A: Standardized psychophysical tests – OCM = Odorant Confusion Matrix; UPSIT = University of Pennsylvania Smell Identification Test, highly reliable A: Electrophysiologic tests – OERP = Odor event-related potentials, experimental, identifies brain EEG activity after odor presentation; far field potentials, cannot localize site of lesion; “EOG” = Electoolfactogram, electrode placed on olfactory epithelium identifies summated generator potentials of olfactory receptor neurons; no local anesthesia so uncomfortable; Flase positives in Kallman’s and schizophrenia |
|
|
Five factors affecting olfactory testing (MASSAM) |
A: Mental State A: Age A: Satiety A: Sex A: Adaptation/Cross-adaptation A: Masking |
|
|
Classification of Hyposmia/Anosmia (3) |
A: Access of odorant changed – Conductive A: Damage to olfactory nerve & receptors – Sensory A: Damage to central olfactory pathways – Neural |
|
|
Ddx of Olfactory dysfunction |
A: Congenital – Kallman’s, Familial anosmia (AD, premature baldness, vascular headaches) A: Obstructive nasal disease (23%) – Polyps, edema, tumors, nasal deformity A: Idiopathic (21%) A: Postinfectious (19%) – Viral injury to olfactory neurons A: Head Trauma (15%) – Shearing of filaments, olfactory bulb contusion, frontal lobe injury; CN I is the most commonly damaged CN, followed by VIII, X, and VII ?VI A: Neurologic – Parkinson’s, Alzheimer’s, Multiple SclerosisA: Psychogenic (schizophrenia) A: Toxins/medications (3%) – Smoking, Formalin A: Aging A: Neoplastic – Foster-Kennedy syndrome A: Other |
|
|
Three reasons for Age-related olfactory changes |
A: Cumulative damage to the olfactory epithelium from viral and other insults A: Ossification/closure of the foramina of the cribriform plate A: Pathologies such as Alzheimer’s and Parkinson’s |
|
|
Name the 3 main functions, and 6 subfunctions, of the nasal airway |
A: Respiration – Warming (37 C), Humidification (85%), and Nasal airflow (which can be altered through airway resistence by congestion & decongestion of the mucosa) A: Protection – Filtration, Mucocilliary clearance, and Immune protection A: Olfaction – To sense the environment through the specialized & general sensory nerves (olfactory & trigeminal) |
|
|
Name four mechanisms of Innate immunity in the nose |
A: Barrier – Epithelial tight junctions A: Enzymes/Peptide antibiotics – Locally secreted in mucus;Lactoferrin, Lysozyme, IgA A: Phagocytes – Neutrophils and macrophages A: PAMP Receptors – Expressed on epithelium and phagocytes, detect Pathogen Associated Molecular Patterns, cause secretion of immune mediators |
|
|
Describe the Sympathetics Autonomic supply to the nasal mucosa |
A: Vasoconstrictor tone A: Preganglionics from sympathetic chain synapse in the Superior Cervical Ganglion A: Postganglionics travel with ICA, split off as deep petrosal nerve and joins with greater superficial petrosal nerve to form the vidian nerve A: Pass through the sphenopalatine ganglion without synapsing, into the sphenopalatine nerve, through the foramen and into the nasal cavity |
|
|
Describe the Parasympathetics Autonomic supply to the nasal mucosa |
A: Vasodilation of capacitance & resistance vessels, also mediate nasal secretion A: Preganglionics arise in Superior Salivatory Nucleus, travel in nervus intermedius and branches off a t the geniculate ganglion as the greater superficial petrosal nerve and becomes the vidian nerve, synapses at the Pterygopalatine Ganglion A: Postganglionics distributed with sympathetics throughMaxillary trigeminal branches to the nose |
|
|
Internal Nasal valve & Cross sectional area |
A: Extends from caudal end of upper lateral cartilages to anterior end of inferior turbinates A: Influenced by nasal septum, upper lateral cartilage, pyriform aperture, anterior inferior turbinate A: Cross sectional area 0.73 cm2; 10-15 degrees caucasians 3: Nasal valve competency tested with the Cottle maneuver |
|
|
Discuss Rhinomanometry |
A: Measures the resistance to airflow in the nose (transnasal pressure and air flow), but cannot identify specific sites of obstruction; 3 types A: Anterior Rhinomanometry – Occlusion of one nostril with an inflatable cuffed pressure sensor at the nasal orifice measures nasopharyngeal pressure; nonphysiologic, as all airflow happens through the other unoccluded nostril A: Posterior Rhinomanometry – Placement of pressure catheter in mouth which can accurately measure nasopharyngeal pressure; more physiologic measure of nasal resistance through both nostrils simultaneously A: Postnasal (Pernasal) Rhinomanometry – Tube is placed in the posterior nose through one of the nostrils 3: Total nasal resistance >0.3 Pa/cm2 usually is symptomatic3: >35% reduction in resistance after decongestion infers mucosal disease; <35% reduction in resistance infers a structural cause |
|
|
Discuss Acoustic Rhinometry |
A: Analyzes 10 msec sound pulses reflected from the airway, can accurately identify the minimal cross-sectional area (MCA), the location of the MCA, and the cross-sectional area at various distances from the nostrils A: I-Notch – Isthmus of the internal nasal valve, within 2 cm of nostril, usually narrowest = 0.73 cm2 A: C-Notch – anterior inferior Concha, ~3.3 cm from nostril A: Does not rely on nasal airflow, but cannot measure the effects of narrow regions on airflow dynamics or resistance 3: Three areas of nasal resistance – Vestibule (1/3), Valve (1/2-2/3), Turbinated cavity is the rest |
|
|
Five factors controlling nasal airflow |
A: Vasomotor control/Nasal cycle A: Exercise – Epinephrine A: Sex Hormones – Puberty, Menstruation, Pregnancy A: Nitric Oxide – Affects Nasal AND Pulmonary blood flow, Ciliary beat frequency A: Head & body Position |
|
|
Ten complications of Septoplasty |
A: Failure/persistent obstruction A: CSF leak A: Synechia A: Anosmia A: Hemorrage A: Septal Hematoma/Abscess A: Perforation A: Saddle nose deformity A: Toxic-shock syndrome A: Aspiration |
|
|
Surgical options for Nasal Valve Obstruction |
A: Spreader grafts A: Baten grafts A: Nasal-orbital suspension A: Valvuloplasty with composite graft A: Columellar strut graft (Bailey p. 331) A: Address other components of the valve – Septum, Turbinate 3: Others: Flaring sutures, overlay grafts, lateral suture suspension |
|
|
Five foramina of maxilla |
A: Infraorbital A: Superior alveolar canal(s) A: Incisive canal A: Maxillary ostium A: Accessory maxillary ostium |
|
|
Four broad categories of Rhinitis |
A: Allergic A: Infectious A: Structural A: Other 3: “All Other Infra-Structures” |
|
|
Name the 13 etiologies of “Other” rhinitis (non-Structural, non-Inflammatory, non-Allergic causes) |
A: Compensatory hypertrophic rhinitis A: Non-Airflow rhinitis – Postlaryngectomy, choanal atresia, adenoid hyperplasia A: Temperature mediated A: Environmental/Irritative rhinitisA: Gustatory rhinitis A: Endstage vascular atony of chronic allergic or inflammatory rhinitis A: Hormonal – OCP, Puberty, Pregnancy (estrogen effect in 2nd trimester), Menopause, Hypothyroidism, Acromegaly A: Drugs – Antihypertensives, Topicals (cocaine & nasal spray abuse), NSAIDs, ASA, Psychotropics A: Non-Allergic Rhinitis with Eosinophilia Syndrome (NARES), or Basophilia – Similar to perennial allergic rhinitis, lacks the IgE mediated immunopathologic events, AND >20% eosinophils on nasal smear A: Recumbency rhinitis A: Paradoxic nasal obstruction and nasal cycle A: Emotional causes A: Idiopathic3: “Compensating for Non Temperate Environments by Gustating Endstage Hormonal Drugs through my Nares Renders me a Paradoxically Emotional Idiot!” |
|
|
Etiology of vasomotor Rhinitis during Pregnancy |
A: 20% of pregnancies, usually starts in 2nd trimesters A: Increased Estrogen levels inhibits Acetylcholinesterase activity, leads to increased ACh in parasympathetic ganglia, causes swelling & edema of nasal mucosa A: Treatment – Conservative, saline spray, possible use ofBudesonide (Rhinocort) spray, Consult obstetrician; no use of decongestants |
|
|
Define Atrophic Rhinitis |
A: Classified as a transformation of the respiratory pseudostratified columnar epithelium to a keritanized squamous epithelium that sloughs off |
|
|
Ten Granulomatous diseases of the Sinonasal tract |
A: Systemic (3) and Infectious (8) A: Sporotrichosis A: Blastomycosis (dermatiditis) A: Coccidiomycosis (immitis) A: Rhinoscleroma A: Rhinosporidiosis (seeberi) A: TB A: Leprosy A: Syphilis A: Sarcoidosis A: Wegener’s A: Histiocytosis X 3: “Sporo Blasto Cocci Rhino-Rhino, TB Lepy Syphi, Sarcoid,Wegener’s & Histio” |
|
|
How to detect Eosinophilia on nasal smears |
A: Acquire sample of nasal mucus (wax paper or swab), smear on slide A: Stain with Hansel stain (Eosin & Methylene Blue) A: Positive criteria = >20% eosinophil content, or if Eosinophils,Mast cells & Goblet cells (EMG) are present |
|
|
Describe the Gell and Coombs Type Hypersensitivity Reactions (ACID) |
A: Type I – Immediate IgE (Allergic rhinitis, anaphylaxis, asthma) A: Type II – Cytotoxic IgG or IgM antibody mediated A: Type III – Immune complex mediated, Ag-Ab-Complement (serum sickness, Arthus reaction) A: Type IV – Delayed type hypersensitivity, T-cell mediated |
|
|
Discuss the Methods of testing for Atopy |
A: Skin tests – Detect presence of IgE-mediated allergy; takes little time to do (~1 hr), but uncomfortable, risk of anaphylaxis; generally classified as Epicutaneous (scratch tests and prick puncture tests) or Intracutaneous (single-dilution and multiple dilution intradermal tests); Negative control is GLYCEROL/saline, and Positive control is Histamine Scratch tests – Neither sensitive nor reproducible Prick tests – Not sensitive for low levels of atopy Intradermal testing – More sensitive & reproducible Serial Dilution Endpoint testing/ Skin Endpoint Titration – Intradermal test, determines more specific levels of atopy, used to determine immunotherapy concentrations A: Direct measurement of Allergen-specific IgE in serum; serumincubated with known Antigens on a matrix; excess serum washed off, and residual complexes incubated with anti-IgE and a marker; More specific but less sensitive cf. skin tests, takes longer to do (days) RadioAllergoSorbent Test (RAST) – Radioactive marker Enzyme-Linked ImmunoAssay (ELISA) – Fluorescent marker |
|
|
Describe the ARIA Classification of Allergic Rhinitis
|
A: Intermittent – <4 days/week OR <4 weeks/year
A: Persistent – >4 days/week AND >4 weeks/year A: Mild – Normal sleep, no impairment in ADLs/Work/School, and no troublesome Symptoms A: Moderate-Severe – Any of Abnormal sleep, impairment inADLs/Work/School, or troublesome Symptoms |
|
|
Three approaches to Treatment of Allergy |
A: Avoidance – Mattress/pillow covers are best measure for mites; removing carpets also useful A: Pharmacotherapy –Nasal Steroid (1st line therapy, spray or inferior turbinate injections), Antihistamines, LeukotrieneReceptor Antagonists, Cromolyn (topical mast cell stabilizer, decreases influx of calcium), Decongestants (topical or systemic),Systemic steroids (short course) A: Immunotherapy |
|
|
List 3 First generation H1 Antihistamines |
A: Diphenhydramine/Benadryl A: Hydroxizine/Atarax A: Chlorpheneramine/Chlortripolon 3: Sedating; “Diphen-Hydroxy-Chlorphen” |
|
|
List 4 Second generation H1 Antihistamines |
A: Loratidine/Claritin A: Desloratidine/Aerius (3rd gen?) A: Certirizine/Reactine A: Fexofenadine/Allegra (3rd gen?) 3: “Lora-Deslora-Certri-Fexo” |
|
|
Six effects of corticosteroids in Allergic Rhinosinusitis |
A: Decreased Arachidonic Acid metabolism (PG/LT/TX) A: Decreased secretion of Mediators of inflammatory cellProliferation A: Decreased Influx of Eosinophils, Basophils & T-lymphocytes into the nasal epithelium A: Decreased Capillary Permeability and promotesVasoconstriction A: Decreased glandular response to ACTH,Decreases Mucus production A: Stabilize Lysosomal membranes A: decreased Migratory inhibitory factor |
|
|
List 4 Intranasal corticosteroids |
A: Mometasome/Nasonex A: Fluticasone/Flonase AND Avamys A: Triamcinolone/Nasacort A: Budesonide/Rhinocort AND Pulmicort A: Omnaris/ciclesonide |
|
|
Ten Complications and Contraindications of Steroid sprays |
A: Hypersensitivity A: Atrophic rhinitis A: Epistaxis A: Septal perforation A: Glaucoma A: Cataracts A: Ocular herpes A: Systemic fungal infections A: TB A: Adrenal suppression |
|
|
Describe the Mygind, Ragan & Moffett positionsNasal drop bioavailablity is enhanced by head position |

A: Improves efficacy of nasal steroid application (controversial) A: Mygind’s position (a) - Administration of nasal drops in a head back supine position, followed by a series of head turns A: Ragan position (b)- Involves the patient lying on one side with the head touching the bed or floor surface, while the drops are instilled in the inferior nostril A: Moffett position (Mecca) (c)- The patient kneels and leans forward with forehead to the ground and administers drops in nostrils |
|
|
Ten causes of Septal Perforation |
A: Trauma A: Surgery A: Cocaine abuse A: Septal hematoma/abscess A: HHT A: Wegener’s A: Lymphoma A: Syphilis A: TB A: Chrome workers A: Bilateral AgNO3 cauterization |
|
|
Ten indications for Immunotherapy in allergic rhinitis include symptoms of allergy after natural exposure to aeroallergens and evidence of clinically relevant specific IgE, AND… |
A: Poor response to Avoidance measures A: Allergens not easily avoided A: Poor response to Pharmacotherapy A: Unacceptable Adverse Effects of medications A: Severe symptomatology, persisting for >1 season A: Coexisting allergic rhinitis and asthma A: Possible Prevention of asthma in children A: Patient Wishes to reduce/avoid long-term pharmacotherapy and cost A: Motivated patients willing to undergo a program that may last up to 5 years |
|
|
Administration & Mechanism of Action of Immunotherapy |
A: Parenteral administration of antigens identified on appropriate in vivo or in vitro tests A: Stimulate formation of allergen-specific IgG4 blocking antibodies which will compete with IgE for binding sites on Mast cells or Basophils A: Decreases IgE and reduces the seasonal rise of IgE A: Changes CD4+ cells from Th2 to Th1 phenotype A: Typically twice a week until a response is noted, then q1 week x 1 year, q2 weeks x 2 years, q3 weekly x 3 years |
|
|
Describe the Skin Endpoint Titration technique and results |
A: 0.01 mL injected – Wheel response of 5 mm normal with control A: Induration (not erythema) is measured, serial increase by 2 mm is the endpoint titration. Recall that need a confirmatory wheel of greater than 2 mm to confirm previous wheel (which also grew by at least 2 mm) |
|
|
Three abnormal wheeling patterns on Skin Endpoint Titration |
A: FlashDay 1 – 5-5-5-13-18-21Day 2 – 5-5-5-5-7-9-11 A: Plateau – 7-7-9-9-11-11Confirmatory here is fifth injection with fourth injection the SET A: Hourglass – 9-7-5-5-7-9-11 |
|
|
Six factors influencing Skin Endpoint Titration |
A: Age A: Antihistamines A: Skin reactivity (eg to trauma, Dermatographia) A: Food allergens A: Increased Allergen exposure – Greater response during allergic season A: Volume injected |
|
|
Condition of positive Skin Endpoint Titration with negative control solution |
A: Dermatographia 3: Can do RAST testing for these patients (not affected by antihistamines) |
|
|
The 3 Pollen seasons for seasonal allergens |
A: Trees – Spring A: Grass – summer A: Weeds – Fall |
|
|
List the 4 types of Perennial Allergens |
A: Animal Dander A: Dust mite (#1) A: Cockroach allergens A: Mold (notes say only outdoor, not black mold?) |
|
|
Most common pollen, mold, and perennial allergens |
A: Pollen – Short Ragweed A: Mold – Alternaria A: Perennial –Dust Mite (Dermatophagoides spp) |
|
|
indications for use of in-vitro allergy testing include |
A: Impracticality of skin testing due to Skin disorder, Drug inhibition or Uncooperative patients A: Clarification of Bizarre or Borderline results from skin testing A: Prevention of systemic reactions in patients with a prior history of or suspected Anaphylactic reactions, Asthma, or when testing for Stinging hypersensitivity A: Convenience of in vitro testing 3: “Impractical Clarifications Prevent Convenience” |
|
|
Three differences between mucosa of nose and sinuses |
A: Ciliated cells more concentrated at the ostia A: Increased number of goblet cells present in the nose A: (No olfactory neuroepithelium in the sinuses) |
|
|
Seven etiologic factors for Nasal Polyps |
A: Chronic infection A: Allergy, including Fungal A: Samter’s triad A: Cystic fibrosis A: Nasal mastocytosis (increased mast cells in nasal mucosa) A: Kartegener’s syndrome A: Young’s syndrome (bronchiectasis, rhinosinusitis and reduced fertility) |
|
|
Define Samter’s triad |
A: Nasal polyposis, asthma, and ASA sensitivity A: Thought to block oxidative phosphorylation; anti-inflammatory actions due to blockage of cyclooxygenase enzyme; polyp formation influenced by stimulation of 5-lipoxygenase, which causes leukotriene overproduction |
|
|
Not including polyps, what are the 4 most common benign nasal cavity lesions in order of frequency? (OHPA!) |
A: Osteoma (most commonly in the frontal sinus) A: Hemangioma A: Papilloma A: Angiofibroma |
|
|
Discuss Osteoma |
A: Most common tumor of the paranasal sinuses A: Clinical – Males affected 3:1; R/O Gardner’s syndrome (with soft tissue tumors/cysts, and colonic polyps) because 100% risk of colorectal cancer by age 40 A: Causes – Developmental (at the junction of membranous frontal bone and endochondral ethmoid bone), but can also be Tramatic, or Infectious (osteitis) A: Histopathology – Eburnated (dense), Mature (cancellous), orMixed A: Types (FEMS) – Frontoethmoidal (95%) > Frontal (80%) >Ethmoid (25%) > Maxillary > Sphenoid A: Complications – Sinusitis (28%), Orbital, or Intracranial A: Treatment – Complete removal, only if symptomatic |
|
|
Discuss Ossifying Fibroma |
A: Can be aggressive & locally destructive A: Osteoid rimmed by osteoblasts forming lamellar bone A: Round or oval, eggshell rims, central translucency A: Treatment – Complete removal |
|
|
Discuss Schneiderian papilloma |
A: Definition – Proliferation of squamous epithelium through fingerlike projections into underlying stroma A: Ddx – Benign vs. Malignant, Epithelial vs. Non-epithelial tumors A: Diagnosis – Biopsy A: Causes – HPV 6 & 11 suspected (inhibit p53) A: Clinical – White, males 3:1, 5th-7th decade; Nasal obstruction(87%), rhinorrhea, facial pain/pressure, epistaxis, frontal headaches, epiphora; Exophytic, fleshy, sessile vs. pedunculated, bony destruction/erosion common, tendency to recur A: Complications – Recurrence, Malignant change (~10%, lateral wall > septal) A: Types – Inverting (50%, lateral wall), Fungiform (47%, septal), Cylindrical/Oncocytic (3%) A: Tests – FOB scope, CT, MRI (iso/hypo on T1, enhance with gad, hyperintense on T2, convoluted cerebriform pattern), Biopsy A: Treatment – Total surgical removal with medial maxillectomy, either via Lateral rhinotomy or Transnasal/ESS approach |
|
|
Krause staging for Schneiderian inverting papilloma |
A: T1 – Limited to nasal cavity A: T2 – Extension ethmoids and/or to medial wall of maxillary sinus A: T3 – Extension to sup/lat/inf/ant/posterior wall of maxillary sinus and/or frontal or sphenoid sinus A: T4 – Extension outside the nasal cavity and sinuses and/or malignancy |
|
|
Eleven limits of Endoscopic Resection of Sinonasal tumors |
A: Massive Dural/Intradural extension A: Massive Skull Base erosion A: Frontal sinus extension A: Nasal pyramid extensionA: Intraorbital extension A: Lacrimal tract extension A: Maxillary wall involvement (except medial)A: Nasopharyngeal extension A: Hard palate extension A: Abundant scar tissue from previous surgery A: Associated Squamous cell carcinoma 3: Contraindications to exclusive endoscopic technique in Sinonasal benign tumors (Nicolai & Castelnuovo):(1) Massive involvement of the frontal sinus and/or of a supraorbital cell(2) Intradural extension or orbital extension(3) Concomitant presence of a malignancy involving critical areas(4) Presence of abundant scar tissue from previous surgery. |
|
|
Five types of nasopharyngeal cysts |
A: Rathke’s pouch cyst – Remnant of invaginated ectoderm that forms the anterior pituitary gland, anterior to the pars intermedia; located high in nasopharynx near sphenovomeral junction; ciliated respiratory epithelium A: Tornwaldt’s cyst – Remnant of notochord, inferior to Rathke’s pouch; filled with jellylike material; ciliated respiratory epithelium (high signal intensity on both T1- and T2-weighted images) A: Dermoid cyst – Benign developmental cyst derived from ectoderm and mesoderm; stratified squamous epithelium with adnexal structures A: Intraadenoidal – From median pharyngeal recess, opens onto adenoid bed A: Extraadenoidal – Deep within pharyngobasilar fascia, remnant of the pharyngeal bursa; usual findings are a cuff of granulation tissue rostral to the pharyngeal tubercle |
|
|
Describe the 4 cell types making up the nasal epithelium |
A: Pseudostratified Ciliated Columnar epithelium – ~50 cilia per cell beating, ~12/second at physiologic temperature, moves mucus 3-25 mm/minute A: Pseudostratified Nonciliated Columnar epithelium – Possess microvilli that expand the surface area of the epithelium A: Goblet cells A: Basal cells 3: Other cell types – Stratified squamous epithelium in nasal vestibule, and olfactory epithelium found along roof of nose |
|
|
Two Mucous layers in upper resp tract, and function of each |
A: Sol layer – Thin periciliary layer which allows cilia to be mobile; produced by microvilli A: Gel layer – Thick layer of mucoglycoproteins in which cilia embed themselves; produced by goblet cells and submucosal glands, propelled by ciliated epithelium; (antibacterial and clearance of foreign particles?) |
|
|
Three stages of sphenoid sinus pneumatization |
A: Sellar (86%) A: Presellar (11%) A: Conchal (3%) 3: Pneumatization starts between 5 & 7 years of age, complete by20-25 years |
|
|
Incidental findings of sphenoid sinusitis on imaging – what should you consider? |
A: Optic complications – 25% of patients with sphenoid sinusitis have neurophthalmic dysfunction |
|
|
Five factors present in nasal secretions which fight infection |
A: IgA A: IgG A: Lysozyme A: Lactoferrin A: Interferon |
|
|
What 10 local factors influence nasal ciliary motility? |
A: Allergy A: Rhinitis medicamentosa (chronic abuse) A: Infection (viral, bacterial) A: Primary ciliary abnormalities A: Temperatures <18 C A: Humidity <50% A: Hypertonic or hypotonic solutions A: Dehydration A: Excessive acidic or basic environment (optimal ciliary function @ pH 7.0) A: Mucosal to mucosal surface contact (coapting) |
|
|
Five clinical features of Kartagener’s (immotile cilia) syndrome, abnormalities in cilia? |
A: Sinusitis A: Bronchiectasis (chronic cough) A: Situs inversus & dextrocardia A: Otitis media A: Male Infertility (immotile sperm) 3: Autosomal recessive inherited lack of Dynein arms in A-tubules (9+2 microtubule structure) |
|
|
Six possible findings in Immotile cilia |

A: Lack of Dynein arms A: Lack of central core structures A: Radial spoke defect A: Microtubule translocation A: Microtubule altered in length A: Ciliary aplasia * Left, Normal cilium, Right, the absence of outer and inner dynein arms in a patient with primary ciliary dyskinesia |
|
|
What are the associations between CRS, Polyps (NP), and Asthma? |
A: 20% of CRS have NP A: 20% of CRS have Asthma A: 40% of FESS have Asthma A: 50% of NP have Asthma (35% of which have Samter’s triad) A: 10% of NP have Samter’s triad |
|
|
Seven areas to evaluate in preoperative CT scan |
A: Frontal sinus/recess and Agger nasi A: Skull base (Keros classification) A: Anterior ethmoid artery A: Lamina papyracea/Uncinate process A: Maxillary sinuses (Haller cells) A: Vertical height of the posterior ethmoid A: Sphenoid sinus (Onodi cells, ON, ICA) |
|
|
General method of subclassifying Complications in Rhinology |
A: Vascular A: Nerve damage A: Facial swelling or ecchymosis A: Orbital A: Intracranial A: Packing related 3: “Very Nice Face or Brain Please!” |
|
|
Six risk factors for complications in FESS |
A: General anesthesia – lack of patient feedback A: Extent of disease A: Amount of Bleeding A: Left orbit for a right-handed surgeon A: Revision FESS A: Expertise of the surgeon 3: “this General Extent of Bleeding is Right for a Revision Expert” |
|
|
Major FESS complications |
A: Intracranial (7) – CSF leak, Tension pneumocephalus,Meningitis, Abscess, Hemorrhage, Encephalocele, Direct brain injury A: Orbital (5) – NLD injury, Enophthalmos, Diplopia (medial rectus injury), Hematoma, Blindness (optic nerve injury) A: Bleeding (4) – Damage to Anterior ethmoidal, Sphenopalatine, or Internal carotid arteries; any requirement of a transfusion A: Other – Anosmia, Asthma exacerbation, Toxic Shock, Death |
|
|
Minor FESS complications |
A: Intracranial – CSF leak A: Orbital – Emphysema, Fat herniation, Ecchymosis A: Bleeding – Small amount, not requiring transfusion A: Other – Hyposmia, mild Asthma exacerbation, MRSA infection, Hypesthesia of the infraorbital nerve or teeth, Synechiae, Atrophic rhinitis, Osteitis |
|
|
Seven predictors of poor FESS outcome |
A: Smoking! A: Asthma A: Polyps A: ASA sensitivity A: Fungal disease A: Extensive disease (CT) A: Previous surgery |
|
|
Seven Indications for Image Guided Surgery according to the AAO-HNS |
A: Revision surgery A: Distorted anatomy A: Extensive NP A: Disease in Frontal, Posterior Ethmoid, or Sphenoid A: Disease abutting the Skull base, Orbit, Optic nerve or carotid A: CSF rhinorrhea or skull base defect A: Benign and malignant sino-nasal neoplasms |
|
|
Define Myospherulosis |
A: Foreign body reaction to the petroleum ointment used in packing |
|
|
Define the Holman-Miller sign |
A: Anterior bowing of posterior maxillary sinus wall A: Indicates JNA invasion of pterygopalatine fossa |
|
|
Biopsy of which 4 nasal masses are at significant risk of hemorrhage? |
A: JNA A: Hemangioma A: Hemangiopericytoma A: AV malformations |
|
|
Potential complications of radiotherapy for management of JNA? |
A: Failure of treatment A: Induction of malignancy A: Failure of facial growth centers A: Cataract formation 3: Radiotherapy used in past successfully for primary therapy, recurrences, inoperable tumors |
|
|
Difference between a Mucocele and a Mucus Retention Cyst |
A: Mucocele – A chronic, cystic lesion of the paranasal sinuseslined with pseudostratified or low columnar epithelium, containing occasional goblet cells; presents radiologically with complete sinus opacification, with rounded thinning pushing margins; blocked sinus A: Mucus retention cyst – Retained mucus within a blocked goblet cell, lined by sinus mucosa rather than a true epithelium 3: These definitions do not apply to salivary pathology, where only the mucus retention cyst is the true cyst, and mucocele refers to mucus extravasation |
|
|
Ddx of small round cells on nasal biopsy (MRS SLEEPI) |
A: Melanoma A: Rhabdomyosarcoma A: Small cell neuroendocrine tumor (Carcinoid?) A: Sinonasal undifferentiated carcinoma (SNUC) A: Lymphoma A: Esthesioneuroblastoma A: Ewing’s sarcoma/PNET (Carcinoid?) A: PlasmacytomaA: Immature teratoma |
|
|
60 year old female with blocked nose, and nasopharyngeal mass. Biopsy is LCA positive and cytokeratin negative. What is this? What is ruled out? |
A: Lymphoma A: SCC (NPC) ruled out by negativity of Cytokeratin |
|
|
Four histologic and clinical differences of T-cell lymphoma and Wegener’s granulomatosis of the nose |
A: Wegener’s has diffuse nasal ulcerations; Lymphoma lesions are Focal, localized & explosive A: Wegener’s has a Small & Medium vessel Vasculitis; Lymphoma has a polymorphic lymphoid infiltrate with Angiocentric & Angioinvasive features A: Wegener’s has an inflammatory cell infiltrate; Lymphoma has am primarily lymphocytic infiltrate A: Otologic, Tracheal, Renal involvement rare in lymphoma |
|
|
Ddx of Fibroosseous nasal lesions (4) |
A: Osteoma A: Osteochondroma A: Ossifying fibroma A: Fibrous dysplasia |
|
Discuss Hemangiopericytoma * Staghorn-shaped capillary spaces lined by plump pericytes (arrows) |
A: Originates from the capillary Pericyte of Zimmermann A: Occurs wherever there are capillaries; MSK and Skin predilection A: Histologically consist of packed ovoid/spindle cells, and staghorn vessels displaying perivascular hyalinization A: Unpredictable, considered Malignant & infiltrative A: Treatment – Wide surgical excision, may require preoperativeembolization; Radiotherapy generally for palliative cases, although adjuvant XRT has been recommended for high-grade features of positive margins; Neck dissection not necessary as lymphatic spread is rare; 5-year survival rate near 70%, and distant metastases usually portend recurrence at the primary site |
|
|
Two Absolute Contraindications to IV iodinated contrast for CT |
A: Previous adverse reaction A: Severe renal insufficiency (esp. in Multiple Myeloma, DM,Nephrotoxic meds) |
|
|
Seven Relative Contraindications to IV iodinated contrast for CT |
A: Advanced age A: Asthma A: Atopy A: Beta-blockers A: Cardiac disease A: Dehydration A: Mild renal insufficiency A: Planned thyroid radio-ablation |
|
|
Precautions for patients on Metformin receiving IV contrast |
A: Stop Metformin for 48 hrs post-CT A: Check renal function prior to resumption 3: Causes ARF with lactic acidosis |
|
|
Four benefits of MRI for sinuses |
A: Differentiation of soft tissue involvement A: Differentiation of soft tissue from fluids A: Multiplanar capabilities with minimal patient movement A: No exposure to radiation |
|
|
Three limitations of MRI for sinuses |
A: Poor visualization of bony involvement A: Increased cost compared to CT scan A: Limitations due to metal |
|
|
Five general Advantages of MRI |
A: Better soft tissue definition than CT A: Multiplanar capability A: Clear delineation of arteries, veins, major cranial nerves A: Absence of ionizing radiation A: Absence of beam-hardening artifacts from dental implants |
|
|
Six General Disadvantages of MRI |
A: Prolonged data collection times A: Higher sensitivity to patient motion A: Contraindications – Pacemakers, certain Implants, Metallic foreign bodies A: Inferior bony detail A: Claustrophobia may prohibit examination A: Higher equipment cost & exam cost |
|
|
List 5 absolute and 4 relative Contraindications to MRI |
A: Pacemakers (most common) and Pacer-wires A: Swan-Gantz catheter A: Cochlear or Brainstem Implants A: Ocular (do xray) or Metallic foreign bodies A: Certain aneurysm clips A: Cardiac valve (relative, usually safe) A: Vascular clips (relative, usually safe) A: Orthopedic prosthesis (relative, usually safe) A: Claustrophobia (relative, premedicate) |
|
|
CT & MRI findings for Mycetoma |
A: Heterogeneous (double density) on CT A: Hypointense on T1/T2 |
|
|
CT & MRI findings for Allergic Mucin |
A: Hyperintense/heterogenous on CT A: Hypointense on T1/T2 – lack of water |
|
|
CT & MRI findings for Polyps |
A: Low density on CT A: Hypointense on T1, Hyperintense on T2 |
|
|
CT & MRI findings for Mucocele |
A: Typically hypointense on CT A: Variable pattern, depends on hydration; Hyperintense on T1 (when dehydrated), Hyperintense secretions on T2 with hypointense central area A: T1 w GAD: Generally does NOT enhance, but if enhancing will do so at periphery 3: Som and Curtin patterns of MRI signal intensity of mucous in CRS (Cummings): (1) Protein concentration < 9% → Hypointense on T1 and hyperintense on T2(2) Protein concentration of 20-25% → Hyperintense on T1 and hyperintense on T2(3) Protein concentration of 25-30% → Hyperintense on T1 and hypointense on T2(4) Protein concentration > 30% → Hypointense on T1 and T2 |
|
|
CT & MRI findings for Fibrous Dysplasia |
A: Featureless trabecular (ground glass) pattern on CT A: Hypo to Hyperintense on T1, T2 homogenous (like air) 3: Histology: Marrow-space replaced by irregular spindle-shaped mesenchymal cells forming whorled patterns and poorly developed bony trabecular with lack of osteoblastic rimming. |
|
|
Describe the 6 structures involved in the Ostiomeatal Unit |
A: Uncinate process A: Ethmoid Bulla and anterior ethmoid ostia A: Ethmoid Infundibulum A: Maxillary sinus ostium A: Frontal recess A: Middle turbinate |
|
|
Etiologic factors for the development of sinusitis, classified into 3 main categories |
A: Infectious – Viral, Bacterial, FungalA: Immune – Congenital, Acquired, Allergic A: Local – Craniofacial anomalies (Choanal atresia, VPI, Cleft palate), Trauma, Surgery, Dental, Ciliary, Anatomic |
|
|
Seven Anatomic variations influencing incidence of sinusitis |
A: Septal deviation and spur A: Conchal bullosa A: Paradoxical middle turbinate (Lateral convexity) A: Prominent ethmoidal bulla A: Pneumatization or deviation of the uncinate plateA: Prominent agger nasi cells A: Haller cells (Infraorbital ethmoids) |
|
|
Eight Congenital immune deficienciesA: Selective antibody deficiencies – IgA, IgG (IgG3 most common in RARS) |
A: Common Variable Immunodeficiency A: Severe Combined Immunodeficiency A: X-linked Agammaglobulinemia A: Complement deficiency A: Hyper IgM A: Hyper IgE/Job syndrome A: Ataxia-Telangiectasia A: Wiskott-Aldrich syndrome A: Digeorge syndrome |
|
|
Eight circumstances in which to screen for primary immunodeficiency |
A: >8 new ear infections per year A: >2 serious sinusitis per year A: >2 pneumonias per year, or bonchiectasis A: >2 months on antibiotics without improvement, or patient not responding to treatment as expected A: Recurrent deep skin or organ abscesses A: Persistent thrush after age 1 A: Failure to thrive A: Family history of PID A: Any patient with recurrent, unusual, severe infections |
|
|
Primary immunodeficiency screening workup (10) |
A: CBC and Differential A: T and B cell subsets A: T-cell stimulation tests – for candida A: IgM/A/G/E, with albumin & TP A: IgG subsets A: Specific antibodies – if titers low, Vaccine response A: C3, C4, CH50A: Special tests – Phagocytic tests for CGD |
|
|
Three important factors for normal nasal function |
A: Ostial patency A: Mucociliary function A: Quantity/quality of nasal secretions |
|
|
Timeframe of Rhinosinusitis |
A: Acute – 7-10d →<4 weeks (symptom-free interval if Recurrent) A: Subacute – 4-12 weeks (not used much anymore, can be grouped with acute or recurrent acute) A: Chronic – >8-12 weeks |
|
|
Six Major signs/symptoms of Rhinosinusitis |
A: Nasal obstruction A: Nasal discharge/PND A: Facial pain/pressure A: Hyposmia/Anosmia A: Purulence on examinationA: Fever (only in ARS) |
|
|
Seven Minor signs/symptoms of Rhinosinusitis (ABCDEFF) |
A: headAche A: Bad breath (Halitosis) A: Cough A: Dental pain A: Ear pain/pressure/fullness A: Fatigue A: Fever |
|
|
EPOS 2007 guidelines for diagnosis of Rhinosinusitis |
A: Inflammation of the nose and sinuses with 2 or more symptoms, one of which is either nasal congestion, obstruction, or anterior or posterior nasal discharge, AND +/- A: Facial pressure/pain A: Hyposmia/AnosmiaAND EITHERA: Endoscopic finding of polyps, middle meatal edema, mucosal obstruction A: CT evidence of mucosal changes in the OMC or sinuses |
|
|
The 2003 Task Force criteria for the Diagnosis of Chronic Rhinosinusitis |
A: Duration >12 weeks AND EITHER OF… A: Discolored discharge, polyp, polypoid swelling on anterior rhinoscopy or endoscopy A: Edema/erythema of the MM on endoscopy A: Edema/erythema/granulation in the nasal cavity, but if somewhere else than the MM, imaging is required A: Imaging confirmation (plain films or CT) |
|
|
Describe the Lund-Mackay CT Staging system |
A: Frontal sinus R & L A: Maxillary sinus R & L A: Anterior Ethmoid R & L A: Posterior Ethmoid R & L A: Sphenoid sinus R & L A: OMC R & L3: Scoring is 0 = clear, 1 = partial opacification, and 2 = total opacification; except for the OMC which is 0 = clear, and 2 = occluded, total score is 24. |
|
|
Six types of Fungal sinusitis classification |

A: Invasive: Acute/Fulminant invasive Immunocompromised pts Fungi: Mucorales order (Rhizopus, Rhizomucor, Absidia, Mucor) , Aspergillus fumigatus Tx: IV ampho b 1mg/kg/day (lipid based is more expensive, less nephrotoxic, can maintain higher doses), voriconazole or itraconazole if not mucor + ampho b nasal rises + aggressive surgical debridement + optimize immune status Chronic/Indolent invasive Limited or no immunocompromise Fungi same as acute but Aspergillus fumigatus more common (sources vary) Granulomatous invasive Limited or no immunocompromise Aspergillus flavus In Sudan areaA: Non-invasive: Allergic fungal – CRS with eosinophilic polyps can be divided into AFRS/EFS/EMRS/ECRS based on fungal cultures and IgE status (see below) Mycetoma – Fungal ball, Aspergillus fumigatus and dematiaceous fungi most common Saprophytic fungal infestation: fungus grows on crust and doesn’t involve mucosa * AFRS; allergic fungal RS, EFRS; eosinophilic fungal RS, EMRS; eosinophilic mucin RS, ECRS; eosinophilic CRS |
|
|
5 major diagnostic criteria for Allergic Fungal Sinusitis (Bent & Kuhn) |
A: Testing or history positive for fungal atopy (type I hypersensitivity) A: Nasal polyps A: Eosinophilic mucin with Noninvasive fungal hyphae A: Positive fungal smear A: CT scan with hyperdense material in sinus cavity and possible sinus wall erosion or expansion of the sinus cavity 3: Minor criteria:(1) Asthma(2) Unilateral predominance(3) Radiographic bone erosion(4) Positive fungal culture(5) Charcot Leyden crystals(6) Serum eosinophilia |
|
|
Four histopathologic findings of Eosinophilic Mucin in fungal sinusitis? |
A: Eosinophils A: Charcot-Leyden crystals (byproduct of eosinophil degranulation) A: Fungal elements & Hyphae A: Necrotic inflammatory cellular debris |
|
|
Kupferberg mucosal staging system for AFS |
A: Stage 0 – No edema or Allergic Mucin A: Stage I – Edema A: Stage II – Polypoid edema A: Stage III – Polyps 3: Suffix A – Without Allergic Mucin; Suffix B – With AllergicMucin |
|
|
Two histological findings with Allergic Rhinitis (from inferior turbinate) |
A: Increased ratio of columnar epithelium to goblet cells A: Increased number of eosinophils (>20% of granulocytes is suggestive of inhalant allergy) |
|
|
What fungi are most commonly seen in allergic fungal sinusitis? |
A: Aspergillus A: Demitaceous species (ABC) – Alternaria, Bipolaris, Curvularia, Cladosporium, Dreshleria, Exophilia, Fusarium 3: UT Southwestern Medical Center in Dallas, Texas study showed Bipolaris is the most common pathogens present, followed by Curvularia, Aspergillus then Alternaria |
|
|
Characteristics of Fungal Hyphae in Invasive fungal sinusitis |
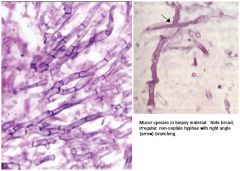
A: Mucor – Broad & ribbonlike (10-15 um), irregular/90 degree branching, rarely septated; order Mucorales in Zygomycetes class, most virulent and common is Rhizopus oryzae; more commonly seen in diabetic ketoacidotic patients A: Aspergillus – Narrow hyphae, regular septations, 45 degree branching; most virulent & frequent species found in those with invasive fungal sinusitis; typically A. fumigatus in North America; more commonly seen in immune compromised patients with neutropenia * Aspergillus on Lt, Mucor on Rt |
|
|
Diabetic patient with poor glycemic control, acute onset sharp R facial pain, opacification of right maxillary sinus with bony destruction; what is dx and what would you see on anterior rhinoscopy? |
A: Mucormycosis A: Necrosis of nasal mucosa, ischemic infarction, granular serosanguinous rhinorrhea; fungal hyphae may be seen A: Stains – Gomori methenamine silver (GMS), KOH, and PAS |
|
|
Name 4 genera of Mucormycosis |
A: Mucor A: Rhizomucor A: Rhizopus A: Absidia |
|
|
Etiologic agents in Acute Sinusitis |
A: Streptococcus pneumonia A: Hemophylous influenzae A: Moraxella catarhallis A: Streptococcus pyogenes A: Peptostreptococcus A: Fusobacterium A: Bacteroides |
|
|
Etiologic agents in Chronic Sinusitis (CCPG 2011) |
A: Main pathogens: S. aureus, Pseudomonas & Enterobacteriaceae A: Less common: Pneumococcus, H. influenzae, Beta hemolytic streptococci, Coagulase-negative Staphylococci A: Greatly increased role of anaerobes – Peptococcus, Bacteroides, Peptostreptococcus |
|
|
Treatment of Acute Rhinosinusitis |
A: Watchful waiting for 7 day IF Non-severe/mild pain, fever<38.3 C, followup ensured, able to re-evaluate if symptoms worsen; 5 adjunctive treatments: A: Double dose Mometasone spray A: Saline irrigations – No iodinated table salt as it inhibits ciliary action A: Mucolytics – Guaifenesin 1200 mg bid, or N-Acetyl Cysteine600 mg bid A: DecongestantsA: Analgesics 3: CPG 2011: Diagnosis requires the presence of ≥ 2 PODS, one of which must be O or D, and- Symptom duration of > 7 days without improvement- Biphasic worsening (better then worse between 5-7 days) or- Purulence for 3-4 days with high fever |
|
|
Antibiotic therapy for community-acquired bacterial sinusitis (CCPG 2011) |
A: Abx + INCS used if: Severe symptoms, mild-mod symptoms with no improvement on INCS in 72 hrs A: First-line: Amoxicillin In beta-lactam allergy: TMP/SMX or macrolide A: Second-line: Amoxicillin/clavulanic acid combination, or quinolones with enhanced gram-positive activity (ie, levofloxacin, moxifloxacin) For use if First-line therapy failed (defined as no clinical response within72 hours) Risk of bacterial resistance is high or Where consequences of therapy failure are greatest (ie, because of underlying systemic disease) A: High likelihood of resistance: exposure to antibiotics in the prior 3 months, exposure to daycare, and chronic symptoms. A: Duration of treatment should be 5 to 10 days as recommended by product monographs |
|
|
Indications for referral of ABRS cases as per CCPG 2011? |
• Persistent symptoms of ABRS despite appropriate therapy, or severe ABRS • Treatment failure after extended course of antibiotics • Frequent recurrence (≥4 per year) • Immunocompromised host • Evaluation for immunotherapy of allergic rhinitis • Anatomic defects causing obstruction • Nosocomial infections • Biopsy to rule out fungal infections, granulomatous disease, neoplasms. 3: IN CRS: Referral to a specialist is warranted when a patient Fails ≥ 1 course of maximal medical therapy or Has ≥ 4 sinus infections/year URGENT consultation w/otolaryngologist is required when a patient: Has severe symptoms of pain/swelling of the sinus areas, or Is immunosuppressed, or Suspect invasive fungal sinusitis |
|
|
What if the half-life of azithromycin? |
A: 68 hours |
|
|
Six Indications for Surgical intervention in acute bacterial sinusitis |
A: Severe pain A: Toxic A: Impending complications of sinusitis A: Nonresponse to medical therapy A: Immunocompromised patient A: >4 infections per year |
|
|
Five groups of mediators important in CRS and asthma |
A: Cells – Eosinophils, Th2 Lymphocytes A: Cytokines – Interleukins (IL-1B predominant, also -4, -5, -13),PAF, TNF A: Prostaglandins & Cysteinyl Leukotrienes A: Chemokines – RANTES, Eotaxin A: Adhesion Molecules – VCAM, ICAM, ELAM |
|
|
Seven Histopathologic findings in CRS |
A: Eosinophilic and Lymphocytic infiltration A: Major Basic Protein deposition A: Basement membrane thickening A: Subepithelial edema/fibrosis A: Goblet cell hyperplasia A: Mucous hypersecretion A: Submucosal gland formation |
|
|
What is the management of a frontal sinusitis and brain abscess in 10 year old? |
A: CT A: Neurosurgical consult A: Surgical debridement of sinuses A: IV antibiotics with good CSF penetration |
|
|
What are the frontal veins of Breschet in the frontal bone and what is their significance? |
A: Perforating veins connecting the intracranial and extracranial venous draining systems A: A potential pathway of hematologic spread of infection A: If not cleared in frontal sinus obliteration, can harbor mucosa and cause mucopyocele formation |
|
|
Sinusitis pathways of spread |
A: Hematogenous spread – Retrograde thrombophlebitis through valveless veins (veins of Breschet) A: Direct extension – Preformed pathways (eg. natural dehiscence of lamina) A: Direct extension – Traumatic/surgical pathways (eg. Traumatic dehiscence of lamina papyracea) A: Direct extension – Osteomyelitis (Pott’s puffy tumor) |
|
|
Describe Chandler classification of orbital complications in sinusitis |
A: Preseptal cellulitis A: Orbital cellulitis A: Subperiosteal abscess A: Orbital abscess A: Cavernous sinus thrombosis |
|
|
Organisms seen in orbital/periorbital cellulitis |
A: H. influenzae A: S. aureus A: S. pneumoniae A: S. pyogenes A: Bacteroides species A: Peptostreptococcus A: Veionella |
|
|
Nine indications of the Caldwell Luc procedure |
A: Chronic maxillary Sinusitis, or disease refractory to endoscopic surgery A: Maxillary sinus foreign body, Tumor, Mycetoma, Multi septate Mucocele, or Antrochoanal polyp A: Approaches to Pterygomaxillary space (Imax ligation, Vidian neurectomy, biopsy of skull base lesions) A: Repair of Oroantral Fistula A: Repair of Trauma A: Orbital Decompression of Grave’s ophthalmopathy |
|
|
Six complications of the Caldwell Luc procedure |
A: Cheek edema & ecchymosis A: Dysesthesia of infraorbital n. distribution A: Epiphora A: Oroantral fistula A: Antral scarring A: Bone thickening |
|
|
Six indications of External Frontoethmoidectomy |
A: Frontoethmoidal mucopyocele A: Orbital complication of sinusitis A: Revision surgery with absent or distorted landmarks A: CSF leak repair A: Biopsy of Anterior skull base lesion – Frontal, orbital, or ethmoid lesion A: Access to the anterior ethmoid artery |
|
|
Twelve complications of External Frontoethmoidectomy |
A: CSF leakA: Intracranial hemorrhage A: Bleeding/crusting A: Orbital hemorrhage A: Diplopia or blindness A: Telecanthus A: Epiphora A: Persistent or Recurrent disease A: Mucocele A: Stenosis/Synechiae of Frontal Recess with Frontal sinusitis A: Scarring/Keloid formation A: Forehead dysesthesia |
|
|
Medial Maxillectomy is the En-bloc resection of what 5 structures? |
A: Medial Maxillary sinus wall (middle/inf turbinates)
A: Ethmoid sinuses A: Lamina papyracea A: Medial Orbital floor A: Lacrimal bone |
|
|
Indication and 4 Contraindications for Medial Maxillectomy |
A: Indication – Benign or low grade malignant tumors confined to the lateral nasal wall, maxillary antrum, and/or ethmoid sinus A: Contraindications – Invasive malignancies extending intracranial, to the pterygoid plates, palate, or extensively into the orbit |
|
|
Six complications of Medial Maxillectomy |
A: Facial neuralgia/Dysesthesia A: Epiphora/Dacryocystitis A: Telecanthus A: Diplopia (may be transient) A: Nasal collapseA: Mucocele |
|
|
Major landmarks along the medial orbital wall |
A: Blood vessels found along the frontoethmoidal suture, which divides the ACF from the ethmoid sinuses A: Anterior Ethmoid artery ~16 (14-22) mm posterior to the anterior lacrimal crest (maxillolacrimal suture) A: Posterior Ethmoid artery ~10 (10-12) mm posterior to the anterior ethmoid artery A: Optic nerve ~6 (4-7) mm posterior to the posterior ethmoid artery |
|
|
Three approaches to a frontal mucocele, advantages & disadvantages of each |
A: Lynch frontoethmoidectomy – Ethmoidectomy plus removal of entire frontal sinus floor A: Osteoplastic flap – Advantage = Eradication of disease and mucosa; Disadvantage = requires coronal or mid-forehead approach, disfiguring, high rate of mucocele recurrence A: Endoscopic – Advantage = All intranasal; Disadvantage =Cannot access sinuses to eradicate mucosa, limited access laterally |
|
|
Six indications for Osteoplastic Flap of the frontal sinus
|
A: Chronic frontal sinusitis with persistent intractable symptoms, sepsis, or other complications despite previous intervention A: Mucocele with Orbital or Intracranial extension A: Osteomyelitis A: Frontal sinus tumor A: Frontal sinus fracture with comminuted anterior table or displaced posterior table A: CSF leak |
|
|
Four contraindications for Osteoplastic Flap Obliteration of the frontal sinus |
A: Hyperpneumatized supraorbital ethmoid cells A: Fungal sinusitis A: Inverting papilloma or other frontal sinus tumor A: Posterior frontal table or orbital roof dehiscence |
|
|
Five historical open frontal sinus procedures |
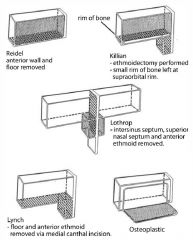
A: Reidel – Removal entire floor & anterior wall of frontal sinus; significant cosmetic deformity A: Killian – Combination of Reidel and Lynch; removal of floor and anterior wall, retain frontal bar A: Lynch – Ethmoidectomy plus removal of entire frontal sinus floor, and part of the lamina papyracea A: Lothrop/Chaput-Mayer – Superior nasal septum and inner sinus septum taken down A: Osteoplastic Flap – Anterior wall frontal sinus based inferiorly retracted and replaced with periosteum intact |
|
|
Describe the Draff classification for endoscopic frontal sinus drillout procedures |
A: Type I – Removal of obstructing disease inferior to frontal ostium, includes removal of anterosuperior ethmoid cells without altering the ostium; indicated for minor pathology, in patient without adverse prognostic risk factors (ASA intolerance, asthma, NP, etc.) A: Type IIa – Extended drainage with ethmoidectomy and resection of the floor of the frontal sinus between the lamina papyracea and the middle turbinate; uncapping the egg A: Type IIb – Extended drainage with ethmoidectomy and resection of the floor of the frontal sinus between the lamina papyracea and the nasal septum, anterior to the ventral margin of the olfactory fossa A: Type III – Endonasal median drainage, the extended IIb opening is enlarged by resecting portions of the superior nasal septum in the neighborhood of the frontal sinus floor (diameter should be ~1.5 cm), followed by resection of the frontal sinus septum; this results in an opening from lamina papyracea to contralateral lamina papyracea 3: The AP diameter of the frontal sinus should be ≥8 mm to undergo a Draff III, otherwise an osteoplastic flap should be considered |
|
|
Ten Surgical approaches to the sphenoid sinus |
A: Transantral A: Transpalatal – Ideal for tumors involving the nasopharynx, posterior pharyngeal wall, and choanae A: Transseptal – Sublabial, Intranasal, External rhinoplasty A: Transethmoidal – Internal, External A: Endoscopic – Transnasal, Transethmoidal, Transantral |
|
|
Four anterior to posterior bony lamina encountered in ESS |
A: Uncinate process A: Ethmoid bulla A: Vertical portion of the basal lamella of the middle turbinate A: Lamella of the Superior turbinate 3: Additional answers may include the Supreme turbinate, andAnterior wall of sphenoid sinus |
|
|
Four bony components of the Medial Orbital Wall |
A: Frontal process of the Maxilla A: Lacrimal bone A: Lamina papyracea of the Ethmoid A: Sphenoid bone (just anterior to the optic canal) 3: Orbital process of palatine bone is also near the apex (more inferior than lateral?) |
|
|
Which anatomic sinus variation is more common in Asians |
A: Sphenoethmoidal/Onodi cells |
|
|
What are the four sides of Bolger’s parallelogram? |
A: Lamina papyracea A: Skull base A: Superior turbinate A: Basal lamella of SUPERIOR turbinate |
|
|
Your postop ESS patient develops a postoperative orbital hematoma. What are your management considerations? |
A: Fast (arterial) (15-30 min) vs. slow (venous) hematoma formation (60-90 min); Proptosis, pupil changes, vision loss indications for immediate surgical intervention A: Medical treatment (5) Urgent Ophthalmology consultation and assess vision Remove packing and suction at bleeding site Mannitol 1-2 g/kg in 20% IV infusion (100 g in 500 cc bag) over 20 minutes Acetazolamide 500 mg IV q4h prn Timolol 0.5% ophthalmic drops (only if slow bleed) Steroids (controversial) Orbital massage (controversial)A: Surgical treatment (4) Lateral canthotomy/cantholysis Medial external (Lynch) decompression Endoscopic decompression 3: If anterior or posterior Ethmoid artery is suspected, Kennedy recommends postop CT sinus to R/O concomitant skull base injury |
|
|
Describe the 7 features of superior orbital fissure syndrome |
A: Orbital pain A: Photophobia A: Proptosis A: Ophthalmoplegia A: Failure of accommodation A: Upper eyelid paralysis A: Forehead paresthesia/hypoesthesia 3: Caused by sphenoid sinusitis, neoplasm, trauma; Involves CNIII, IV, V1, VI; Differs from Orbital apex syndrome in that CN II usually not involved as it is in its own canal |
|
|
Discuss Cavernous Sinus Syndrome |
A: Cause – Ethmoiditis, 80% mortality rate A: Symptoms – Orbital pain (V1), Proptosis, Photophobia, Ophthalmoplegia (CN III, IV, VI involvement), venous congestion of retina, lids, conjunctiva A: Treatment – Antibiotics, Anticoagulation 3: Similar to superior orbital fissure syndrome, except for additional involvement of venous system |
|
|
Name the 4 structures visible on the walls of the sphenoid sinus (top to bottom)? |
A: Optic nerve – Projects into sinus less commonly, ~50%; bone dehiscent in ~4-6% A: Optico-carotid recess A: Internal carotid artery – Medial deflection into lateral wall called the carotid sulcus, present 65-98% of time; bone dehiscent in ~7-22% A: V2A: lateral recess between V2 and vidian A: vidian nerve |
|
|
Six anatomic relationships of the Sphenoid Ostium |
A: 7 cm from the Anterior Nasal Spine A: 30o angle from the floor of the nose (Pasha: most reliable) A: 1-1.5 cm above the upper limit of the choana A: 1/3 up from the choana to the skull base A: Adjacent the posterior border of the nasal Septum (2-3 mm) A: Inferomedial to the posterior attachment of the Superior Turbinate on sphenoid face (Parson’s ridge) |
|
|
Six useful landmarks for Revision ESS |
A: Skull base A: Superior attachment of Middle Turbinate A: Sphenoid sinus ostium A: Maxillary ostium A: Roof of maxillary sinus A: Lamina papyracea |
|
|
Internal carotid artery branches supplying the internal nose |
A: Anterior Ethmoid artery A: Posterior Ethmoid artery 3: Branches off the ophthalmic artery, each divides into a medical branch (Little’s area & septum) and a lateral branch (superior & middle turbinates) |
|
|
External carotid artery branches supplying the internal nose |
A: Sphenopalatine artery – Lateral posterior nasal artery (supplies lateral nasal wall), and Septal posterior nasal artery (across anterior sphenoid and along septum up to Little’s area) A: Descending Palatine artery – Splits into lesser and GreaterPalatine arteries (the latter supplies Little’s area in the septum & floor of nose through the Incisive branch) A: Septal branch of Superior Labial artery – Supplies the Septum and Ala A: Pharyngeal branch – Supplies posterior nose & nasopharynx 3: All are terminal branches of the internal maxillary artery except the superior labial artery, which is a branch off the facial artery |
|
|
Describe the Venous drainage of the nose |
A: Greater Palatine vein – Posterior Facial vein, into ExternalJugular vein A: Septal and Angular veins – Anterior Facial vein, into InternalJugular vein A: Anterior and Posterior Ethmoidal veins – Ophthalmic vein, toCavernous sinus, into Internal Jugular vein A: Sphenopalatine vein – Maxillary vein, to Cavernous sinus, into Internal Jugular vein |
|
|
Describe the two nasal vascular arterial plexuses and their blood supply |
A: Kiesselbach’s plexus – Little’s area, found on the anterior septum (Anterior ethmoid, Sphenopalatine, Greater palatine, andSuperior labial arteries) A: Woodruff’s plexus (naso-nasopharyngeal plexus) – Venous, located in the posterior lateral nasal wall inferior to the InferiorTurbinate |
|
|
Management of Epistaxis |
A: Non-surgical (5) Topical decongestion Cauterization – silver nitrate, electrocautery Packing – Absorbable vs. nonabsorbable, anterior, posterior, combined, balloon packs Greater palatine canal injection Radiologic Embolization of internal maxillary & facial arteries A: Surgical (4) Sphenopalatine artery ligation – Transantral vs. Endoscopic Ethmoid artery ligation – Lynch frontoethmoidectomy approach vs. Endoscopic Maxillary artery ligation – Transantral External carotid artery ligation |
|
|
Name the most important landmark for performing and Endoscopic Sphenopalatine artery ligation |
A: The Crista Ethmoidalis, part of the perpendicular process of the Palatine bone |
|
|
What 2 vessels must be ligated in a transantral maxillary artery ligation to prevent recurrent epistaxis from collaterals? |
A: Sphenopalatine artery A: Descending palatine artery |
|
|
Complications of posterior nasal packing |
A: Airway obstruction & exacerbation of OSA A: Dyspnea A: Nasopulmonary reflex – Bronchoconstriction, hypoxemia, apnea, and cardiac dysrhythmia A: Sinusitis A: Otitis media A: Toxic shock syndrome A: Septal or alar necrosis |
|
|
Discuss Osler Weber Rendu syndrome/Hereditary Hemorrhagic Telangiectasia |
A: Definition – Autosomal dominant disorder characterized by ectatic vessels of the skin, mucous membranes, and viscera A: Diagnosis – The Curacao criteria, published in 2000, remain the mainstay of HHT clinical diagnosis: Recurrent, spontaneous nosebleeds Mucocutaneous telangiectases at characteristic sites (fingertips, lips, oral mucosa, tongue) Visceral AVMs (gastrointestinal, pulmonary, hepatic, cerebral, or spinal) Family history (first-degree affected relative)Definite HHT = 3 or 4 criteriaPossible HHT = 2 criteriaUnlikely HHT = 0 or 1 criteria A: Cause – Mutation in the Endoglin protein, a receptor for TGF beta, which has a role in tissue repair and angiogenesis, leading to the development of abnormal vasculature, chromosome 9 A: Clinical – Triad of Telangiectasias, recurrent Epistaxis, and a positive Family History for the disorder; may also have pulmonary, GI & CNS bleeds A: Complications – Morbidity and mortality due to multiorgan arteriovenous malformations, and associated hemorrhages A: Treatment – Manage anemia/acute bleeds; septal dermoplasty for epistaxis, laser, Young’s procedure, septectomy? |
|
|
CSF leak anterior skull base – Size of defect that is suitable for a) mucosa only coverage and b) composite (multilayer) coverage |
A: <3 or 5? mm mucosal defect A: >3 or 5? mm mucosal or >2 cm bony defect |
|
|
Ddx of CSF rhinorrhea |
A: Iatrogenic A: Blunt trauma (closed HI or skull fractures) A: Increased ICP – Tumors, Post-infectious, Post-trauma,Hydrocephalus A: Arachnoid granulations A: Encephalocele A: CSF otorrhea via ET 3: Consult Neurosurgery for all cases of spontaneous CSF leak in order to R/O elevated Intracranial Pressure |
|
|
Diagnostic tests for CSF leak |
A: Clinical – Halo signA: Chemistry – Glucose (≥5 mg/dl), beta-2 transferrin, beta-trace proteinA: Endoscopy +/- ValsalvaA: High resolution CT with coronal and sagittal reconstructionsA: CT or MR CisternographyA: Intraoperative intrathecal fluorescein – 0.1 cc of 10% fluorescein in 10 cc of CSF, slowly infusedA: Radionucleotide scanning or scintiphotography |
|
|
List 5 Complications of intrathecal fluorescein |
A: Generalized Seizures A: Opisthotonus (hyperextension and spasticity) A: Lower limb weakness/paresthesias A: Headache A: Cranial nerve deficits |
|
|
Three approaches for CSF leak repair |
A: Intracranial A: Extracranial external A: Endoscopic 3: Can be Overlay or Underlay (>5 mm) 3: Postop care = 24 hrs bed rest, HOB elevated, lumbar drain, no nose blowing, no straining, stool softeners at 10 cc/h for 24-48 hrs may be used |
|
|
Four neural systems of nose |
A: CN 0 (nervus terminalis) – Loose plexus of fine nerve fibers throughout the nose; high GnRH content A: CN I: olfactory A: CN V: nasociliary (V1); Nasopalatine (V2); Maxillary nerve (V2)A: Vomeronasal Organ (VNO) – Rudimentary, non-functioning in humans A: Vidian nerve: sympathetics/parasympathethics |
|
|
Four Complications of Nasal Folliculitis and Furuncle |
A: Septal chondritis A: Septal abscess A: Saddle-nose deformity A: Cavernous sinus thrombosis 3: Infections of hair follicle caused by Staph aureus or Strep |